Transcription
Information Meeting on ZELBORAF and cobas BRAF V600 Mutation TestCHUGAI PHAMACEUTICAL CO., LTD.Roche Diagnostics K.K.April 2, 2015
Forward-Looking StatementsThis presentation may include forward-looking statements pertaining to thebusiness and prospects of Chugai Pharmaceutical Co., Ltd. (the“Company”). These statements reflect the Company’s current analysis ofexisting information and trends.Actual results may differ from expectations based on risks anduncertainties that may affect the Company’s businesses.Although this presentation includes information regarding pharmaceuticals(including products under development), the information is not intended asany advertisement and/or medical advice.1
Overview of ZELBORAF Takahiro MizuiZELBORAF Lifecycle LeaderCHUGAI PHARMACEUTICAL CO., LTD.
Outline of ZELBORAF ZELBORAF is a small molecule compound thatselectively inhibits oncogenic BRAF kinase,developed by F. Hoffmann-La Roche Ltd. and Plexxikon Inc. Nonproprietary name: Vemurafenib (JAN)Structural formula Molecular weight: 489.92 Chemical name: de3
Development history of ZELBORAF Month/YearGlobalNov/2006 Roche and Plexxikon Started Phase Istudy (PLX06-02 [BRIM1])Sep/2009 Started Phase II study (NP22657[BRIM2])Jan/2010 Started Phase III study (NO25026[BRIM3])Aug/2011 Approval for the patients withunresectable or metastatic melanomawith BRAF V600E mutation in USFeb/2012 Approval for the patients withunresectable or metastatic melanomawith BRAF V600 mutation in EUJapanSep/2012 Chugai Started Phase I/II study (JO28178) Orphan drug designationApr/2014 New drug application filed for vemurafenibDec/2014 Approval for the patients withunresectable melanoma with BRAFmutationBRAF mutation should be determined by cobas 4800 BRAF V600 Mutation Test. The cobas 4800 BRAF V600 Mutation Test hasbeen approved as the companion diagnostics in the US (Aug. 2011), and CE-marked in the EU (Aug. 2011).4
Selectivity against V600 mutated BRAF kinase(in vitro) Kinase inhibitory activity of vemurafenibagainst various kinasesKinaseIC50 (nmol/L) Kinase inhibitory activity of vemurafenibagainst V600 mutated BRAF ol/L)BRAF V600E8CRAF16V600E*Baculo1009, 9.9ARAF29V600A*Baculo10027, 14BRAF WT39V600DE. coli1005SRMS18V600GBaculo1008ACK119V600KE. coli10110MAP4K5 (KHS1)51FGR63V600KBaculo1007BRK202V600ME. coli10013LCK218V600MBaculo1007NEK11317V600RE. coli1034FYN533V600RBaculo1009KIT538K601EE. 877STK3 �� Result from 2 in vitro studiesChugai Internal Document5
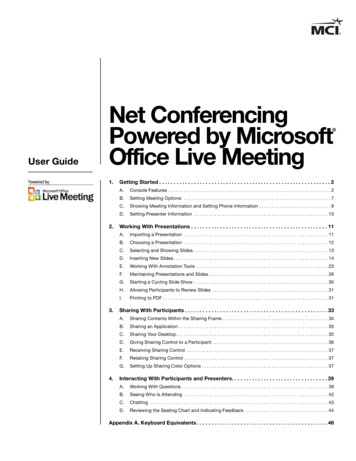
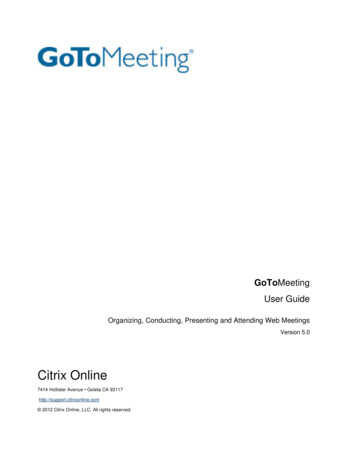
The mechanism of antitumor activity of vemurafenib intumor cells with mutant BRAF V600Normal signalingvia RAS-BRAF1)Growth factorSignaling in tumor cells withmutant BRAF V6002, 3)Inhibitory activity of vemurafenbagainst the tumor cellswith mutant BRAF V6003-5)RAS-GTPReceptor tyrosinekinaseBRAFBRAF V600BRAF V600MEKMEKMEKERKERKERKNormal cellularsurvival/proliferationPromoted cellularsurvival/proliferationInhibited cellularproliferation &elevated apoptosisvemurafenibConceptualillustration1) Garnett MJ, et al. Cancer Cell 2004, 6: 313-319 2) Wan PTC, et al. Cell 2004, 116: 855-8673) Poulikakos PI, et al. Nature 2010, 464: 427-4304) Bollag G, et al. Nature 2010, 467: 596-5995) Yang H, et al. Cancer Res 2010, 70: 5518-55276
Description Regulatory classificationPowerful drug, Prescription-only drug** Caution - Use only pursuant to the prescription ordirections of a physician, etc. StorageStore at room temperature; protect frommoisture (ZELBORAF should be stored in itsoriginal PTP packaging) Expiration date2 years (Use before the expiration dateindicated on the carton)Long axisShort axisThicknessWeightapprox. 19.1 mmapprox. 9.7 mmapprox. 7.4 mm870 mgPackage Insert: Dec. 2014 (Version 1)7
Indications【INDICATIONS】Unresectable melanoma with BRAF mutation Precautions related to INDICATIONS 1. ZELBORAF should be administered only in patients confirmed to be BRAFmutation-positive through tests by an adequately experienced pathologistor test facility.The test should be conducted using an approved in vitro diagnostic.2. Eligible patients should be selected after carefully reading the CLINICALSTUDIES section to gain a thorough understanding of the effectivenessand safety of ZELBORAF.3. The effectiveness and safety of ZELBORAF as post-operative adjuvantchemotherapy have not been established.Package Insert: Dec. 2014 (Version 1)8
Dosage and administration【DOSAGE AND ADMINISTRATION】The usual adult dosage of vemurafenib is 960 mg administeredorally twice daily. Precautions Related to DOSAGE AND ADMINISTRATION 1.If an adverse reaction occurs, the dose should be modified with reference to Table1. However, if cutaneous squamous cell carcinoma or new primary melanomaoccurs, treatment can continue without dose reduction or interruption after thepatient receives appropriate intervention, such as surgical resection. In patientswho develop QTc prolongation, the dose should be modified with reference toTable 2.2.Increased Cmax and AUC has been reported with postprandial administration ofZELBORAF. To avoid the food effect, dosing is preferable in a fasted state (fasting2 hours before and 1 hour after dose) (see PHARMACOKINETICS).3.The effectiveness and safety of ZELBORAF in combination therapy with otheranti-cancer drugs have not been established.Please refer to the package insert about “Table1” and “Table2.”Package Insert: Dec. 2014 (Version 1)9
Conditions for approval1. A drug risk management plan should be prepared andappropriately implemented.2. Because the number of patients in Japanese clinical trials isvery limited, postmarketing drug use surveillance of allpatients receiving ZELBORAF should be conducted untildata for a set number of patients are collected in order toidentify the background characteristics of patients usingZELBORAF, collect early data on the safety and efficacy ofZELBORAF, and take necessary measures for appropriateuse of ZELBORAF.Package Insert: Dec. 2014 (Version 1)10
cobas BRAF V600 Mutation TestToru OgawaManager, Molecular DiagnosticsRoche Diagnostics K.K.11
Companion Diagnostics”cobas BRAF V600 Mutation Test” isa companion diagnostic for “Zelboraf ”RUO; Research Use OnlyIVD; in vitro diagnosticsCoDx; Companion Diagnostics identify patients who are most likely to benefit from a particular therapeutic product identify patients who are likely to be at increased risk for serious side effects as a result oftreatment with a particular therapeutic product monitor response to treatment with a particular therapeutic product for the purpose ofadjusting treatment to achieve improved safety or effectiveness12
cobas BRAF V600 Mutation TestTo aid in the selection of patients for therapy withZelboraf Zelboraf ?Unresectable Malignant Melanomacobas BRAF V600Mutation TestOnly cobas BRAF Mutation Test can be used for the identification of patientsfor therapy with Zelboraf .13
Extracts from Package insert cobas BRAF V600 Mutation Test【intended use】Detection of BRAF V600 mutationsin DNA extracted from formalin-fixed,paraffin-embedded human melanoma tissue (an aid in selecting melanoma patients whosetumors carry the BRAF V600E mutation for treatment with vemurafenib) Zelboraf Tablets【Precautions Related to INDICATIONS】ZELBORAF should be administered only in patients confirmed to be BRAF mutation-positivethrough tests by an adequately experienced pathologist or test facility. The test should beconducted using an approved in vitro diagnostic.【CLINICAL STUDIES】Note 8: Tested using a cobas BRAF V600 Mutation Test kit, the approved companiondiagnostic.Package insert “cobas BRAF V600 Mutation Test”Package insert “Zelboraf”14
Reagents and System for Diagnosticscobas DNA SamplePreparation Kit(FFPE)DNA Extractioncobas BRAF V600Mutation Testcobas 4800 Systemz480Reagent for Amplificationand DetectionSystem15
cobas BRAF V600 Mutation TestSpecificationcobas BRAF V600 Mutation TestIntended UseMutation CoverageSpecimen TypeDetection of BRAF V600 mutationsin DNA extracted from formalin-fixed,paraffin-embedded human melanoma tissue (an aid in selectingmelanoma patients whose tumors carry the BRAFV600E mutation for treatment with vemurafenib)Exon 15 codon 600formalin-fixed, paraffin-embedded tissue (FFPET)DNA Volume125 ng/SampleMethodReal-time PCRSensitivityInstrumentThroughput/runcobas 4800 BRAF V600 Mutation Test can detect the BRAF V600Emutation in actual clinical FFPET specimens at 5% mutation levelcobas 4800 z480 v2.194 samples (8 batch/kit)Package insert “cobas BRAF V600 Mutation Test”16
Detection:The detection of exon 15, codon 600 in BRAF geneBRAF gene123131415ExonIntroncodon600Most of malignant melanoma is the mutation of codon 600 V(Val) to E(Glu), D(Asp),and K(Lys).cobas BRAF V600 mutation kit could cross react to D and K in addition to E.Roche Diagnostics Document17
4 key stepsStep 1Step 2(1) H&E staining& tumor contentdeterminationMacro-dissect, if 50% tumor content byareaGenomicDNA isolationDNAquantificationStep 3Step danalysisPCR setupHarkanwal Halait, et al, Diagn Mol Pathol Volume 21, Number 1, March 201218
ReportTest results are automatically reported.Basic informationDate, Lot.Control resultMeasurement result19
Doing now what patients need next20
ZELBORAF tabletPostmarketing safety measuresShin YoshidaPharmacovigilance DepartmentCHUGAI PHARMACEUTICAL CO., LTD.21
Contents1. Reasons for implementing safety measures2. Safety measures based on post-approval commitments(PACs)– Implement safety measures on the basis of the risk managementplan (RMP)– Implement postmarketing surveillance for all patients treated3. Other approaches for safety measures4. Summary22
1. Reasons for implementing safety measures Only a very small number of patients were studied in Japanese clinicaltrials. Only 11 patients received the clinical dose during the Japanese Phase I/II clinical trial.Therefore, it is necessary to identify demographic characteristics of patients givenZelboraf, collect data at an early stage on the safety and efficacy of Zelboraf, andtake necessary measures for the appropriate use of Zelboraf. Serious adverse drug reactions (ADRs), such as squamous-cellcarcinoma and QT interval prolongation, may occur. It is necessary to reliably provide healthcare professionals and patients withinformation on the appropriate use of Zelboraf, such as ADR incidence and actions totake when ADRs occur.It is necessary to set use requirements to ensure that Zelboraf will only beadministered under the care of medical institutions and physicians who arethoroughly familiar with chemotherapy and can adequately control any risksassociated with Zelboraf.Strict postmarketing safety measures are necessary for theappropriate use of Zelboraf.23
1. Reasons for implementing safety measuresPackage Insert: WARNINGS【WARNINGS】Zelboraf should be administered only in patients who are deemedsuitable for treatment, in a medical facility adequately equipped todeal with emergencies, and under the supervision of a physician whois knowledgeable and experienced in cancer chemotherapy. Beforetreatment is started, patients or their families should be provided witha full explanation of the benefits and risks of Zelboraf. Zelboraf shouldbe administered only after informed consent has been obtained.Package Insert: CONTRAINDICATIONS【CONTRAINDICATIONS (Zelboraf is contraindicated in the followingpatients.)】Patients with a previous history of hypersensitivity to any of theingredients of Zelboraf.24
2. Safety measures based on PACs Implement safety measures on the basis of the RMPRMPs should be planned and appropriately implemented. Implement postmarketing surveillance for all patientstreatedOnly a very small number of Japanese patients were treatedduring the clinical trials. Therefore, from product launch untildata on a given number of patients have been accumulated,the MAH should conduct drug use surveillance in all patients,thereby identifying the background characteristics of patientsgiven Zelboraf and collecting early data on the safety andefficacy of Zelboraf, and should take the measuresnecessary for the appropriate use of Zelboraf.25
2. Safety measures based on PACsRMPSafety specificationImportant identified risks Squamous-cell carcinoma Secondary malignancies other thansquamous-cell carcinoma Liver disorder Photosensitivity QT interval prolongation Skin disorder Hypersensitivity Eye disorder (Uveitis, etc.)Important potential risks Progression of malignancies with RAS genemutation Facial nerve paralysis Myelosuppression Gastrointestinal polypImportant missinginformation None26
2. Safety measures based on PACs-Implement safety measures on the basis of the RMPRMPRisk minimization activitiesRoutine Early postmarketing phase vigilance(EPPV) Special drug use surveillance (allpatient) Postmarketing clinical studies JPI creation (revision) Patient Guide creation (revision)AdditionalRoutine1) Collection and evaluation ofindividual cases2) Research report (literature, etc.)3) Report on safety actions takenoverseas4) Periodic SAE signal detection andassessmentAdditionalPharmacovigilance activities Provide information via EPPV Provide healthcare professionals withinformation(Appropriate Use Guide) Provide patients with information(Patient Handbook)27
2. Safety measures based on PACs-Implement safety measures on the basis of the RMPProductlaunchApprovalPharmacovigilance activities: EPPVDeliveryMR visit, briefing,and request forcooperationbefore delivery2 weeks afterdelivery6 months afterproduct launchRequests for cooperation, and regular(once/2 weeks) provision of informationand raising of precautions by Chugai MRs Implement for 6 months after product launch MRs regularly visit medical institutions to collect information onADRs and provide periodic information.28
2. Safety measures based on PACs-Implement safety measures on the basis of the RMPRisk minimization activities: Information provisionMaterials for healthcare professionalsMaterials for patients29
2. Safety measures based on PACs-Implement postmarketing surveillance for all patients treatedSurveillanceobjectivesTo determine the following items under the conditions of actual clinical use ofZelboraf during a long-term follow-up period (24 months) Incidence of ADRs Unlabeled ADRs Overall survival Factors thought to affect safety and effectivenessTarget patientsAll patients who use Zelboraf during the enrollment periodEvents ofinterestSquamous-cell carcinoma, secondary malignancies other than squamous-cellcarcinoma, QT interval prolongation, liver disorder, skin disorder, andhypersensitivityTargetSurveillancesample size500 patientsPatientEnrollmentperiodFor 72 months after product launch(Even after the target sample size is reached, patient enrollment will becontinued until lifting of the PAC on all-patient surveillance.)30
3. Other approaches for safety measures Confirmation of requirements forinstitutions/physicians planning to use Zelboraf Careful selection of patients for treatment Use of Zelboraf Emergency Contact Card31
3. Other approaches for safety measuresConfirmation of requirements for institutions/physicians planning to use ZelborafInstitution requirements1. Understand and cooperate with the safety measures specified for Zelboraf.2. Be able to appropriately provide urgent transportation and emergency treatment if a patient's condition suddenly deteriorates, etc.3. Be able to perform ECG, provide cardiovascular diagnosis or evaluation, and provide appropriate emergency treatment on site orat an affiliated medical institution.4. Be able to provide ophthalmologic diagnosis or evaluation and appropriate treatment on site or at an affiliated medical institution.5. Be staffed by physicians belonging to the Japanese Skin Cancer Society or skin cancer specialists who can engage in treatment.6. Be able to appropriately perform surgical resection or histopathological diagnosis on site or at an affiliated medical institution ifcutaneous malignancies, including squamous-cell carcinoma, occur during Zelboraf treatment.7. Be able to perform the BRAF gene mutation test approved as an in-vitro test, on site or at an affiliated medical institution.8. Be able to perform the following tests, etc., for evaluation or diagnosis of secondary malignancies on site or at an affiliatedmedical institution.(CT scan, radiography, MRI, gastrointestinal endoscopy, head and neck screening, and gynecological examination)Physician requirements1. Be able to accommodate routine visits from Chugai Pharmaceutical Co., Ltd. MRs.2. Be able to cooperate with necessary safety measures for Zelboraf.3. Possess adequate experience in surgery or chemotherapy for malignant melanoma.32
3. Other approaches for safety measuresCareful selection of patients for treatmentAll patients who will use Zelborafshould be enrolled before drugadministrationConfirm patient eligibilityRaise precautions by informing theprescribing physician about thepackage insert contents if necessaryAll-patient surveillance33
3. Other approaches for safety measuresUse of Zelboraf Emergency Contact CardThis card must be shown when Zelboraf is dispensed. Physicians are requestedto provide patients with this card when Zelboraf is prescribed.[Front: ADRs that need to be reported at onset][ Back:Emergency contact details]34
4. Summary Reasons for implementing safety assurancemeasures Only a very small number of patients were studied inclinical trials in Japan. Serious ADRs may occur. Approaches for safety assurance Safety measures based on PACs Implement safety measures on the basis of the RMP Implement postmarketing surveillance for all patientstreated Other approaches for safety measures35
Overview of melanoma andclinical trials of vemurafenibNaoya Yamazaki, M.D., Ph.D.Chief, Dept. of Dermatologic OncologyNational Cancer Center Hospital, Japan36
Characteristics of main skin cancerBasal cellcarcinomaSquamous cellcarcinoma Usually caused by UV ray exposure and occur frequently on the facein the elderly Rarely spread to other parts of the body and become lifethreatening Generally treated by surgical excision Malignant growth of epidermal keratinocytesOccur frequently on the sun-exposed areaNecrosis and ulceration accompanying malodor in hard nodeTreatment options are surgical excision, lymph node dissection,radiation therapy and chemotherapy Solar keratosis or Bowen’s disease is popular genesisMalignantmelanoma Lymphogenic metastasis, hematogenous metastasis Although melanoma accounts for only 4% of all skin cancers, 80% ofthe patients who die from skin cancers have melanoma, thus it is ahighly malignant form of carcinoma Treatment options are surgical excision, radiation therapy,chemotherapy, molecular-targeted therapy and immunotherapyPaget diseaseexcl. breast Intraepidermal carcinoma derived from apocrine gland Occur frequently on the vulva, anal region and axilla Generally treated by surgical excisionAtarashii hifukagaku version2 (Nakayama shoten) 2011, p422-430, 433-436, 457, tabularisation37
Number of New Cases/Deaths of Melanomaby Race/EthnicityMale27.732.31.01.52.01.00.41.2Asian /Pacific Islander0.44.10.34.0American Indian /Alaska ic4.41020.0Black0.5201.7White4.63016.7All Races4.1(%) 40Female(person/100,000・year)0New Case (2007-2011)1.8010203040 (%)Death (2006-2010)SEER18 Registry data set analyzed by SEER Stat ver8.0.1SEER Stat Fact Sheets: Melanoma of the Skin l)38
Number of deaths of melanoma patients in Japan700(Total number of deaths from 1972-2013)Male(8,448)Female 0820092010201120122013Number of deaths600Statistics and Information Department, MHLW, Vital Statistics, 1972 201339
Incidence rates of melanoma by Stage (UICC, 2002)UnresectableStageTis11%18%Stage IaStage Ib9%Stage ⅡaStage ⅡbResectableStage8%13%Stage ⅡcStage ⅢaStage Ⅲb4%Stage Ⅲc9%9%10%Stage Ⅳ9%Fujisawa Y. et al., Skin Cancer 2008;195-20440
Treatment algorithm for melanoma:Clinical practice guideline for skin cancer (Japan)ProphylaxisRisk factorScreeningClinical findings/DermoscopyDifficulties inclinical diagnosisBiopsyHistologyDiagnosisNCCNPreoperative testTarget of chemotherapyDistant metastasisNo distant metastasisDTICTis, T1a T1bExcision of primary lesionNo clinical lymphnode metastasisClinical lymph nodemetastasisSurgical excisionof metastaticlesion (smallnumber ofmetastasis )ClinicalstudyRadiationBSCHepatic arteryinjection (livermetastasis only)Excision of primary lesion SLN biopsyNo SLN metastasisExcision of primary lesion radical lymph node dissectionSLN metastasisSLN: Sentinel lymph nodeDTIC: DacarbazineBSC: Best supportive careAdjuvant therapyFollow-upAdapted from ncer/mm/mm.html41
Overall survival rate of melanoma by Stage Melanoma is extremely resistant to chemotherapy. The response rate of DTIC(Dacarbazine), standard treatment for progressive melanoma, is 10-20%. Melanoma is resistant to radiotherapy in general.Overall survival rate(%)100Survival curve by Stage (UICC, 2002) in Japanese melanoma patientsStage I (n 264) 90%80Stage II (n 295) 72%60Stage III (n 155) 54%Stage I40Stage IIStage III20Stage IVStage IV (n 87) 7%0020406080100120p 0.0001p 0.0029p 0.0001(log-rank test)140 (month)TimeIshihara K, et al. Int J Clin Oncol 2008, 13: 33-41Saida T. et al. Issatsu de wakaru hifu gan (Bunkodo) 2011, p234-23742
Histological subtypes of melanoma(Clark’s classification)Nodular melanoma:NMSuperficial spreading melanoma:SSMAcral lentiginous melanoma:ALMLentigo maligna melanoma:LMMAtypical melanocyte (individuality)Alveolar of atypical melanocyteAtarashii hifukagaku version 2 (Nakayama shoten) 2011, p457-458Saida T. et al. Issatsu de wakaru hifu gan (Bunkodo) 2011, p222, 22943
Incidence rate according to types of melanomaNMJapan1) �803.8%100 (%)1.0%14.0%US2)063.0%204012.0% 9.0%6080100 (%)1) Japanese Classification of Skin Cancer version 2 (KANEHARA & Co., LTD) 2010, p178-1792) Fujisawa Y. et al. Nihon Rinsho 2013, 71 (Suppl 4): 7-1244
Oncogenic mutation of melanoma Major signaling pathways in melanoma and oncogenic mutation frequency1)RTKGPCRαγβ30-50% LossPTENGNAQ mutated 50% ofuveal melanomaGrowth FactorsRASCell MembraneCytoplasmNRAS 15% mutatedPI3KRAF30% AmplifiedAkt1MEK1/2IκBmTORGEFTBRAF 50-70% CKLIMKMLCMPK1NFκBTranslationTranscription (CDK4, CCND1, BCL2)Survival, proliferation, metastases, neoangiogenesis1) Bello DM, et al: Cancer Control 20: 261-281, 20132) Ashida A., et al.: J Dermatol Sci. 66 (3): 240-242, 20123) Yamazaki N., et al.: Melanoma Res. 25 (1): 9-14, 201545
Treatment algorithm for melanoma:Clinical practice guideline for skin cancer (Japan)ProphylaxisRisk factorScreeningClinical findings/DermoscopyDifficulties inclinical diagnosisBiopsyHistologyDiagnosisNCCNPreoperative testTarget of chemotherapyDistant metastasisNo distant metastasisNivolumabVemurafenibDTICTis, T1a T1bExcision of primary lesionNo clinical lymphnode metastasisClinical lymph nodemetastasisSurgical excisionof metastaticlesion (smallnumber ofmetastasis )ClinicalstudyRadiationBSCHepatic arteryinjection (livermetastasis only)Excision of primary lesion SLN biopsyNo SLN metastasisSLN metastasisExcision of primary lesion radical lymph node dissectionSLN: Sentinel lymph nodeDTIC: DacarbazineBSC: Best supportive careAdjuvant therapyFollow-upAdapted from ncer/mm/mm.html46
Phase III study (NO25026[BRIM3])Overseas Phase III study (NO25026[BRIM3]) Study designPreviously untreatedpatients with unresectableStage III or Stage IVmelanoma positive forBRAF V600 mutation*1)(n 675)Vemurafenib960mg, b.i.d., p.o.(n 337)RPD1:1Dacarbazine (DTIC)*2)1,000mg/m2, i.v.,3 week cycle(n 338)Stratification factor :Regions, ECOG PS, Metastatic classification, LDHPD*1) Determined by cobas 4800 BRAF V600 Mutation Testapproved as the companion diagnostics.*2) This dosage and administration of DTIC is not approved inJapan. Primary endpoints:PFS, OS Secondary endpoints:Best overall response rate (BORR), Durationof response, Time to response, Safety etc.*Efficacy endpoints by investigator assessmentChugai Internal Document; Chapman PB, et al. N Engl J Med 2011, 364: 2507-251647
Phase III study (NO25026[BRIM3])Patient CharacteristicsDTIC (n 338)Vemurafenib (n 337)181 (54%)200 (59%)52.5 (17-86)56.0 (21-86)Metastatic ClassificationIV:M1aIV:M1bIV:M1cUnresectable StageIIIC40 (12%)65 (19%)220 (65%)13 (4%)34 (10%)62 (18%)221 (66%)20 (6%)Histological SubtypesSSMLMMALMNMOther109 (32%)5 (1%)3 ( 1%)78 (23%)143 (42%)104 (31%)1 ( 1%)1 ( 1%)78 (23%)153 (45%)ECOG PS01230 (68%)108 (32%)229 (68%)108 (32%)Serum LDHNormal rangeElevated196 (58%)142 (42%)195 (58%)142 (42%)MaleMedian age (range)Chugai Internal Document; Chapman PB, et al. N Engl J Med 2011, 364: 2507-2516 48
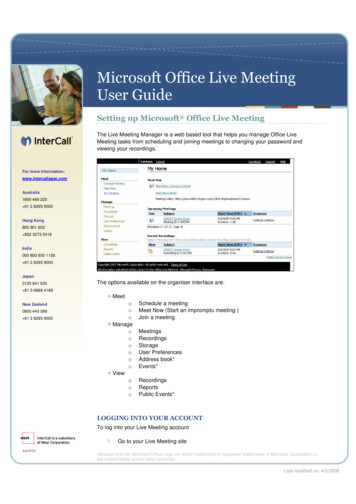
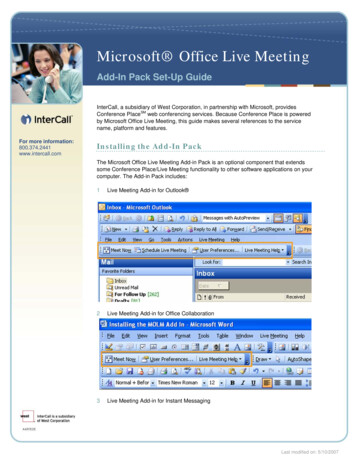
Phase III study (NO25026[BRIM3])PFS (at the time of primary analysis)Progression-free survival1.0Vemurafenib (n 275)DTIC (n 274)0.8HR 0.26 (95%CI 0.20-0.33)p 0.0001, Unstratified log-rank test0.60.40.20n at riskDTICVemurafenibNumber of events104 (37.8%)182 8852114812228105165010353403000061612 (month)00Investigators assessment, RECIST ver. 1.1Data cut-off:2010/12/30Chugai Internal Document; Chapman PB, et al. N Engl J Med 2011, 364: 2507-251649
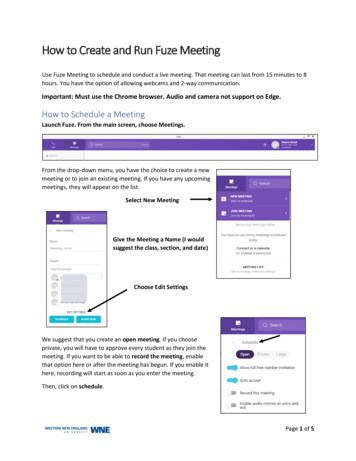
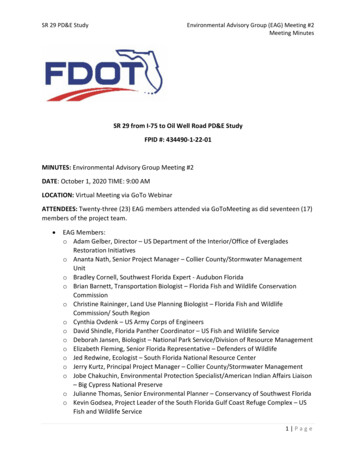
Phase III study (NO25026[BRIM3])OS (at the time of primary analysis)Vemurafenib (n 336)DTIC (n 336)1.0Number of events43 (12.8%)75 (22.3%)HR 0.37 (95%CI 0.26-0.55)p 0.0001, Unstratified log-rank testOverall survival0.80.60.40.20n at 6137210981626411167Time8910113980914161100203512 (month)00Data cut-off:2010/12/30Chugai Internal Document; Chapman PB, et al. N Engl J Med 2011, 364: 2507-2516 50
Phase III study (NO25026[BRIM3])Best overall response rate, Duration of response(at the time of primary analysis)RespondersResponse rate(95%CI)CRPRSDPDMedian Durationof response(95%CI)DTIC(n 220)Vemurafenib(n 219)125.5% (2.8-9.3)10648.4% (41.6-55.2)0 (0.0%)12 (5.5%)53 (24.1%)103 (46.8%)2 (0.9%)104 (47.5%)81 (37.0%)23 (10.5%)NR(4.60-NR)5.49 month(3.98-5.72)p-value(Schouten χ2 test) 0.0001NR:Not reachedData cut-off:2010/12/30Chugai Internal Document; Chapman PB, et al. N Engl J Med 2011, 364: 2507-251651
Phase III study (NO25026[BRIM3])Best tumor response (at the time of primary analysis) Vemurafenib (n 209)Change from Baselinein Diameters of Target Lesions(%)250200150100500-50-100Metastatic ClassificationUnresectable Stage IIICn 219IV:M1aResponders (n)106IV:M1bResponse rate (%)48.4IV:M1cCR (n)PR (n)Median Timeto response(month)21041.45Change from Baselinein Diameters of Target Lesions DTIC (n 158)(%)250200150100500-50-100Metastatic ClassificationUnresectable Stage IIICIV: M1aIV: M1bIV: M1cn 220Responders (n)Response rate (%)CR (n)PR (n)Median Timeto response(month)125.50122.72Data cut-off:2010/12/30Chapman PB, et al. N Engl J Med 2011, 364: 2507-251652
Phase III study (NO25026[BRIM3])Summary of safety (at the time of primary analysis)DTIC(n 282)Vemurafenib(n 336)Any AEsAEs of Grade 3 and aboveAEs of Grade 4AEs of Grade 5Serious AEsAEs that led to discontinuationAEs that led to dose modification/interruptionDeaths*Due to other causes besides disease progression253 (89.7%)86 (30.5%)22 (7.8%)6 (2.1%)45 (16.0%)12 (4.3%)44 (15.6%)16 (5.5%)†1 (0.3%) †326 (97.0%)168 (50.0%)13 (3.9%)6 (1.8%)110 (32.7%)19 (5.7%)129 (38.4%)22 (6.5%)4 (1.2%)Typical AEs associated with vemurafenibCutaneous squamous cell rmal liver function testQT prolongation1 (0.4%)10 (3.5%)10 (3.5%)9 (3.2%)108 (38.3%)13 (4.6%)16 (5.7%)62 (18.5%)202 (60.1%)124 (36.9%)165 (49.1%)138 (41.1%)59 (17.6%)28 (8.3%)* Deaths within 28 days of last dosing† DTIC (n 289)Data cut-off:2010/12/30Chugai Internal Document; Chapman PB, et al. N Engl J Med 2011, 364: 2507-251653
Phase III study (NO25026[BRIM3])Adverse events (incidence: 10%)DTIC (n 282)All Grades Grade 3Total Pts with at Least one ingPhotosensitivity ed appetiteHyperkeratosisEdema peripheralPain in extremitySkin papillomaDry skinDysgeusiaMyalgiaErythemaCutaneous squamous cell carcinomaNeutropeniaMedDRA ver. 13.1, NCI-CTCAE ver. 4.0253 (89.7%)115 (40.8%)87 (30.9%)9 (3.2%)3 (1.1%)6 (2.1%)34 (12.1%)67 (23.8%)10 (3.5%)26 (9.2%)65 (23.0%)25 (8.9%)4 (1.4%)20 (7.1%)-13 (4.6%)17 (6.0%)-3 (1.1%)9 (3.2%)4 (1.4%)4 (1.4%)1 (0.4%)32 (11.3%)Data (1.8%)(0.7%)--1 (0.4%)3 (1.1%)---2 (0.7%)----5 (1.8%)-----1 (0.4%)24 (8.5%)Vemurafenib (n 336)All Grades Grade 3326 (97.0%)101 (30.1%)112 (33.3%)165 (49.1%)121 (36.0%)117 (34.8%)84 (25.0%)50 (14.9%)101 (30.1%)72 (21.4%)32 (9.5%)59 (17.6%)74 (22.0%)53 (15.8%)67 (19.9%)50 (14.9%)45 (13.4%)62 (18.5%)54 (16.1%)44 (13.1%)39 (11.6%)38 (11.3%)40 (11.9%)2 (0.6%)168 (50.0%)4 (1.2%)6 (1.8%)11 (3.3%)28 (8.3%)1 (0.3%)2 (0.6%)4 (1.2%)9 (2.7%)2 (0.6%)-2 (0.6%)5 (1.5%)-4 (1.2%)1 (0.3%)1 (0.3%)1 (0.3%)----38 (11.3%)1 (0.3%)Chugai Internal Document; Chapman PB, et al. N Engl J Med 2011, 364: 2507-251654
Phase III study (NO25026[BRIM3])Conclusions:NO25026[BRIM3] Vemurafenib demonstrated
BRAF mutation should be determined by cobas 4800 BRAF V600 Mutation Test. The cobas 4800 BRAF V600 Mutation Test has been approved as the companion diagnostics in the US (Aug. 2011), and CE-marked in the EU (Aug. 2011). 5 BRAF mutation Source ATP