Transcription
pISSN, eISSN 0125-5614M Dent J 2017; 37 (1) : 103-111Case ReportGuided implant placement and provisional restorationsin the aesthetic zone: a case reportNawakamon Suriyan1, Surakit Visuttiwattanakorn2, Chatchai Kunavisarut3,Natthamet Wongsirichat2123Prachatipat Hospital, PathumthaniDepartment of Oral Maxillofacial Surgery Faculty of Dentistry Mahidol UniversityDepartment of Advanced General DentistryPurpose: The accuracy of implants placed with the aid of a surgical template is limited. The objective of thisstudy was to validate the position between virtually planned implants using a computer and then comparing theclinically placed implants with the computer aided surgical template in the maxilla.Material and Methods: The implants’ positions were calculated and compared between the planned implantsand the implants' clinical position after surgery. The results show the most differences in distance at the levelof the hex, the apex, and the depth. The angular differences were presented in degrees.Results: The greatest errors were found at the vertical depth and showed divergence at the level of the hexand apex of the implants.Conclusion: there were significant differences between the virtually planned implants' position and the finalposition of implants placed clinically. For the treatment planning, placement, and restoration of dental implantsfor a partially edentulous patient it is recommended that clinicians, who are providing dental implant procedures,become knowledgeable in 3D diagnosis and treatment planning concepts and should also be familiar withinteractive treatment planning software applications. Anatomical limitations can make implant locations difficult todetermine. This article describes how to facilitate a computer-guided surgical technique, for a partially edentulouspatient, with a fabricated restoration prior to implant placement in order to create more accuracy.Keyword: Computer guided implant, Computer-aided design, Computer-assisted manufacturing, provisionalrestoration, Computer tomography, Dental implantHow to cite: Suriyan N, Visuttiwattanakorn S, Kunavisarut C, Wongsirichat N. Guided implant placement andprovisional restorations in the aesthetic zone: A case report. M Dent J 2017; 37: 103-111.In dentistry using digital techniques canmaximize the potential of emerging technologies.The third wave is in full swing. Are you on boardyet? The clock is ticking. By 2020, all consumerproducts will be available on demand via 3Dprinting so get connected or be prepared to fail.The 3 dimensional image is the key to achievethe long term success from the point of view ofsatisfaction and biological and aesthetic success[1]. The AAOMR(The American Academy ofOral and Maxillofacial Radiology) recommendsthat cross-sectional imaging be used for theassessment of all dental implant sites and thatCBCT is the imaging method of choice for gainingthis information. The team approach will makean accurate and predictable placement of theimplant, include the temporary abutment andprovisional crown. Advancements in implantdesign, digital dentistry, restorative protocols, andprosthetic materials continue to improve both theefficacy and efficiency of treatment. The ability todigitally plan and visualize implant restorations,prior to surgical intervention, allows the clinicianto evaluate virtually every aspect of a case beforetreatment begins; from extraction, to implantation,to the final prosthetic outcome. This includesintraoral scanning, digital treatment planning,guided surgery, CAD/CAM technology, and theCorresponding author: Nawakamon Suriyan, Prachatipat Hospital, Pathumthani Tel: 66815682588 Email: nawakamons@hotmail.comReceived : 1 December 2016Accepted : 8 March 2017
Nawakamon Suriyan, et alversatility of the provision [2]. Many systematicreviews support immediate provisionalization orrestoration to provide benefits to the patient in termof appearance, satisfaction scores and overalllength of treatment. Patient satisfaction is anotherimportant factor in predicting the success ofimplant therapy in the anterior maxilla. This articlepresents a comprehensive approach to optimizefunctional and aesthetic results by blendingsurgical, technical, and restorative steps into onesuccessful protocol. The drill guide design is usedto provide exact implant placement, virtual crownsand to get all of the restorative components.The techniques provide 3D digital informationusing computed tomography (cone beam-CT/CBCT and 3D implant planning software withthe advances in CAD/CAM (Computer-AidedDesign/Computer-Assisted Manufacturing) [3].Comprehensive treatment planning is essentialfor long term success. The treatment plan willstart from scanning, designing, and milling.Immediate restoration and loading can be used ineach case to fulfil all the inclusion criteria and toensure the implant achieves good primary stabilityat an adequate length ( 8 mm) and diameter( 4 mm). The restoration should not be removedduring the healing period of approximately 6weeks. The patient should be educated in how tofunction during the healing period and to practiceadequate oral hygiene. Screw-retained provisionalrestorations are also recommended. This studyaims to evaluate guided implant placement withan immediate provisional crown or bridge with aconventional implant placement in the aestheticzone [4].The digital process chain work, from an Intraoral structure of each patient, was scanned using anintra-oral scanner (Trios 3Shape, USA) and mergedwith the CBCT (GiANO, Newtom, Italy) images.Implant placements (CAMLOG, Germany) wereplanned, regarding the direction and position, usingsoftware (Implant Studio , Denmark) and placedusing the CAD/CAM guide surgical template. This104 M Dent J 2017 April; 37 (1): 105-113software uses a prosthodontics driven conceptby initially placing virtual crowns according tothe setting. Proper depths and angulations canbe determined, ensuring that the implants arepositioned to accommodate the maximum amountof bone, while establishing optimal support andthe platform needed to achieve an aestheticoutcome for the proposed restoration. Then, thefabrication of anatomically accurate abutments ofthe restoration was done using CAD/CAM zirconia.The CBCT was performed before and after implantplacement. During surgery, the drilled templatewas used as a drill guide. Then crop the CBCT in3 dimensions and then superimpose the imageslater in a software defined panoramic curve.The software starts by placing virtual crownsaccording to the prosthodontic setting. Properdepth and angulation are determined, ensuringthat the implants are positioned to accommodatea maximum amount of bone while establishingoptimal support and the platform needed toachieve an aesthetic outcome for the proposedrestoration. We designed the implant supportedbridge 13 to 11 and the 21 implant supportedcrown using the 3Shape software. The plan wasto fabricate an anatomically accurate abutmentcrown and bridge by using CAD/CAM zirconia.The virtual planning can be undertaken in thesoftware by the prosthodontics and professionalsurgery. From the CBCT we measured the housefield unit at the osteotomies’ site to confirm thebone quality. The CBCT images in this studydemonstrated a mean thickness of the facialbone wall as being between 1-2 mm at variouslevels. After the implant placement, a digitalimpression with a scan body were recorded andcompared with the preoperative using McNemar’stest. One hour before surgery the patient willget 2 g of Amoxillin (400 mg) or Ibuprofen (1g) or paracetamol then the mucoperiosteal flapfrom tooth 14 to 22 is started. Preparation of theimplant bed starts with a bone drill sequence. Itwas planned to connect a definitive prefabricated
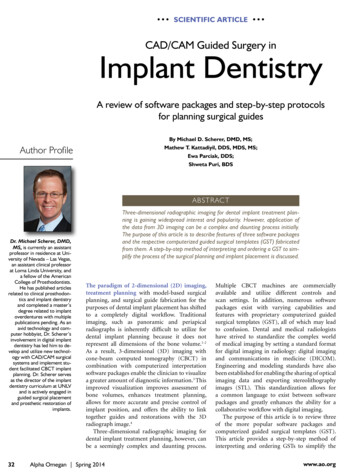
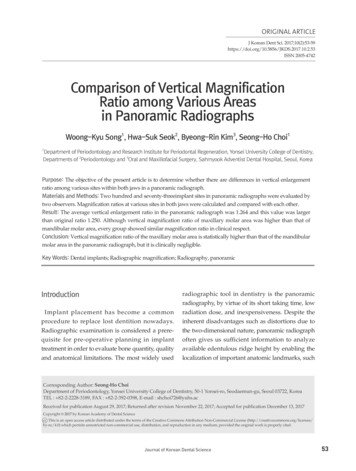
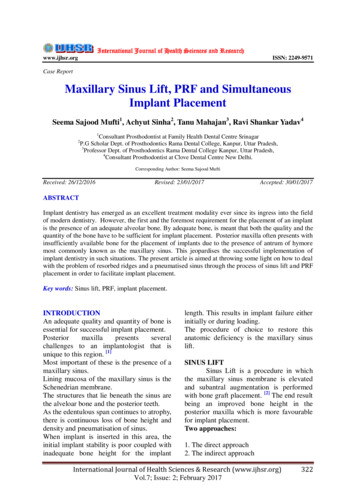
Guided implant placement and provisional restorations in the aesthetic zone: a case reportabutment and provisional restoration to the implantimmediately after surgery. The restoration shouldbe taken out of any functional occlusal contactsboth in the centric occlusion and during excursivemandibular movements.Case Report1. Patient HistoryA male patient 72 years of age reported witha history of an extract 3 months earlier from failedroot canal treatment on supported bridge 13-22.He would like to get fix prosthodontics for hismissing teeth. The patient’s general periodontalcondition was fair. The medical history to ruleout systemic contraindications was assumed, Hehad cardiovascular disease and was on Warfarinat 50 mg per day. The clinical and radiographicevaluation was performed on the initial visit. Hewas informed of all the viable options to replace hismissing left molar. A detailed written description ofthe risks and benefits of the proposed treatmentwas given, followed by a written consent formbeing signed.I (Figure 3). The left side showed an unclassifiedmolar relationship due to the missing tooth (Figure4). The SAC classification for implant dentistry wasused. An implant site–specific evaluation was thencarried out, including an evaluation of the innerocclusal space, in addition to both a hard- anda soft-tissue assessment, showing good ridgedimensions and keratinized tissue volume. Thekeratinized tissue width was 8 mm. The CT scanrevealed the bucco-lingual cortical width was 7mm. The mesio-distal width was 32 mm. The CTscan revealed the bucco-lingual cortical widthwas 7 mm. From the Orthopantomograph, thecrest to floor of nose was 16mm. (Figure 3). Anintraoral periapical radiograph was also taken.(Figure 4-6).2. Treatment OptionsThe patient was presented with the followingtreatment options for the replacement of the Figure 1 Pre-operation, There are available bone at theimplant siteanterior maxilla. The first option was a 3-unitfixed prosthodontic using teeth 14, 22 and 23as abutments. Second, an implant restoration forthe replacement of the edentulous space at teethnumbers 13, 11, 21 and 22 was determined to bethe more conservative option. Third an implantrestoration for the replacement of the edentulousspace at teeth numbers 13, 11, 21 or 22 wasdetermined.3. Clinical assessmentAn inclusive extraoral examination, followedby intraoral examination were performed (Figure 1, Figure 2 Pre-operation, There are crossectional showbone available at the implant site2). The occlusion on the right side show molar Clhttp://www.dt.mahidol.ac.th/division/th Academic Journal Unit105
Nawakamon Suriyan, et al4. Surgical technique and outcomeA surgical guide was used to ensure aprosthodontically favourable placement of theimplant in 3 dimensions. On the day of the surgery,the patient rinsed with 10 ml of 0.2% Chlorhexidinegluconate solution followed by an extraoral scrubwith 5% povidine iodine. The surgical procedureswere all carried out under local anaesthesia insterile surgical conditions. Conventional flapFigure 3 The Ortho-panoramic image shows the bone procedures were used and the osteotomy sitesin the edentulous area and no bonewere directly cooled with irrigation by removingpathologythe drills in sequence. Before implant insertion,a periodontal probe was used to check for anybony fenestrations of the osteotomy. The guidedimplants were inserted first with a hand pieceat the recommended torque, and then the finalseating was done manually with a wrench until theprimary stability was good. The 3.8 -mm-diameter 3implants were then placed and a healing abutmentFigure 4 The other Teeth showa a normal periodontal of 3 mm in height was used to cover the fixture forthe two-stage implant-procedure. An immediatewith no pathology in the apical areapostoperative radiograph was done to confirm thecomplete seating of the cover screw.5. Loading Protocols in Implant Dentistry PartiallyDentate PatientsA conventional loading of an implant, after ahealing period of 3 to 6 months, was used.Figure 5 Bone at the edentulous areaFigure 6 The neighbouring teeth no bone pathology106 M Dent J 2017 April; 37 (1): 105-1136. Prosthodontics technique and outcomeDuring the restorative phase, an impressionwas taken at implant level, according to theprotocol. This set assists in determining thedimensions for assuming the axial alignment andgingival height. The appropriate space obtainedand good emergence profile of the cementretained restoration was selected for this particularcase. All the information gathered before theactual surgery, together with the guided surgicaltemplate, would definitely facilitate the proceduresto ensure an accurate, functional and aestheticfinal restoration.
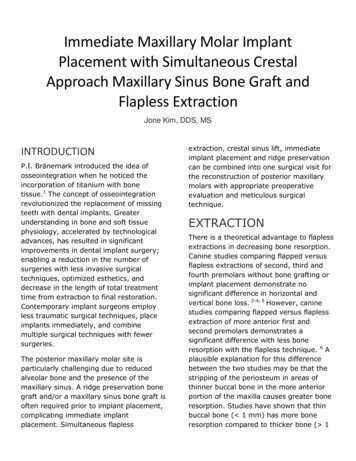
Guided implant placement and provisional restorations in the aesthetic zone: a case reportFigure 7 Virtual crown (3Shape Implant Studio , USA)for prosthetic driven implant planning andsurgical guide design.Figure 9 Design and manufacturing abutmentincluding the provisional bridge providedbefore surgery (#13,#11,#21)Figure 11 A guided template was stably placed beforethe start of the operationFigure 8 Cone beam (CBCT) merges with intraoral 3Ddigital impression files and created approvedimplant positions with a click.Figure 10 The tooth-supported surgical guide(SurgiGuided,3Shape ImplantStudio ,USA)design on the stereolithography modelFigure 12 Implant placementhttp://www.dt.mahidol.ac.th/division/th Academic Journal Unit107
Nawakamon Suriyan, et alFigure 13 Final abutment design by the 3shape DentalSystem , USAFigure 14 Fix titanium base and customized CAD /CAMabutment with the resin cementFigure 15 The emergence profile of the zirconiaabutment on Ti-base was sandblast and fixusing resin cement (Multilink Automix, IvoclarVivadent)Figure 17 Adjustments should be reglazed and thenpolished thoroughly with appropriate rotaryinstrumentation. .108 M Dent J 2017 April; 37 (1): 105-113Figure 16 Final monolithic zirconia crowns fabricatedby computer-aided design and computeraided manufacture was cemented.Figure 18 Zirconia abutment position and preparationof teeth before inserting the crown
Guided implant placement and provisional restorations in the aesthetic zone: a case reportimplant placement. Titanium-base abutments withcustomizing abutments manufactured via CAD/CAM be made of zirconium dioxide for bone levelimplant were used with cement-retain crowns.They are two pieces abutments with titanium basesometimes concerned about bonding betweentwo pieces abutment and complication regardingof shipping ceramic. The main advantage of thisabutment type is there is no ceramic materialFigure 19 Cross-sectional positioninside the titanium implant connection. However,to date the disadvantage lies in the lack ofevidence in published. The definitive prosthesisdesign with posterior manufacture, based on thethree-dimensional imaging data, will facilitate thepreparation of a guide for the surgical intervention[7]. This technique results in less postoperativemorbidity, since surgery is minimally invasive, andincreased patient satisfaction is ensured, giventhe appreciation of the immediate restorationFigure 20 Final restoration was done by Monolitic of aesthetics and function [8]. This is probablythe reason that it brings individual, tailoredzirconia crowns and bridge on implantmade solutions to our job. However, appropriatepatient selection and an understanding of newlydeveloped techniques and limitations are neededto ensure a high success rate in the aesthetic zone[2].Figure 21 Final restorationImplant restoration, using the guidedsurgery technique and immediate functionalloading, is therefore a predictable procedure,providing that both the patient selection and theemployed surgical techniques are adequate[5,6]. A comprehensive preoperative workup isessential for planning the number and type ofimplants, in addition to the optimum location of theTable 1 The difference between virtual plan andplacementTooth 0.630.37Corono-apical1.221.461.38Divergence degree12.328.4610.14DiscussionThe accuracy of guided surgery have beenanalysed [9]. The accuracy depend on manyfactors such as the quality of the computertomography, the quality of surface scan evenintraoral scan or cast scan, the plane of panoramic,http://www.dt.mahidol.ac.th/division/th Academic Journal Unit109
Nawakamon Suriyan, et althe quality of merging, the undercut of dental arch,the number of implant, the design of the surgicaltemplate even bone support or tooth support, theseat of the surgical template, The implant system,the deviation of the axis of the drill or implant [5].The digital data shows all information regardingthe available possibilities from conception anddesign through to fabrication. These are alladvantages in order to communicate correctly andeffectively between the dentist, the dentaltechnician and the patient [8]. Diagnostic andrestorative tools allow for the precise, predictableplacement of dental implants, providing patientswith improved function, comfort and aesthetics.The implementation of intraoral scanning, digitaltreatment planning, guided surgery, and CAD/CAM software enables detailed visualization of theprosthetic outcome prior to the actual treatment[6,10]. These technologies help to improvetreatment outcomes, offering the benefits ofprovisionalization to a growing number of patientswhile helping to ensure an accurate, functionaland aesthetic final restoration. It is the best processchain, together with CAD/CAM and the digitalproduction method, to achieve professional results[5,11,12]. The systematic review of soft tissuealteration following immediate implant placementand restoration show the adequate of soft tissue inboth height and embrasure fill affects the estheticoutcome [13].Digital transformation is more than a“phenomenon” and certainly more than atechnological one; as it states that its technologicalpillars such as mobile services, cloud services,big data including analytics and social networkingor system engagement will be driving the futuregrowth and innovation in the industry.AcknowledgementDepartment of Oral & Maxillofacial Surgery,Faculty of Dentistry, Mahidol University110 M Dent J 2017 April; 37 (1): 105-113Funding: NoneCompeting interests: NoneEthical approval: None (Case Report)References1. Ramasamy M, Giri, Raja R, Subramonian, Karthik,Narendrakumar R. Implant surgical guides: From thepast to the present. Journal of pharmacy & bioalliedsciences 2013; 5: S98-S102.2. Abad-Gallegos M, Gomez-Santos L, SanchezGarces MA, et al. Complications of guided surgeryand immediate loading in oral implantology: a reportof 12 cases. Medicina oral, patologia oral y cirugiabucal. 2011 ;16: 220-224.3. Widmann G, Stoffner R, Schullian P, et al.Comparison of the accuracy of invasive andnoninvasive registration methods for image-guidedoral implant surgery. The International journal of oral& maxillofacial implants 2010; 25: 491-498.4. Pettersson A, Kero T, Soderberg R, Nasstrom K.Accuracy of virtually planned and CAD/CAM-guidedimplant surgery on plastic models. The Journal ofprosthetic dentistry. 2014; 112: 1472-1478.5. Schneider D, Marquardt P, Zwahlen M, Jung RE. Asystematic review on the accuracy and the clinicaloutcome of computer-guided template-based implantdentistry. Clinical oral implants research. 2009; 20:73-86.6. Tahmaseb A, De Clerck R, Wismeijer D. Computerguided implant placement: 3D planning software,fixed intraoral reference points, and CAD/CAMtechnology. A case report. The International journalof oral & maxillofacial implants. 2009; 24: 541-546.7. Valente F, Schiroli G, Sbrenna A. Accuracy ofcomputer-aided oral implant surgery: a clinical andradiographic study. The International journal of oral &maxillofacial implants. 2009; 24: 234-242.8. Pettersson A, Komiyama A, Hultin M, Nasstrom K,Klinge B. Accuracy of virtually planned and templateguided implant surgery on edentate patients. Clinicalimplant dentistry and related research. 2012; 14: 527537.9. Jung RE, Schneider D, Ganeles J, et al. Computertechnology applications in surgical implant dentistry:a systematic review. The International journal of oral& maxillofacial implants. 2009; 24: 92-109.
Guided implant placement and provisional restorations in the aesthetic zone: a case report10. Van Assche N, Vercruyssen M, Coucke W, TeughelsW, Jacobs R, Quirynen M. Accuracy of computeraided implant placement. Clinical oral implantsresearch. 2012; 23:112-123.11. Zhao XZ, Xu WH, Tang ZH, Wu MJ, Zhu J, ChenS. Accuracy of computer-guided implant surgeryby a CAD/CAM and laser scanning technique. TheChinese journal of dental research. 2014; 17: 31-36.12. Vasak C, Strbac GD, Huber CD, Lettner S, GahleitnerA, Zechner W. Evaluation of three different validationprocedures regarding the accuracy of templateguided implant placement: an in vitro study. Clinicalimplant dentistry and related research. 2015; 17: 142149.13. Khzam N, Arora H, Kim P, Fisher A, Mattheos N,Ivanovski S. Systematic Review of Soft TissueAlterations and Esthetic Outcomes FollowingImmediate Implant Placement and Restoration ofSingle Implants in the Anterior Maxilla. Journal ofperiodontology. 2015; 86: 1321-1330.http://www.dt.mahidol.ac.th/division/th Academic Journal Unit111
assessment of all dental implant sites and that CBCT is the imaging method of choice for gaining this information. The team approach will make an accurate and predictable placement of the implant, include the temporary abutment and provisional crown. Advancements in implant design, digital dentistry, restorative protocols, and prosthetic materials continue to improve both the efficacy and .