Transcription
Peri-Implant Therapy for the Dental Hygienist
Peri-Implant Therapy for the Dental HygienistClinical Guide to Maintenance and Disease ComplicationsSusan S. Wingrove, RDHWriter, Trainer, Clinical AdvisorWingrove DynamicsMissoula, MT
This edition first published 2013 2013 by John Wiley & Sons, Inc.Wiley-Blackwell is an imprint of John Wiley & Sons, formed by the merger of Wiley’s global Scientific, Technical andMedical business with Blackwell Publishing.Editorial offices:2121 State Avenue, Ames, Iowa 50014-8300, USAThe Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK9600 Garsington Road, Oxford, OX4 2DQ, UKFor details of our global editorial offices, for customer services and for information about how to apply for permissionto reuse the copyright material in this book please see our website at www.wiley.com/wiley-blackwell.Authorization to photocopy items for internal or personal use, or the internal or personal use of specific clients, isgranted by Blackwell Publishing, provided that the base fee is paid directly to the Copyright Clearance Center, 222Rosewood Drive, Danvers, MA 01923. For those organizations that have been granted a photocopy license by CCC, aseparate system of payments has been arranged. The fee codes for users of the Transactional Reporting Service areISBN-13: 978-0-4709-6285-5/2013.Designations used by companies to distinguish their products are often claimed as trademarks. All brand names andproduct names used in this book are trade names, service marks, trademarks or registered trademarks of theirrespective owners. The publisher is not associated with any product or vendor mentioned in this book.The contents of this work are intended to further general scientific research, understanding, and discussion only andare not intended and should not be relied upon as recommending or promoting a specific method, diagnosis, ortreatment by health science practitioners for any particular patient. The publisher and the author make norepresentations or warranties with respect to the accuracy or completeness of the contents of this work and specificallydisclaim all warranties, including without limitation any implied warranties of fitness for a particular purpose. Inview of ongoing research, equipment modifications, changes in governmental regulations, and the constant flow ofinformation relating to the use of medicines, equipment, and devices, the reader is urged to review and evaluate theinformation provided in the package insert or instructions for each medicine, equipment, or device for, among otherthings, any changes in the instructions or indication of usage and for added warnings and precautions. Readersshould consult with a specialist where appropriate. The fact that an organization or Website is referred to in this workas a citation and/or a potential source of further information does not mean that the author or the publisher endorsesthe information the organization or Website may provide or recommendations it may make. Further, readers should beaware that Internet Websites listed in this work may have changed or disappeared between when this work waswritten and when it is read. No warranty may be created or extended by any promotional statements for this work.Neither the publisher nor the author shall be liable for any damages arising herefrom.Library of Congress Cataloging-in-Publication DataWingrove, Susan S.Peri-implant therapy for the dental hygienist : clinical guide to maintenance and disease complications /Susan S. Wingrove.p. ; cm.Includes bibliographical references and index.ISBN 978-0-470-96285-5 (softback : pbk. : alk. paper) – ISBN 978-1-118-64686-1 (pdf) – ISBN 978-1-118-64690-8 (pub)– ISBN 978-1-118-64691-5 (mobi)I. Title. [DNLM: 1. Dental Implants. 2. Dental Hygienists. 3. Dental Implants–adverse effects. WU 640]RK667.I45617.6'93–dc232013007107A catalogue record for this book is available from the British Library.Wiley also publishes its books in a variety of electronic formats. Some content that appears in print may not beavailable in electronic books.Cover image: bottom left image Susan S. WingroveCover design by Matt KuhnsSet in 10/12.5 pt Palatino by Toppan Best-set Premedia Limited12013
To my late husband Dr. Frank Wingrove, who opened my mind and my passionfor implant and regeneration dentistry.To my late father Dr. Richard Strand, who passed along the importance ofbuilding relationships with your patients.They both taught me lessons to last a lifetime.Life is a journeyThat continues around every corner.Embrace it, treasure it, and live it to the fullest!Go, see, do
ContentsContributor List . . . . . . . . . . . . . . . . . . . . . . . . . ix5Foreword . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xiiiRobert Schneider, DDS, MSHow to Talk to Patients about ImplantDentistry: Risks, Benefits, andAlternatives . . . . . . . . . . . . . . . . . . . . . . . . . 776AIM for Implant Success: Assess, Identify,and Monitor . . . . . . . . . . . . . . . . . . . . . . . . 931Implants 101: History, ImplantDesign, Parts, and Pieces . . . . . . . . . . . . . . 172Patient Selection for Implant Therapy:Oral Systemic Health, MedicalHistory, and Risk Assessment . . . . . . . . . 15Implant Complications: Peri-ImplantDisease and Cement ResidueProtocol . . . . . . . . . . . . . . . . . . . . . . . . . . . 107With contribution by Alfonso Piñeyro,DDS3What Lies Beneath the Surface?Natural Teeth, Bone, and ImplantPlacement . . . . . . . . . . . . . . . . . . . . . . . . . . 298Implant Home Care Is Key! . . . . . . . . . . 1279Safe, Effective, In-Office ImplantMaintenance . . . . . . . . . . . . . . . . . . . . . . . 1454Setting the Stage: Adjunctive SurgicalProcedures, Restorative Options,and Treatment Planning . . . . . . . . . . . . . . 51With contributions by Robert Horowitz,DDS, and Robert Schneider, DDS, MSAcknowledgments . . . . . . . . . . . . . . . . . . . . . . . . xiAppendix: Terminology andResources . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 175Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 181vii
Contributor ListRobert Horowitz, DDSClinical Assistant ProfessorDepartments of Periodontics and ImplantDentistry, Oral SurgeryNew York University College of DentistryNew York, New YorkAlfonso Piñeyro, DDSClinical Affiliate InstructorUniversity of WashingtonDepartments of Restorative DentistrySeattle, WashingtonRobert Schneider, DDS, MSProfessorUniversity of Iowa Hospitals and ClinicsHospital Dentistry InstituteDivision DirectorMaxillofacial ProsthodonticsIowa City, IowaSusan S. Wingrove, RDHWriter, Trainer, Clinical AdvisorWingrove DynamicsMissoula, Montanaix
AcknowledgmentsOver this past year, many friends, colleagues,and companies have contributed to the successof Peri-Implant Therapy for the Dental Hygienist.It has been another journey for me that I knowwill continue to lead me into more learningopportunities in the future.A very heartfelt thank you goes to thefollowing:To my contributors, Dr. Robert Horowitz,Dr. Alfonso Piñeyro, and Dr. Robert Schneider,who have supported not only me by writ ing sections to be included in the book, butalso hygienists in their role as first respond ers in this important challenge of implantdentistry.To my fellow dental colleagues and friendswho have supported me, critiqued chapters,and encouraged me on this year-long journey:Nancy Adair, Wendy Birtles, Jennifer Butler,Jeff and Kathi Carlson, John DeAngelo, Cath erine Fairfield, Carla Frey, Edie Gibson-Shu man, Debbie and Paul Harrison, Tracy Hull,Carol Jahn, Shelby Kahl, Deborah Lyle, PegMarcy, Linda Meeuwenberg, Linda Miller,Carie Miskell, Erin Murphy, Judy O’Brien,Heather Rogers, Wanda Smith-Beller, JeanneStrand-Anderson, Lynette Thompson, TimTorbenson, Linda Turner, and Leslie Winston.To Dr. Kevin Frawley, Dr. Peter Fritz, Dr.Paul Ouellette, Dr. Marco Padilla, Dr. JohnRemien, and Steve White, for their outstand ing photographs.To the companies that have generously pro vided photos, illustrations, and information:BioHorizons, Colgate, Dentsply, EMS, Glide well Dental, Ivoclar Vivadent, Keystone Dental,Nobel Biocare, Parkell, Paradise Dental Tech nologies (PDT), Preventech, Proctor & Gamble,Rowpar, Salvin Dental, Straumann, Sunstar,Surgical Esthetics, Tepe, and Waterpik.To Rick Blanchette and Melissa Wahl atWiley Blackwell, for their expertise andencouragement.And a special thank you goes to all my“PDT family” nationally and internationallyfor their belief in innovation and their supportfor me and our dental profession.Go, see, do!S.S.W.xi
ForewordOsseointegration and implant dentistry useand research are at a previously unthought-ofpinnacle. Dental implants are no longer “exper imental” but are mainstream dentistry. Theplacement of dental implants is not limited tosurgical specialists such as periodontists andoral and maxillofacial surgeons, many generaldentists are also placing dental implants. Dentalhygienists will see many more patients whohave been restored with implants as their useincreases even further. More than one milliondentists worldwide are eager to learn aboutimplants and offer implants treatment to theirpatients. Many types of dental implants are inuse, and many more are in development.Success for dental implants is based onmany factors from the basic diagnostic proce dures, proper planning, surgical technique,restorative techniques, dental technology, andmaterials knowledge, and, of course, peri odontal maintenance, perhaps the most impor tant in maintaining long-term osseointegrationof the root form implants. Continued observa tion and maintenance of the implant-retainedand -supported prostheses is critical, espe cially with the plethora of prosthesis designsbeing utilized today from conventional crownand bridge, removable prostheses, and hybriddesigns that are very difficult for the patientto clean and maintain.Dental implants are utilized for everythingfrom single-tooth replacement to full archtooth replacement, and each restorationcomes with unique challenges for appropriatehygiene access and maintenance. For singleteeth, proper emergence profile and propercement margin placement is critical in themaintenance of a healthy periodontium. Withfull arch fixed restorations, access to the abut ments and the pontic/gingival areas, whichshould follow a convex contour as desired inroutine pontic design, are very important forpatient access and proper oral hygiene tech nique and procedures.In addition to basic prosthesis design foroptimal hygiene access, the hygienist will alsosee biomechanical issues leading to gingival/alveolar challenges such as fractured or looseprosthetic- and abutment-retaining screws,which can manifest as a loose prosthesis, gin gival hypertrophy, peri-impalantitis, alveolarbone loss, and so on. Cement-retained implantrestorations have become very prevalent. Asignificant periodontal concern is inadequateremoval of the residual cement in the subgin gival areas. Incomplete cement removal canresult in serious peri-implantitis and alveolarbone loss. These issues need to be identifiedby the hygienist and an appropriate treatmentrendered to help ensure the longevity of theimplant and prosthesis along with continuedgingival health.Ailing or failing dental implants, due topoor oral hygiene or lack of appropriate fol low-up, may lead to possible health issues dueto the unaddressed peri-implantitis. Infectionand/or alveolar bone loss can be an issuein many patients, especially with the agingxiii
xiv Forewordpopulation and the “graying” of the babyboomers. Quality oral health care may be achallenge for many of our patients as theytransition into assisted living or supervisedcare facilities for the aged. Dental hygienistswill play a critical role in maintaining thegeneral dental and medical health of thesepatients and the role will expand even more asan increased number of dental implants areplaced and restored and the population ages.This excellent text will provide muchneeded information for the dental hygienistand therapist to facilitate monitoring andmaintaining dental implant patients in anoptimal state of dental health and generalwell-being.Robert Schneider, DDS, MSProfessorUniversity of Iowa Hospitals and ClinicsHospital Dentistry InstituteDivision DirectorMaxillofacial ProsthodonticsIowa City, Iowa
1 Implants 101: History, Implant Design,Parts, and PiecesHistory, 1Dental implant history timeline, 4Implants, 6Implant design, 7Parts and pieces for implants, 10Implant dentistry terminology, 12Summary, 12References, 12Understand as hygienists a tidal wave of ailing or failingimplants may be imminent. It is imperative that hygienists are trained in identifying and treating peri-implantmucosal inflammation that could affect overall bodyhealth. (1)—G. Nogueira-Filho, DDS, MDent, PhDDental hygienists must be ready and be prepared to take on this next, very importantchallenge in our profession! The 21st centuryis an important and critical time to be a hygienist. During this exciting time in dentistry,we as hygienists have a critical role in implanttherapy. As a hygienist, your role will be toaccess patients for healthy periodontium priorto placement of implants, to monitor the tissuesurrounding the implants, and to maintain theimplants through safe, effective implant maintenance. Current studies reveal that infectionsin the periodontium occur in more than 50%of implants placed (2). Therefore we as dentalprofessionals will be faced with differentdynamics, challenges, and complications.As a hygienist the history of implant dentistry makes you aware that implants are notnew, but have been evolving for decades.Patients may have concerns that implants areso new that not enough research or development has been done for them to feel comfortable with the procedure. With your knowledgeof the history, design, and research done onimplants you will be better able to talk withyour patients and answer these concerns. Afundamental understanding of key terms andstatistics associated with implant dentistrywill also be a valuable tool to add to yourverbal skills when talking with patients abouttooth replacement.HistoryBelieve it or not, the history of dental implantsdates back to 600 AD with the ancient Mayans.Dr. and Mrs. Wilson Popenoe found the lowermandible of a young Mayan woman in Honduras in 1931 (Figure 1.1). She was missingsome of her lower teeth and they had beenreplaced with the earliest example of the firstdental implants, made from pieces of shellshaped to resemble teeth. Scientists believePeri-Implant Therapy for the Dental Hygienist: Clinical Guide to Maintenance and Disease Complications,First Edition. Susan S. Wingrove. 2013 John Wiley & Sons, Inc. Published 2013 by John Wiley & Sons, Inc.1
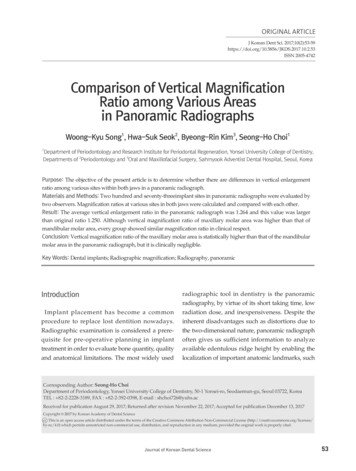
2 Peri-Implant Therapy for the Dental HygienistFigure 1.1 Discovery by Dr. and Mrs. Wilson Popenoe,Honduras, 1931. Reprinted with permission from MalvinE. Ring, Dentistry: An Illustrated History, 1st ed., Mosby.that these shells may have actually worked.Slots were made into the bone and the shellswere pounded in like little wedges, withoutanesthesia!Similar discoveries were made in Egypt,artifacts that date back to the 1700s. Ivory andthe bones of animals were also sometimesused to replace missing teeth. It would bedecades after these archaeological discoveriesbefore the modern world caught up with theMayans’ and Egyptians’ dental technology.In the late 18th and 19th centuries, the levelof dental care went through many changes.Through the letters, journals, and accounts leftby our first president, George Washington, wehave a well-documented case history of hislifelong dental problems and the level ofdental care available at that time. GeorgeWashington started losing his teeth at age 24and by 1789, the year that Washington took hisoath of office, he had only one of his originalteeth left (Figure 1.2).Dr. John Greenwood made a set of denturesfor Washington made of hippopotamus ivoryand eight real human teeth attached by brassscrews. The denture, which was anchored onthe one remaining tooth in Washington’smouth, has a hole that fit snugly around theone tooth. Dr. Greenwood was noted to bequite ahead of his time in his dental practice,Figure 1.2 George Washington’s lower denture. Courtesy of Rick Blanchette.extracting teeth and utilizing them in the manufacture of dentures, but he also experimentedwith implantation.Unfortunately for Dr. Greenwood, the 18thcentury’s lack of antibiotics and any understanding of germ theory or antisepsis doomedany such experiments to failure. He did makePresident George Washington several sets ofdentures, none made out of wood as oftenreferred to. They were made from gold, ivory,lead, and human and animal teeth (horseand donkey teeth were common components),with springs to help them open and bolts tohold them together.In the 18th century, researchers experimented with gold and other metal alloysincluding lead as implants. Dr. Maggiolo fabricated gold implants that were placed in sock ets where teeth had recently been extractedand after a healing period attached a “donor”tooth. Dr. Harris, a physician, attempted thesame procedure with a platinum post, bothhad poor results.Dr. Edmunds in 1886 was the first in theUnited States to implant a porcelain crownmounted on a platinum disc and presented atthe First District Dental Society of New York.Other metal alloys with porcelain crowns wereexperimented with, but these implants did nothave a long-term success rate.
Implants 101: History, Implant Design, Parts, and Pieces 3Dr. E.J. Greenfield, pioneer of the endosseous implant, provided many of basic conceptsof nascent field of implantology. He wasknown for his patented hollow-cylinderimplants made of wire soldered with 24 karatgold. This hollow-basket design was a similardesign that Straumann Implant Companyfrom Switzerland adopted many years later.He presented his research and surgical technique in 1913, and although histological proofof bone-to-implant contact was not availableat that time, he understood the clinical importance to what he called “primary stability”or osseointegration. His surgical techniques,stepwise use of drill diameters starting withround bur, were presented in 1913 and are stillpracticed today (3).It wasn’t until 1937 before the first relativelylong-term implant success was noted. Dr. A.E.Strock used the metal alloy Vitallium , placinga series of implants at Harvard University inanimals and humans. He published a paper onthe physiological effects of Vitallium in bone,with no post-operative complications or reactions noted, total toleration. These were thefirst relatively successful dental implants andcertain types of implants are still cast in Vitallium today.The turning point of implant dental his tory happened in the 1950s, when ProfessorPer-Ingvar Brånemark, an orthopedic sur geon, discovered that titanium componentscan bond irreversibly with living bone tissue.His team designed many studies on thehealing effects of bone with one specificstudy on rabbits in which a titanium metalcylinder was screwed in a rabbit’s thigh bone. A several-month healing period andother experiments of the blood circulation inanimals using a hollow titanium cylinderdemonstrated that the titanium cylinder fusedto the bone. Brånemark named this discoveryosseointegration (the firm, direct, and lastingbiological attachment of a metallic implantto vital bone with no intervening connectivetissue) (Figure 1.3).Figure 1.3 Professor Per-Ingvar Brånemark, an orthopedic surgeon. Courtesy of Nobel Biocare.Brånemark’s research and other colleaguesfrom other disciplines evolved this theory ofosseointegration along with the design ofthe “Brånemark titanium screw” device witha number of specific surface treatments toenhance bioacceptance with bone. One of thekey reasons that titanium was chosen byBrånemark is his relationship to Hans Emneus,an orthopedic surgeon, who studied differentmetals used for hip joint prostheses. Hisresearch indicated that a new metal, titanium,from Russia and used in nuclear industry,might be optimal. Brånemark used a samplefrom Russia and from there on the best metalfor implants has been pure titanium.In 1964, commercial-grade pure titaniumwas accepted as the material of choice fordental implants. Other bodies of medicine(e.g., joint replacements) had recognized thefact that the body does not recognize titaniumas a foreign material, which results in highersuccess rate and fewer rejections. Eventuallythe use of commercial pure titanium evolvedinto the use of titanium alloys (TiAl6V4 being
4 Peri-Implant Therapy for the Dental Hygienistthe most commonly used) due to experimentation and improved durability.In 1981, Dr. Per-Ingvar Brånemark published his findings covering all the data on theanimal and human clinical trials: success rate,concept, and the design of endosteal root-formtitanium implants most commonly placedtoday. In an effort to gain international supportand collaboration, based on patient care withsound biological and clinical principles Brånemark founded the Association of BrånemarkOsseointegration Centers (ABOC).Brånemark identified the edentulous patientas an amputee, an oral invalid, to whom weshould pay total respect and rehabilitationambitions. He was also instrumental in identifying the mouth as a much more importantpart of the human body than medicine andcontrolling agencies had previously recognized. He coined the term osseoperception, “thedentate mouth communicates with the brain,possibly improving not only daily function,but also being an important factor in restitution after intra-cranial vascular events” (P-IBrånemark, September 2005).In the 21st century, technology and clinicalawareness will take on more importance. Thescience and clinical advancements have madeit possible for oral and maxillofacial surgeons,periodontists, and general dentists in theUnited States to double the number of implantsperformed per dentist between 1995 and 2002.Dental implant history timelineAncient history: Mayans back in AD 600 haddental implants made from pieces of shell andancient Egyptians used shells and ivory.1700s: Lost teeth were often replaced withteeth from human donors. The process wasmostly unsuccessful due to immune systemreactions to the foreign material.1800s: Researchers fabricated gold, platinum, and other metal alloys, including lead,into posts that were placed into the sockets of6. Iridoplatinum basketlikemounting root. (Greenfield27)Figure 1.4 Dr. Greenfield’s basket design. Source: EJGreenfield, “Implantation of artificial crown and bridgeabutments,” The Dental Cosmos, 1913; 55(4):364–369.extracted teeth and donor teeth were attachedafter a healing period.1886: Dr. Edmunds was the first in theUnited States to implant a porcelain crownmounted on a platinum disc and presented atthe First District Dental Society of New York.1913: Dr. E.J. Greenfield, pioneer of endosseous implant, provided many of basic concepts of the nascent field of implantology. Hewas most known for his patented hollowcylinder implants made of wire soldered with24 karat gold and outlined surgical implantplacement technique (Figure 1.4).1939: Dr. A.E. Strock introduced the first biocompatible material, the metal alloy Vitallium,to place a series of implants at Harvard University in animals and humans. He is creditedwith the first relatively long-term successfuldental implants.1941: Dr. Gustav Dahl of Sweden is creditedwith the development of the subperiostealimplant, a metal framework that is surgicallyplaced on top of the jawbone for completelyedentulous patients (Figure 1.5).1952: Professor Per-Ingvar Brånemark discovered that titanium components can bondirreversibly with living bone tissue and coinedthe term osseointegration.1964: Commercial grade pure titanium, orcommercial pure titanium, was accepted asmaterial of choice for dental implants.
Implants 101: History, Implant Design, Parts, and Pieces 5Figure 1.5Dr. Dahl subperiosteal design.1967: Dr. Leonard Linkow of New Yorkdeveloped the blade implants and DoctorsRalph and Harold Roberts are also creditedto the development of endosteal implants(Figure 1.6).1968: Dr. Irwin Small developed the transosteal dental implant (Figure 1.7).1969: Dr. Per-Ingvar Brånemark providedthe proof of long-term success of titaniumimplants.1981: Dr. Per-Ingvar Brånemark publishedhis finding covering all the data on the animaland human clinical trials: success rate, concept,and the current design of endosteal root-formtitanium implants.1982: The Toronto Conference on Osseo integration in Clinical Dentistry created thefirst guidelines for what would be consideredthe standardization of successful implantdentistry.1986: Implants received the endorsement ofthe American Dental Association.1989: The Brånemark OsseointegrationCenter (BOC) in Gothenburg, Sweden, wasfounded. BOC’s primary mission was to pro vide treatment for patients with severe oral,maxillofacial, and orthopedic impediments.Figure 1.6 Endosteal design. Source: G Juodzbalys, HLWang, “Guidelines for the identification of the mandibular vital structures: practical clinical applications ofanatomy and radiological examination methods,” J OralMaxillofac Res 2010; 1(2):e1.Figure 1.7 Transosteal design. Reprinted with permission from Mosby’s Dental Dictionary, 2nd ed., 2008Elsevier, Inc. All rights reserved.2002: An ADA survey showed that oraland maxillofacial surgeons, periodontists,and general dentists doubled the number ofimplants performed per dentist between 1995and 2002.
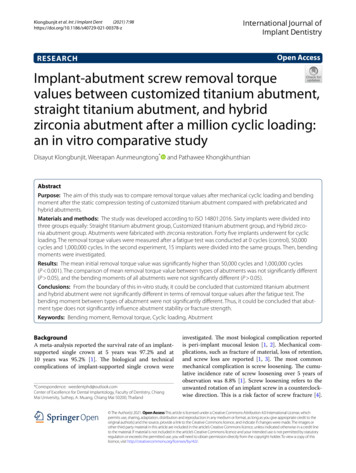
6 Peri-Implant Therapy for the Dental HygienistFigure 1.9 SEM titanium alloy implant macro/microroughened surface. Courtesy of PDT.Figure 1.8 Implants. Courtesy of BioHorizons.Today: The FDA regulates the oral anddental implants being placed, requiringimplant companies to furnish data and controlled studies under medical devices to gainfull approval.ImplantsOver the past 30 years, research has validatedthe success of osseointegrated implants as aviable alternative to fixed or removable prosthetic restorations (Figure 1.8) (4). Implantplacement in the premolar and molar are 95%successful and are considered the first choicein tooth-replacement options (5, 6). This issupported by the dental literature for manyimplant systems in every area of the mouth(7). According to Michael Tischler, et al. (8, 9),because of “the amount of edentulism currently documented, it is essential for cliniciansto incorporate dental implants into everydaypractice.” The American Association of Oraland Maxillofacial Surgeons report that 69% ofadults between ages 35 and 44 years have lostat least one permanent tooth and 43% of adultsover the age of 65 years old are missing six ormore teeth due to tooth decay, periodontaldisease, a failed root canal, or trauma (8, 9).As hygienists, these changes have evolvedinto a new phase of maintenance care for ourpatients. Before we can understand the newprotocols for our maintenance appointments,an understanding of the basics of implants andwhy most implants are made from titaniumalloy is necessary. The choice of which type ofimplant to use will be in the hands of thesurgeon, but hygienist should have an understanding of the component parts. The maincomponent parts of an implant are the fixture(design, length, shape, diameter, and surface),transmucosal abutment, and the prosthesis(Figure 1.9).Why is titanium metal used for dentalimplants? The reasons make quite a remarkable list: it is strong, lightweight, corrosionresistant, nontoxic, nonferromagnetic, biocompatible (not rejected by the human body),long lasting, and osseointegrative (joins tohuman bone), and its flexibility and elasticityare similar to that of human bone. Titaniumalloy which is what dental implants are madefrom are mainly TiAl6V4 otherwise known asmedical grade 5 and grade 23 for the greatestfracture resistance. Implants have a rough,smooth, and/or coated surface to speed up theosseointegration process. Types of treated surfaces are always evolving with the goal being
Implants 101: History, Implant Design, Parts, and Pieces 1 History, 1 Dental implant history timeline, 4 Implants, 6 Implant design, 7 Parts and pieces for implants, 10 Implant dentistry terminology, 12 Summary, 12 References, 12 professionals will be faced with different dynamics, challenges, and complications. As a hygienist the history of .