Transcription
International Journal of Health Sciences and Researchwww.ijhsr.orgISSN: 2249-9571Case ReportMaxillary Sinus Lift, PRF and SimultaneousImplant PlacementSeema Sajood Mufti1, Achyut Sinha2, Tanu Mahajan3, Ravi Shankar Yadav412Consultant Prosthodontist at Family Health Dental Centre SrinagarP.G Scholar Dept. of Prosthodontics Rama Dental College, Kanpur, Uttar Pradesh,3Professor Dept. of Prosthodontics Rama Dental College Kanpur, Uttar Pradesh,4Consultant Prosthodontist at Clove Dental Centre New Delhi.Corresponding Author: Seema Sajood MuftiReceived: 26/12/2016Revised: 23/01/2017Accepted: 30/01/2017ABSTRACTImplant dentistry has emerged as an excellent treatment modality ever since its ingress into the fieldof modern dentistry. However, the first and the foremost requirement for the placement of an implantis the presence of an adequate alveolar bone. By adequate bone, is meant that both the quality and thequantity of the bone have to be sufficient for implant placement. Posterior maxilla often presents withinsufficiently available bone for the placement of implants due to the presence of antrum of hymoremost commonly known as the maxillary sinus. This jeopardises the successful implementation ofimplant dentistry in such situations. The present article is aimed at throwing some light on how to dealwith the problem of resorbed ridges and a pneumatised sinus through the process of sinus lift and PRFplacement in order to facilitate implant placement.Key words: Sinus lift, PRF, implant placement.INTRODUCTIONAn adequate quality and quantity of bone isessential for successful implant s to an implantologist that isunique to this region. [1]Most important of these is the presence of amaxillary sinus.Lining mucosa of the maxillary sinus is theSchenedrian membrane.The structures that lie beneath the sinus arethe alveloar bone and the posterior teeth.As the edentulous span continues to atrophy,there is continuous loss of bone height anddensity and pneumatisation of sinus.When implant is inserted in this area, theinitial implant stability is poor coupled withinadequate bone height for the implantlength. This results in implant failure eitherinitially or during loading.The procedure of choice to restore thisanatomic deficiency is the maxillary sinuslift.SINUS LIFTSinus Lift is a procedure in whichthe maxillary sinus membrane is elevatedand subantral augmentation is performedwith bone graft placement. [2] The end resultbeing an improved bone height in theposterior maxilla which is more favourablefor implant placement.Two approaches:1. The direct approach2. The indirect approachInternational Journal of Health Sciences & Research (www.ijhsr.org)Vol.7; Issue: 2; February 2017322
Seema Sajood Mufti et al. Maxillary Sinus Lift, PRF and Simultaneous Implant PlacementSURGICAL TECHNIQUESCarl Misch subcategorized theimplant treatment planning into fourapproaches based on bone height in theposterior area:SUBANTRAL OPTION 1 (SA1)Conventional implant placement:There is sufficient available bone height,usually greater than 12mm to permit theplacement of an endosteal implant.No sinus lift is required in this category asimplant can be placed normally. Bone graftmay be used only to augment the bonewidth.SUBANTRAL OPTION 2 (SA2)This technique was developed by Tatum inmid 1970s.Sinus lift and simultaneous implantplacement with osteotome lift technique:Selected when there is 10-12mm ofavailable bone height. Thus the availablebone is only 0 -2 mm insufficient of theideal implant length which according tonumerous studies (Hurztler et al) is 13mmor more.Osteotome lift technique is used where theimplant is tapped to produce a green stickfracture on the sinus floor. Bone graft can beadded.SUBANTRAL OPTION 3 (SA3)Sinus membrane elevation with vised when atleast 5mm bone height ofsufficient width is present.A Tatum lateral wall approach is performedjust superior to the residual alveolar bone.A Green stick fracture is introduced in theaccess window as it is rotating inward andupward and serves as the floor of theimplant.A mixture of autogenous bone and/orallograft material is placed.Implant is then placed from the top of theridge.SUBANTRAL OPTION 4 (SA4)Sinus membrane elevation and subantralaugmentation with extended delay ofimplant placement:There is 5mm or less of bone height andthus there is not enough surface area foranchorage and stabilization of the implant.In this case, Tatum lateral wall approach isperformed.A mixture of autogenous bone and/orallograft material is placed.Implant will be placed at 8 to 12 monthslater as the new bone is allowed to migrate,differentiate, and mature.PRP & PRFReconstructivedentalsurgeonsareconstantly looking for an edge that willjump starts the healing process to maximizepredictability as well as the volume ofregenerated bone. [3]PRP (PLATELET RICH PLASMA)Several studies have shown that boneregenerative procedures may be enhancedby the addition of specific growth factors.Platelet-rich plasma (PRP) was proposedas a method of introducing concentratedgrowth factors PDGF, TGF-ß, and IGF-1 tothe surgical site, enriching the naturalblood clot in order to expedite woundhealing and stimulate bone regeneration.A natural human blood clot contains 95%red blood cells (RBCs), 5% platelets, lessthan 1% white blood cells (WBCs), andnumerous amounts of fibrin strands.A PRP blood clot, on the other hand,contains 4% RBCs, 95% platelets, and 1%WBCs.PRF (PLATELET RICH FIBRIN)PRF is a matrix of autologous fibrin, inwhich are embedded a large quantity ofplatelet and leukocyte cytokines duringcentrifugation.Platelet-rich fibrin (PRF) was firstdeveloped in France by Choukroun et al in2001. [4] It represents a new step in theplatelet gel therapeutic concept withsimplified processing, minus artificialbiochemical modification.Unlike other platelet concentrates, thistechnique requires neither anticoagulantsnor bovine thrombin (nor any othergelifying agent), making it no more thancentrifuged natural blood without additives.International Journal of Health Sciences & Research (www.ijhsr.org)Vol.7; Issue: 2; February 2017323
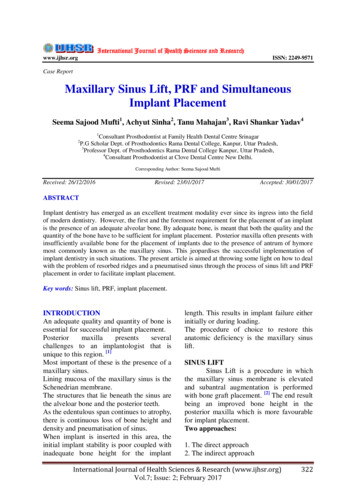
Seema Sajood Mufti et al. Maxillary Sinus Lift, PRF and Simultaneous Implant PlacementThis second generation platelet concentrateis widely used to accelerate soft and hardtissue healing.PRF is in the form of a platelet gel and canbe used in conjunction with a bone graftwhich offers several advantages like:PREPARATION OF PRFPRF preparation requires an adequateamount of whole blood, a table centrifuge, acollection kit including a 24 gauge butterflyneedle and a 10ml blood collection tube.The required quantity of blood is drawn into10 ml test tubes without an anti coagulantand centrifuged immediately.Blood is centrifuged for 12mins at 2700rpm.Because of the absence of anticoagulant,blood begins to coagulate as soon as itcomes in contact with the glass surface.Therefore for successful preparation of PRF,a speedy blood collection and immediatecentrifugation, before the clotting cascade isinitiated is absolutely essential.The resultant product consists of followingthree layers:Topmost layer consisting of acellular PPPPRF clot in middleRBC’s at bottom.CASE REPORTA 48 year old female patient reported, to thedepartment of Prosthodontics, Rama DentalCollege, with the chief complaint ofdifficulty in chewing on the right side due tomissing teeth in the right upper back toothregion.On oral examination it was found that theright maxillary first and second molars weremissing.On radiographic examination (Fig.1) theavailable bone height in this molar region(16 region) was found to be approximately10mm from the maxillary sinus lining.After a thorough oral and radiographicexamination, two stage surgeries wasplanned.It was decided to lift the sinus lining with anindirect approach through alveolar crest andsimultaneous implant placement.An endosteal implant of 10mm length and5mm diameter was selected.Afterperforming the incision and raising a fullthickness flap, (Fig. 2) the indirect approachbegins with a pilot drill to mark the implantsite.(Fig.2) Incision and full thickness flap(Fig . 3) Radiograph showing paralleling pin at implant site.(Fig. 1) Radiographic examination showing the implant siteFirst the site was prepared upto 5mm. Aparalleling pin was placed and an IOPAInternational Journal of Health Sciences & Research (www.ijhsr.org)Vol.7; Issue: 2; February 2017324
Seema Sajood Mufti et al. Maxillary Sinus Lift, PRF and Simultaneous Implant Placementradiograph taken (Fig.3). Since there wasstill ample amount of bone, the preparationwas extended further upto 8 mm with thetwist drillit was decided to achieve the remainingheight with the help of osteotomes. ( Fig.5)(Fig. 5) Osteotomes used to lift the sinus floor(Fig .4) Radiograph showing remaining space of 1 to 2 mmbetween osteotomy and maxillary sinus floor.Now after drilling 8mm the bone remainingbetween the osteotomy and the sinus floorwas about 1 to 2 mm. (Fig. 4)Further drilling for 2 to 3 mm for placingthe implant slightly subcrestal would haveresulted in perforation of the sinus floor. SoBefore using the osteotome a small amountof allopastic bone graft material (Fig. 6) wasplaced into the implant site. This materialalso acts as a shock absorber when tappingof osteotome is done with the mallet.(Fig. 6) Alloplastic graft material placed at the implant site.(Fig. 7) PRF being pulled out of the test tube(Fig. 8) Remaining RBC’s being scrapped off from the PRFInternational Journal of Health Sciences & Research (www.ijhsr.org)Vol.7; Issue: 2; February 2017325
Seema Sajood Mufti et al. Maxillary Sinus Lift, PRF and Simultaneous Implant PlacementOnce the required bone height of 10 mmwas obtained by osteotomes , the PRF waspulled out of the test tube (Fig.7) , theremaining RBC’c were scrapped off (Fig.8) and the PRF was placed at the preparedosteotomy site.(Fig. 9) Radiograph showing endosteal implant secured atthe implant siteThe primary stability of the implant waschecked, cover screws placed, implantswere covered with mucosa and sutures wereplaced. (Fig. 10)DISCUSSIONIt has been observed that manysurgical techniques exist that can help toovercometheexpectedanatomicaldifficulties encountered during implantation.However, it is important to remember thedesired treatment outcome and to explore allthe possible solutions.A good evaluation of both thepatient’s desires and the availablepossibilities and by choosing a suitabletechnique, keeping the technique as simpleand as predictable as possible, the likelihoodof success increases greatly even incompromised situations.Next the endosteal implant was gentlyplaced in the prepared site.(Fig. 9 )This further pushed and secured the PRFupwards.(Fig. 10) Implant site covered with flap and secured with sutures.REFERENCES1. Garg A. Augmentation grafting of themaxillary sinus for the placement ofdental implants: Anatomy, physiologyand procedure. Implant Dent 1999;8 (1):36-6.2. Small SA, Zinner ID, Panno FV et al.Augmentation of the maxillary sinus forimplants:- Report of 27 patients. Int JOral Maxillofac Implants 1993;8: 5238.3. Long term effects of vertical boneaugmentation: a systemic review. JAppl Oral Sci 2016; 24 (1): 3-17.4. Toffler M, Toscano N, Holtzclaw D,Corso MD, Ehrenfest DD. IntroducingChoukron’s Platelet Rich Fibrin(PRF)toReconstructive Surgery Milieu. Journalof implant and advanced clinicaldentistry 2009; 1(6): 21-30.How to cite this article: Mufti SS, Sinha A, Mahajan T et al. Maxillary sinus lift, PRF and simultaneousimplant placement. Int J Health Sci Res. 2017; 7(2):322-326.***********International Journal of Health Sciences & Research (www.ijhsr.org)Vol.7; Issue: 2; February 2017326
placement of an endosteal implant. No sinus lift is required in this category as implant can be placed normally. Bone graft may be used only to augment the bone width. SUBANTRAL OPTION 2 (SA2) This technique was developed by Tatum in mid 1970s. Sinus lift and simultaneous implant placement with osteotome lift technique: