Transcription
PRACTICEIN BRIEF Dental implant placement must be both biologically and restoratively driven.Dental implants should only be placed following a comprehensive examination andaccurate diagnosis.The deficient osseous ridge must be reconstructed prior to implant placement.4Surgical guidelines for dental implant placementM. Handelsman1The goal of an implant supported reconstruction is to obtain optimal aesthetics and function. In order to achieve this,visualisation of the final restorative reconstruction is necessary prior to beginning treatment. The term ‘restorative-driven’treatment planning has been used to identify this process.1 It requires a team approach of specialists, who can develop a multidisciplinary treatment plan. It starts with an accurate diagnosis, which will lead to a prognosis of each individual tooth and theoverall dentition. This information will help the clinician develop the treatment options suitable for tooth replacement. Onlywhen the goals have been defined can the sequence of therapy be established. Working backwards from the wax-up of the finaldiagnostic model of the proposed treatment assists not only with the management of the complex case, but will help avoidmishaps.2 Effective communication between the team and the patient is extremely important. Understanding the patient’sexpectations is key to a successful outcome. Deciding that these expectations are realistic requires a correct diagnosis and aninter-disciplinary treatment plan that is logical. This approach takes time and requires a comprehensive treatment discussionbetween the team members, and then a thorough case presentation to the patient.3 Only then will the patient begin tounderstand the extent of their problem and the options available to reconstruct their mouth.IMPLANTS1. Rationale for dental implants2. Treatment planning of implants inposterior quadrants3. Treatment planning of implants inthe aesthetic zone4. Surgical guidelines for dentalimplant placement5. Immediate implant placement:treatment planning and surgicalsteps for successful outcomes6. Treatment planning of theedentulous maxilla7. Treatment planning of theedentulous mandible8. Impressions techniques forimplant dentistry9. Screw versus cemented implantsupported restorations10. Designing abutments forcement retained implant supportedrestorations11. Connecting implants to teeth12. Transitioning a patient fromteeth to implants13. The role of orthodontics inimplant dentistry14. Interdisciplinary approach toimplant dentistry15. Factors that affect individualtooth prognosis and choices incontemporary treatment planning16. Maintenance and failuresDIAGNOSISThe restorative dentist will develop and directthe plan after gathering data, which includesa complete medical and dental history, clinical findings, photographs, mounted diagnosticcasts and radiographs. Consultation with otherspecialists (periodontist, oral surgeon, orthodontist, endodontist) regarding the periodontaland endodontic health, and any occlusal, skeletal and space problems will be required.A correct diagnosis with long-term prognostic information is mandatory, in order to develop an interdisciplinary treatment plan. All thetreating specialists on the team need to collaborate their findings, which includes the followingexaminations.A. Periodontal examination (Figs 1-8)A comprehensive periodontal examinationincludes the soft and hard supporting tissues ofthe dentition. The patient’s tissue biotype is classified according to how thick or thin the supporting bone and gingival soft tissues are defined.Becker and Oschenbein4 classified three distinct1Diplomate: American Board of Periodontology / Private Practice:Santa Monica, CaliforniaCorrespondence to: Dr Mark Handelsman, 1245 Sixteenth Street,#206, Santa Monica, CA 90404, USAEmail: markhandelsman@aol.comRefereed Paper British Dental Journal 2006; 201: 139-152DOI: 10.1038/sj.bdj.4813820BRITISH DENTAL JOURNAL VOLUME 201 NO. 3 AUG 12 20063p139-152.indd 139types: pronounced scalloped, scalloped and flat.A thin periodontium will be pronounced scalloped or scalloped. A thick periodontium willpresent with flat gingival architecture, usuallysupported by thick buccal and lingual plates ofalveolar bone. A thin skeletal pattern with scalloped architecture will have root dehiscence andfenestrations even in a healthy periodontium. Ifperiodontal disease is present, it is important toestablish the attachment level (probing depthsand gingival recession) as well as any contributing factors, such as mucogingival problems(lack of keratinised attached tissue) and furcation involvement, which will alter the prognosisof the remaining teeth. It is critical to measurenot only probing depths, but identify the levelof the crestal alveolar bone. Kois5 classified ahigh crest when the crestal bone level is close tothe CEJ (delayed passive eruption). The normalcrest is defined as 2 mm from the CEJ and thelow crest is present in patients with recession.Sounding to bone is the best clinical parameter to help identify the attachment level. Thisis extremely important in the aesthetic zone,when considering replacing partially edentulous teeth. The interproximal attachment levelon the teeth adjacent to a future implant sitewill dictate the future gingival architecture.6In the aesthetic zone it is extremely importantto identify the amount of teeth and soft tissuesvisible not only from the frontal view, but alsofrom the lateral view, both with the lip at rest1392/8/06 10:15:57
PRACTICEand also when smiling. Uneven gingival architecture, the position of teeth relative to the archshape and opposing occlusion will all affect anddictate the decision making process.The presence of bone loss due to periodontal disease or trauma will greatly affect the outcome of treatment. If teeth are already missingthen the amount of ridge collapse needs to bemeasured according to both horizontal and vertical collapse. (Siebert Classification type I, IIand III.) Lekholm and Zarb7 classified the hardtissue according to the shape of the ridge (morphology) and the bone quality; shape a–e andtype 1-4 respectively. This will be discussed ingreater detail later in the article as relating tosurgical technique.If the prognosis of teeth is deemed hopelessdue to periodontal, endodontic or non-restorability factors, then anticipating the amount offuture ridge collapse needs to be estimated. Inthis case, it is extremely important to identifythe tissue biotype and the underlining missingbone, which will help determine the prognosisand steps necessary to preserve or rebuild thedesired soft and hard tissue architecture aftertooth loss. Thick tissue is much more forgiving, easier to manipulate and provides a morepredictable aesthetic outcome, as compared tothin tissue which is more likely to shrink. Deciding when to extract a tooth is easy when it ishopeless, but often more heroic attempts to saveteeth that are broken down with a questionableprognosis is not as simple. In order to preservethe alveolar bone for implants, sacrificing teeth(early extraction) requires a change of thinkingas compared to previous philosophical treatment decisions.B. Occlusal analysisPatients with occlusal wear or abfraction typedefects due to clenching or bruxism shouldbe identified. The parafunctional habits willgreatly affect the outcome and longevity ofthe type of reconstruction planned. The opposing occlusion along with the type of restorativematerials selected for the final prosthesis willaffect the ability of the bone-implant interface to withstand the occlusal load. In the periodontally compromised patient, loss of teethwithout replacement leads to lack of posteriorsupport. This often causes an unstable occlusalscheme with mesial drifting of posterior teethand flaring of anterior teeth with a loss of vertical dimension. A full examination includes notonly the mobility of remaining teeth, but alsothe occlusal scheme and guidance in lateral andprotrusive movements. Over-eruption of anyteeth will cause occlusal interferences and alsodecrease the inter-occlusal space necessary forimplant restorative components. Lack of restorative space is a major contributor to mechanical failure of implant restorations. Mounteddiagnostic casts are used to evaluate the occlusion, the edentulous space ridge relationship tothe adjacent teeth and the opposing dentition.The amount of vertical and horizontal over1403p139-152.indd 140lap as well as the restorative space available isextremely important. Replacing teeth in partially edentulous spaces, without comprehensivecare of the remaining dentition, is sure to causefailure in the long term.C. EndodonticThe endodontic integrity and vitality of remaining dentition must be established. Any pathological changes, such as periapical lesions andexisting root canals that are incomplete need tobe evaluated. Any teeth with a poor endodonticprognosis should have a thorough risk assessment completed, so as not to jeopardise futureimplant sites.D. RestorativeThe integrity of all existing restorations shouldbe evaluated. This must include margin integrity and soft tissue response to sub-gingivalplacement. Teeth with biologic width violation,that will require surgical crown lengthening,will affect the future level of the osseous crest atsites adjacent to implants. In the aesthetic zone,it is important to anticipate the future gingivalcontours of the teeth adjacent to the implantsite. Teeth that are fractured, broken downbeyond predictable restoration, or have compromised support will be given a poor or hopeless prognosis. The strategic value of each toothneeds to be determined, prior to removal. Oftenin complex cases, even teeth with a poor prognosis can be kept in the initial phases to supporta fixed interim prosthesis, while implant healingprogresses. This phased approach of sequentialextraction will help manage the complex case,sometimes through long periods (two years)while site development and healing of implantsites is progressing.E. OrthodonticAnalysis of the restorative space is importantregarding future tooth restoration size, but it isequally important to analyse the position andangulation of the roots in the alveolar bone.Drifting and tipping of remaining teeth willoften present problems with space mesially-distally. The orthodontist needs to be given clearinstructions when opening or closing spaces inregards to root positions. Taking radiographsduring treatment will give useful informationto the treating team, prior to appliance removaland completion of treatment. It is always preferable in aesthetic cases to complete the orthodontic care prior to implant placement. In casesmissing posterior teeth, provisional interimimplants can be placed to help the orthodontistestablish anchorage. The final implants shouldonly be placed posteriorly, if the orthodonticwax-up of the final result allows for correctpositioning, without compromising the endresult.F. Radiographic examination. (Figs 28-33)The preliminary exam will include a set of fullmouth periapical and bitewing radiographs. ABRITISH DENTAL JOURNAL VOLUME 201 NO. 3 AUG 12 20062/8/06 10:17:17
PRACTICEpanorex is helpful as well, but limited comparedto 3-D CT scan imaging. Once the patient hashad the initial consultation and accepted theproposed options, a diagnostic wax-up of thefinal proposed treatment will be a template tofabricate a radiographic guide. This radiographic guide can be placed in the mouth at the timeof the CT scan. Transferring the restorative template on to the radiographic images is the mostuseful information for determining the surgicalplan. Lack of bone and ridge collapse both horizontally and vertically can be accurately measured. The surgical needs can be identified andthe most predictable options can be presentedto the patient prior to beginning treatment. Thegoals of the final reconstruction, whether fixedor removable, can be determined. The treatmentexpectations can be presented to the patient,with realistic steps of what can and cannot beaccomplished. Only then can the treatment planin a phased approach, be determined by all thetreating doctors on the team. All financial obligations, treatment consent as well as aestheticgoals are established prior to taking any furthersteps.Occasionally, when questionable teeth arestill present, it may be beneficial to have a CTscan prior to removing teeth. This can help maketreatment decisions regarding surgical optionsof timing of implant placement (see discussionlater in article).Pre-surgical planningViewing the CT images which have the crosssectional reformatted images of the bonequantity and quality at each desired implantsite, allows the surgeon to develop the surgical plan. The question most often asked — ‘DoI have enough bone?’ — can be answered withan educated answer. The goals of the restorative dentist can be accomplished or cannot beachieved. In complex fully edentulous cases,whether fixed or removable reconstruction willbe the best outcome can be determined. The surgeon can then modify the radiographic guide tobe used as a surgical guide on the day of surgery. Recent developments in CAD-CAM technology allow the team to perform pre-surgicalplanning on a virtual model and then transferthis information to a clinical surgical guide toassist accurate placement of implants (eg NobelBiocare ARK, Simplant).The hard tissue classification by Lekholm andZarb defined quantity and quality of the edentulous ridge.QualityType 1: Almost the entire jaw is composed ofhomogenous compact bone.Type 2: A thick layer of compact bone surroundsa core of dense trabecular bone.Type 3: A thin layer of cortical bone surroundsa core of dense trabecular bone of favourablestrength.Type 4: A thin layer of cortical bone surrounds acore of low density trabecular bone.BRITISH DENTAL JOURNAL VOLUME 201 NO. 3 AUG 12 20063p139-152.indd 141Quantity: Ridge shape a–e.Shape ‘a’ represents no bone resorption, while‘e’ represents advanced ridge resorption.The pattern of resorption in the anterior maxilla (Figs 5–8) advances posteriorly and superiorly, which greatly affects the aesthetic zoneand lip support. The pattern of resorption of theposterior ridges greatly affects the occlusion andhorizontal overlap of the dentition8 (Figs 9-13).SURGICAL GUIDELINES — TOOTH OR TEETHALREADY MISSINGAdequate osseous ridgeThe Brånemark surgical protocol9 establishedosseointegration as an extremely predictableoption for tooth replacement with excellentlong term stability. Many implant systems havesince been developed which use this concept. Thenumerous shapes and sizes of implants availablefor use on patients today continue to change andare overwhelming. It is extremely important forall members of the team to discuss which components are to be used surgically and restoratively,so that the benefits and limitations are defined.Whether the prosthesis will be screw retained orcement retained can affect the axial inclinationand angle of placement. Due to common anatomical limitations post-extraction (concavitiesand collapse of the ridge circumference), usingcement retained restorations allows greater flexibility at the time of surgical placement.Flap designThe original Brånemark protocol required avestibular flap with a two stage approach. Theimplant was placed and buried under the softtissue and after an adequate period of healing(three months mandible, six months maxilla), asecond stage surgery was performed with crestal incisions to expose the fixtures and connecta trans-epithelial abutment. After adequate softtissue healing, the restorative dentist could fabricate the prosthesis. One stage surgical protocols were developed by ITI in Switzerland10 thatallowed the implant fixture to extend throughthe soft tissues during the period of initial healing. This protocol was duplicated and shown tobe effective using a two stage system with thesame predictability.11 Today this trend continues with most implants placed with a one stageprotocol allowing adequate time for healingprior to loading the fixtures. Using the one stagetechnique requires a crestal incision or even aflapless approach, drilling directly through thesoft tissues. Obviously, deciding which casesare suitable for the flapless technique is the keyto a successful outcome; adequate bone widthwith plenty of keratinised soft tissue is desired.Compromising the site while drilling due to lackof visibility is not advised. In the aesthetic zoneit is important to maintain adequate thicknesson the buccal aspect of the implant for longterm stability of the soft tissue contours. Usually this area lacks enough tissue due to resorption subsequent to tooth loss, and augmentation techniques are required. The L. Abram’s roll1412/8/06 10:17:46
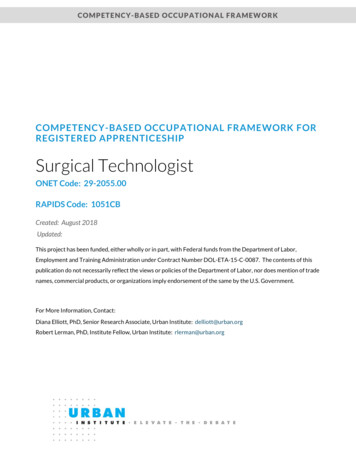
PRACTICEFig. 1 (left) Anterior X-section ofthick periodontium with high crest(bone at level of CEJ)Fig. 2 (right) Thin periodontiumwith low crest (Note the bonedehiscence on the buccal surface)Fig. 3 (left) Periodontitis withadvanced bone loss and probingdepths; expect vertical ridge collapseafter tooth extractedFig. 4 (right) Recession; attachmentloss with advanced horizontal boneloss; expect even larger ridge defectafter tooth lossFig. 5 (left) Type ‘a’ ridge (thickperiodontium) with no collapseFig. 6 (right) Loss of vertical heightafter extraction of teeth withmoderate to advanced periodontitis(normal to thick periodontium). Thiswill also present with loss of papillaheight, due to previous interproximalbone defectFig. 7 (left) Expected collapse ofridge after extraction with thinperiodontium (even in healthyenvironment)Fig. 8 (right) Shape ‘c’ or ‘d’. Thinperiodontium with pronouncedscalloped biotype and disease (seeFigs 3-4) will usually shrink more,leaving concavity type defect withknife edge ridgeFig. 9 (left) Posterior x-sectionshowing horizontal overlap and ridgerelationship in healthFig. 10 (right) Tooth loss withminimal ridge collapse. (Type ‘a’ and‘b’ ridge shape)1423p139-152.indd 142BRITISH DENTAL JOURNAL VOLUME 201 NO. 3 AUG 12 20062/8/06 10:19:15
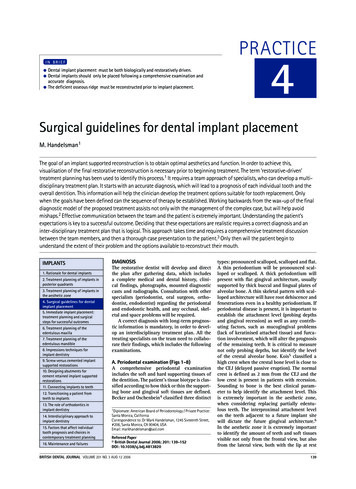
PRACTICEFig. 11 (left) Further resorptioncreates greater interarch distancewith less bone available to place onlyshorter implantsFig. 12 (right) Minimal resorptionallows occlusal scheme to remain thesame as prior to extraction, and idealemergence for crown contoursFig. 13 (left) Buccal collapse of theridges (left) requires implants to beplaced in a more lingual position. Thiscreates restorations with buccal overcontouring and unfavourable loadingconditions on the implant. Thealternative option is to restore withan x-bite relationship. Note on theother side of diagram, short clinicalcrowns require countersinking of theimplants to allow adequate space forrestorative componentsFig. 14 (right) Intra-oral graft sitesinclude ramus and chinFig. 15 (left) Posterior maxillapresents with enlarged sinus andnot enough bone height to placeimplants. Note minimal amount ofvertical ridge height collapseFig. 16 (right) Sinus Lift usingwindow approach through the lateralwall. After adequate bone healing(four to six months), implants arethen placed. Simultaneous bonegrafting and implant placement isa risker procedure. Note crown toimplant ratio will be favourableFig. 17 (left) Note more advancedridge resorption. Sinus Lift withoutreconstruction of ridge height leadsto less favourable crown to implantratio. Placement of the most mesialimplant adjacent to the cuspid toothon the incline creates problem withInterproximal tissues and forcesimplant placement slightly moredistal than ideal in order to protectattachment on distal of cuspidFig. 18 (right) Onlay block graftwith fixation screws to reconstructthe ridge height and improve crowncontoursFig. 19 (left) After adequatehealing, screws are removed andimplants are placed. Note idealcrown/implant ratioFig. 20 (right) Posterior maxilla withideal bone height and widthBRITISH DENTAL JOURNAL VOLUME 201 NO. 3 AUG 12 20063p139-152.indd 1431432/8/06 10:19:48
PRACTICEtechnique12 is often used to transfer the crestalthicker tissue onto the buccal aspect, rather thanusing a punch technique (flapless approach)which is subtractive.Using a two stage protocol in the aestheticzone also allows for an additional opportunityfor surgical intervention with further hard orsoft tissue grafting procedures. Langer13 introduced the sub-epithelial connective tissue graftas a predictable technique for augmenting thintissue and it is especially useful when minorridge resorption is present. The most commondonor site is the palatal tissue mesial to the firstmolar. Another popular donor site is the tuberosity tissue. This area is especially desirable whena thicker graft is needed for ridge augmentation procedures (inlay or pouch technique)14 inthe anterior aesthetic zone. Palacci15 has alsodescribed rotated flap techniques for papillaregeneration. It is always important to define thetype of defect, and realise that building the supporting bone beneath the soft tissue will producethe most predictable outcome. The bony architecture provides the scaffold that supports thesoft tissue around proper implant positioning.POSITION AND ANGULATION OF IMPLANTPresurgical analysis has determined the bestavailable sites for placement. In the partiallyedentulous case, being aware of the root morphology and inclination of teeth adjacent tothe implant site is crucial. If a radiographicguide was used at the time of CT scan and thenadapted for use as a surgical guide, mishaps willbe prevented. If a surgical guide is fabricatedwithout the knowledge of the root positions orbony deficiencies, then careful interpretationand adjustments by the surgeon is required. Theinitial drilling (round bur) starting point can bemoved and the angulation of the implant tippedto avoid bone dehiscence or fenestration. Themore palatal the movement, the deeper sub-gingivally the implant platform must be positionedto accommodate for the emergence of the restorative components through the soft tissue. Idealdimensions16 are 3–4 mm subgingival, with thebuccal aspect of the implant platform at least 1mm or more palatal or lingual to the future buccal aspect of the restoration at the level of thegingival margin. Placing a wider platform in theanterior aesthetic region provides for a smoothergingival restorative interface (platform does nothave to be as deep), but invites greater risk ofapical migration of the soft tissue margin. Theconcept of ‘platform switching’ – using a narrower restorative component on a wider implantplatform (possible only with some implantsystems, eg 3i) – is interesting.17 It appears tohelp support the soft tissue and prevent crestalresorption of the bone at the level of the implantplatform. At this time further research is needed.Dense boneDense bone (Type 1 & 2) requires careful attention to drilling with adequate irrigation in ordernot to overheat the bone. Care should be taken1443p139-152.indd 144to debride the osteotomy site from bone debrisand to widen the site to the manufacturer’s recommended diameter prior to tapping the site.Placing the implant into too tight a site can leadto failure due to pressure necrosis. The shape ofthe implant, parallel walled vs. tapered will alsogreatly affect the tightness (primary stability).Softer boneType 3 and 4 bone requires modification of thedrilling protocol. Care must be taken to underprepare the osteotomy site. Over-preparationor inadvertent implant angulation changescan preclude placement of the implant. Usingthe Osteotome technique18 can also help initial stabilisation by compressing the availablesoft bone instead of compromising the site withdrilling. Tapered implants have an advantage insofter bone due to the wedging effect at the timeof placement. The tapered implant is more challenging at the time of placement, because thedepth of the prepared site needs to be exactlyat the level of where the desired final positionof the implant needs to be placed. As opposedto a parallel wall implant that can be placeddeeper if desired, due to the ability to sink theimplant into the prepared site. The twist drillsfor the parallel wall implants have markings,which prepare the depth slightly longer thanthe implant length. Due to this design and extratip at the end of the drill, care should always betaken when drilling above vital structures suchas the alveolar canal in the posterior mandible.Bi-cortical fixation in softer sites helpsanchor the fixture especially in the posteriormaxilla. Engaging the sinus floor is suggestedto achieve this anchorage.Countersinking into the crestal bone maycause loss of initial stabilisation at the time ofplacement. The need to countersink the implantis usually restorative driven for aesthetic andemergence purposes or due to lack of restorative space. The original protocol requiredcountersinking to protect the implant fromtrans-mucosal forces generated by removable appliances over the implant head. In softerbone, it is preferable to place the platform ofthe implant at the crest or supra-crestal if spaceallows for adequate emergence.The deficient osseous ridge (Figs 34-61)Lack of vertical heightAnterior maxilla: Vertical resorption of theridge will affect the aesthetic result in partiallyedentulous cases. In fully edentulous cases theamount of loss might limit treatment to removable overdentures.Options for surgical correction include: Onlay bone grafting Distraction osteogenesis.The onlay block graft19 requires an autogenous block of bone be taken from either intraoral sites (Ramus or chin) (see Fig. 14) or extraoral site (iliac crest or calvaria). The greater thedefect, the more bone required. Analysis of theBRITISH DENTAL JOURNAL VOLUME 201 NO. 3 AUG 12 20062/8/06 10:20:16
PRACTICEdimensions required will dictate which donorsite is preferable. Extra-oral sites require general anaesthesia and increase the risk of greatermorbidity. Intra-oral block grafts are better suited for partially edentulous situations. The blockof cortical cancellous bone is carefully adaptedto the recipient site and fixated with screws tostabilise the graft during the healing period.Building vertical height is the least predictableof all the grafting options.Distraction Osteogenesis20 allows the existing bone to be transferred to a more coronalposition after surgical osteotomy cuts andplacement of a device that is activated daily inthe mouth. After several weeks of movement,the bone is left to mature for a few months priorto implant placement.Posterior maxilla: The posterior maxilla has historically always been the most challenging site toachieve success. The most common site for toothloss in the periodontally compromised patient isthe maxillary molars due to furcation involvement.21 Due to a combination of periodontal boneloss and sinus proximity, limited bone height isusually available for implants (Fig. 15). The boneis also usually soft (type 3 or 4), which makes initial stabilisation difficult to achieve. Several techniques have been developed and perfected overthe last decade to improve the surgical options inthe posterior maxilla (Figs 16-24).The Sinus Lift procedure22 reported byBoyne et al. showed that it is possible to openthe maxillary sinus through the lateral wall,elevate the sinus membrane and pack bonegrafting material into the space. Many types ofbone grafting materials are available. Autogenous bone has always been the most predictable option that has set the gold standard.Intra-oral bone can be harvested from the chin,ramus or tuberosity areas. This bone is groundand the particulated graft material is best combined with an osteo-conductive material of thesurgeon’s choice (eg Hydroxy-apatite, Bio-ossor freeze dried bone). Using Platelet Rich Plasma23 to aid the healing response is an additional option. It is more predictable to performthe sinus lift graft, and then wait 5-6 monthsfor healing prior to implant placement. If 5 mmor more of bone height is available, simultaneous implant placement with sinus lift and bonegrafting is possible, with less predictability. If 7or 8 mm of height is available, then placementof the implants with an osteotome techniquefor increasing the length of implant is possible(see Figs 20-24). The protocol calls for drillingthe initial twist drills at least 3 mm short ofthe sinus floor. The osteotome is placed intothe osteotomy. The sinus floor is in-fractured,thereby raising the membrane and creatingspace for the graft. Bone graft material canthen be pushed into the preparation site priorto placing the implant. This technique is popular, because it seems less invasive as comparedto the sinus lift via the lateral wall technique,but obviously it requires careful patient selection. It is a technique sensitive procedure, goodBRITISH DENTAL JOURNAL VOLUME 201 NO. 3 AUG 12 20063p139-152.indd 145for single tooth replacement, but with lesspredictability, due to the greater potential forsinus membrane perforation.Posterior mandible: The inferior alveolarnerve needs to be visualised in order not to causenerve damage such as paraesthesia. It often limitsimplant placement to short wide implants. Alternative options are the nerve transposition procedure24 which has a high morbidity and rate ofnerve damage, or to consider distal cantileveringof the prosthesis off implants placed mesial to theforamina. Distraction osteogenesis can also beused if inter-arch space is not a problem.Lack of horizontal widthAnterior maxilla: The pattern of resorption usually creates knife-edge ridges or ridges that aretoo thin due to concavities (Fig. 8). The anterior incisal foramen is sometimes large and canrestrict implant placement in the maxillary central positions (Fig. 37).Knife-edge ridges are best treated with veneergrafts19 using an intra-oral block of corticalcancellous autogenous bone stabilised with fixation screws (Figs 25-26). Unlike onlay grafts,these veneer grafts are more predictable. Concavity defects can be treated with block grafts,but these also respond favourably
3. Treatment planning of implants in the aesthetic zone 4. Surgical guidelines for dental implant placement 5. Immediate implant placement: treatment planning and surgical steps for successful outcomes 6. Treatment planning of the edentulous maxilla 7. Treatment planning of the edentulous mandible 8. Impress