Transcription
SCIENTIFIC ARTICLEMaxillary protraction for early orthopediccorrectionof skeletal ClassIII malocclusionPaul W. Major DDS, MSc, MRCD(C)H.E. EIBadrawy,MS, HDD, DDSAbstractThe clinical use of combinedmaxillary expansion and protraction headgearis reviewed. The diagnostic considerationsnecessaryfor appropriatecase selection are discussed. A description of appliancetechniqueis providedin sufficient detail tofamiliarize the pediatric dentist with the associatedclinical procedures.(Pediatr Dent 15: 203--07, 1993)IntroductionDifferential diagnosisTreating the developing Class III skeletal malocclusionis one of the more challenging problems facing clinicalorthodontists. The incidence of this type of malocclusionin a major Canadian city was found to be approximately11%of the population with no apparent gender difference.Someracial groups, in particular Asians, have a muchhigher frequency. It has been estimated that in Japan 313%of the population have a Class III skeletal malocclu2sion.Manypractitioners avoid early treatment of the Class skeletal malocclusion because they believe the condition is caused by mandibular overgrowth and thereforemandibular surgery is inevitable. Attempts to restrictmandibular growth using chin cup retraction deviceslargely have been abandoned. Recent studies suggest that3malocclusionscorrected in this wayhave limited stabilityand latent mandibulargrowth and a return to the pretreat4, 5ment condition are common.There is also concern about the long term-effects of chincup therapy on temporomandibular joint health. Posterior condylar displacement has been implicated in developing TMJinternal derangement,6 and it is reasonable topostulate that forces of sufficient magnitude to inhibitcondylar growth may cause the capsular ligaments tostretch, increasing the risk of TMJdysfunction.Several recent studies have shownthat the majority ofClass I malocclusions exhibit maxillary retrusion. Ellis7 found that 65%of their sample exhibitedand McNamaraa retrusive maxilla. Although this was associated withmandibular protrusion in 30%of the cases, it was alsoassociated with normal mandibular skeletal position in25%of the cases. Similarly Guyeret al.s reported that oftheir total Class I sample, 9.5% had simple maxillaryretrusion and 34%had combined maxillary retrusion andmandibular protrusion. In view of the high frequency ofmaxillary retrusion, managing manyClass III malocclusions should include maxillary advancement as a majorobjective. Early intervention with orthopedic maxillaryprotraction provides a nonsurgical alternative.In treatment planning, correction of a Class III malocclusion several diagnostic features should be considered.FunctionalassessmentAnaccurate diagnosis of the relationship of maxilla tomandible in centric relation is very important. Anteriorpositioning of the mandiblegenerally results from abnormal tooth contacts that force the mandible forward. Patients presenting with a Class I skeletal pattern, normalfacial profile, and Class I molarrelation in centric relation,but a Class IlI skeletal and dental pattern in centric occlusion very often have abnormalincisor positioning. Treatment of this pseudo Class III problem should be undertaken as early as possible by advancing the maxillaryincisors and/or retracting the mandibular incisors. Evena true Class III malocclusion can appear muchmore serious if there is an anterior path of tric analysis is commonlyused to differentiate between maxillary retrusion and mandibular protrusion. The ANBangle in Class III samples is generallynegative with a smaller than normal SNAangle (Fig I a,b).Unfortunately cephalometric analysis maybe potentiallymisleading. Sue et alo 9 reported that when SNAand SNBwere used, the mandible was implicated as the majorcontributor, but whenA point to Facial Plane and Nasionperpendicular to A point were used, the majority of caseswere dassified as maxillary retrusion. Individual variationsin cranial base flexure and anterior/posterior displacementof Nasion(N) alter the ANBangle2 Alternative cephalometric values to assess maxillary anterior/posterior relationship1to the mandible and cranial base include Wits appraisaUeffective midfacelength, 12 Frankfort horizontal to NA, Apoint to Nasion perpendicular, 12 and A point to FacialPlane. 13 All cephalometric measurementsmust take intoaccount the amountof anterior functional shift from centric relation to centric occlusion. If the lateral cephalogramis taken with the patient in centric relation, any increasedvertical dimension must be taken into account.Pediatric Dentistry: May/June,1993 - Volume15, Number3 203
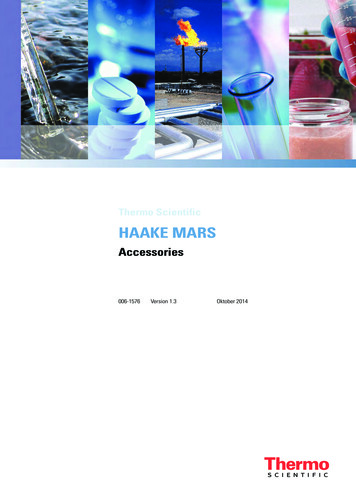
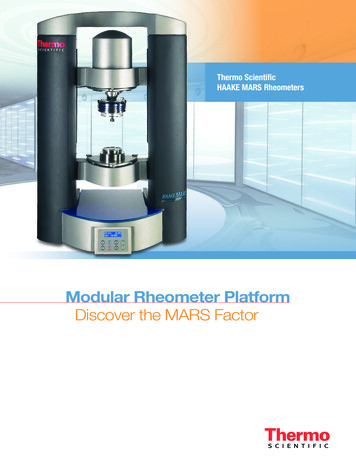
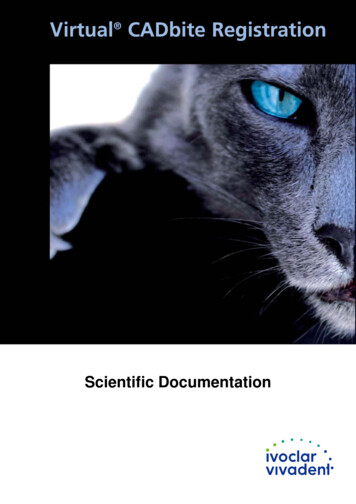
%SNASNBANBCauc Patient Normal 75 81 7979 2-4SNASNBANBCaucasianPatient Normal 81 81 8579 -4 2Fig1. A. (left) ClassIII skeletalpatterndueto leandassociatednegativeANBangle.)B. (right) ClassIII skeletalpatterndueto mandibularprotrusion.(Notethe .Clinical assessmentBecause the treatment objective is to optimize fadalesthetics, treatment decisions should be based more on thepatient’s facial features than cephalometric values. A facial evaluation involves an analysis of facial proportions,chin position, and midfaceposition. 14 Maxillary deficiencyis evidenced by flattening of the infraorbital rim and thearea adjacent to the nose. Very often patients will appearto have droopy lower eyelids and show excessive sclera.Lookingat the patient in profile, block out the lower lipand chin with your hand to accentuate the midface. In awell-balanced face there is a convexity extending from theinferior border of the orbit through the alar base of thenose down to the comer of the mouth. A straight orFig2. Normalfacial proportions.concave tissue contour indicates a midface deficiency.Similarly, chin position can be evaluated by using twofingers to block out the upper and lower lips. The chinshould not be positioned anterior to a vertical line extending down from soft tissue Nasion. The lip posture isassessed for evidence of overclosure, amountof incisordisplay at rest and whether the lip looks adequately supported by the maxilla. It is importantto realize that facialconvexity normally decreases as the patient matures. Adegree of chin prominence that would be normal in anadult maysuggest a Class lII skeletal pattern in a youngchild.Vertical facial proportions and skeletal relationshipsalso should be assessed. Clinically, vertical proportionsFig 3. stry:May/June,1993-Volume15, Number3A - Frontomaxilla yB - ZygomaticotemporalC- ZygornatJcomaxi]la.,yD o Pte ygopalatineFig4. Orientationof thecircum-maxillarysutures.
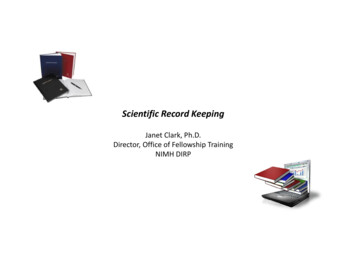
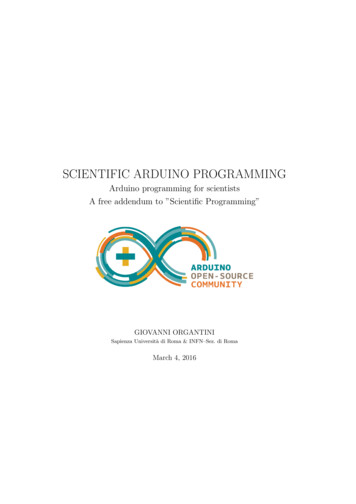
can be assessedby comparing themidface height tothe lower faceheight. The distance from softCentero! tissue Nasion toResista nce )Subnasal (wherethe nose joins theupper lip) shouldequal the distancefromonentsSubnasal to soft( /ForceCo’oP1 tissue Mentonis(Fig 2). NandaFig 5. Forcecomponentsassociatedwith reported that thepatterns of anteprotractionheadgear.rior facial proportions are established at an early age and are maintained during growth.Growthdirection is difficult to accurately predict, butgrowth trends maybe clinically or cephalometrically assessed by measuring the Frankfort plane angle. 16 Patientsexhibiting excess vertical growth generally will have alarger than normal mandibular plane angle (Fig 3). Othercephalometric assessments of growth direction indudeFHto Y axis, facial axis, 3 and posterior / anterior face heightratio. 17 Clinical proceduresthat openthe bite and result inincreased vertical dimension should be avoided in casesalready displaying excessive lower face height.Skeletal effects of protraction headgearThe most important growth sites in the development ofthe nasomaxillary complex are the circummaxillary sutures.iS,19 These include the lary,and thepterygopalatine sutures. These sutures are situated parallel to each other and are oriented so they project downward. Growthat these sutures has the effect of shifting themaxillary complex downwardand forward (Fig 4).Animaland skull studies a , al using maxillary protraction devices showsignificant anterior displacement of themaxillary complexand significant changes in the circummaxillary sutures and maxillary tuberosity. Tension producedwithin the sutures causes an increase in vascularityand a concomitant differentiation of the cellular tissueresulting in increased osteoblastic activity. While recognizing the limitations of skull studies, it is reasonable toconclude that maxillary protraction appliances have theirprimary skeletal effect at the midfacial sutural growthsites.During the use of conventional maxillary protractionappliances, clinicians have observed extrusion and anterior rotation of anchor teeth, downwardmovementof themaxilla, anterior movementof the maxilla, anterior (counterclockwise) rotation of the maxilla, and a constriction ofthe anterior region of the maxilla. 2 24 Anterior maxillaryrotation is the result of downwardmovementof the posterior nasal spine. The center of resistance of the maxillarycomplex has been estimated to be positioned between themaxillary first and second premolar sagitally, and between the lower margin of the orbit and the distal apex of the maxillary permanentfirst molar vertically.Conventional protraction headgear devices use elasticsstretched between some point of attachment on the maxillary teeth and the headgear. For patient comfort theelastics must comeout of the mouthwithout distorting thelips, whichlimits the clinicians’ control of the direction offorce application. Becausethe elastics’ protraction force isapplied at a distance below the center of resistance, themaxillary complex is subjected to a forward and downward force as well as a counterclockwiserotational force.(Fig 5) Other changes that have been observed with conventional protraction headgear include a posterior (dockwise) rotation of the mandible, increased anterior faceheight and increased facial convexity.27 Most of the mandibular changes can be attributed to increased downwardgrowth of the maxilla. The protraction headgear does,however,transfer part of the reciprocal force to the mandible, and it has been shownthat stress trajectories doconcentrate along the ramus and condylar neck of themandible,as Other less widely used protraction headgearhave been designed to overcomethis problem by using acomplex facebow attachment mechanism,as, asClinical studies indicate that the maxilla can be advanced 2-4 mmover a 12- to 15-monthperiod of treatmentwith a protraction headgear worn 14 hr per day. 24,27 Theamount of anterior maxillary movement is larger inyounger patients (under 9 years of age).24 Althoughlongterm follow-upstudies are not available, it is reasonabletoassume the maxillary changes are relatively stable. Thelong-term stability of midpalatal suture expansion is welldocumentedand the histologic effect on the circum-maxillary sutures with protraction headgear is very similar.Whenrelapse is observed it is likely due to an increase ina7mandibular protrusion,Clinical apj}lications and treatmentconsiderationscaseselectionPatients selected for protraction headgear treatmentshould have a retrusive maxilla with a normal or mildlyprotrusive mandible and inadequate or normal maxillaryvertical development. Cases presenting with excessiveincisor display, anterior openbite, or excessive lower faceheight should not be treated with protraction headgear.Palatal expansionVery often patients presenting with Class I skeletalmalocclusions have bilateral posterior crossbites due todeficient transverse maxillary growth combined with theabnormal sagittal relationship of the maxilla and mandible. Maxillary expansionprior to protraction, as well asaddressing the transverse discrepancy, has the added ben29 and perhaps forward moveefit of initiating downwardPediatricDentistry:May/June, 1993 - Volume 15, Number 3 205
mentof the maxilla. B Palatal expansion affects not only the intermaxillary suture system, but the entire circum-maxillary suturesystem.31 Palatal expansioninitiates cellularresponse in the sutures, allowing a morepositive reaction to protraction force.Palatal expansion should be started witha fixed rapid palatal expansion appliance(hyrax) at least 7-10 days prior to initiatingprotraction force. The hyrax expansion appliance should be activated by turning thejack screw1 / 4 turn daily, resulting in 1 -rampalatal width increase every four days .3o Thelength of preprotraction expansion will depend on the severity of the posterior transverse discrepancy.A .045" wire is soldered to the buccal aspect of the hyrax expansion appliance. Thewires should extend forward into the cuspid region and be bent into a hookto attachthe extraoral elastics to the protraction headgear (Fig 6).(a)Fig7. Protractionheadgear.to monitor pro-gress. The overjet should be overcorrected andthe protraction headgear continued at nights for 4 to 6 monthsdepending on the patient’s tendency to relapse. Full bandedorthodontic therapy will be required following Phase I orthopedic correction. The protractionHeadgearadjustment(b)headgear may be necessary durThe headgear pads should be adjusted toFig 6. Modifiedhyrax expansioning Phase II to help control discomfortably contact the forehead and chin,proportionate growth betweenand the elastics should be directed with a appliance.the maxilla and mandible durslightly downwardforce (Fig 7). The direcingtheprepubertalgrowthspurt.tion of the elastic force can be modifiedslightly dependingon the degree of anterior maxillary rotation versus bitePatient motivationopening that is desired. Morehorizontally directed forcePatient complianceis critical to successful treatment.will reduce the amount of bite opening but increase thePositive reinforcement using a series of short- and longrotational effect (Fig 5). Excessivepressure from the superterm goals is vital. Praise and rewards are most effectiveior edge of the chin cup maycause labial gingival receswhen developed together with the patient, and awardedsion.upon the attainment of each goal. Contacting the child’sApplication of force should begin with light elasticsteacher to explain the nature of the problemand the objec(100-150grn per side) until the patient has adapted to the32tives of the protraction headgear appliance is helpful.appliance, then the force should be increased to 300-500 The teacher can then explain the situation to the child’sgrn per side. The elastics should be replaced daily.class, helping to eliminate negative peer pressure at school.TreatmenttimingConclusionProtraction headgear has been shownto be most effective in the full primaryor early transitional dentition, withProtraction headgearis a very useful and effective meansconsiderablyless skeletal changeafter 9 years of age.2 It isof treating youngpatients presenting with a Class HI skelalso important to initiate treatment early enoughso thatetal pattern. Patients should exhibit a retrusive maxillaadequate root structure is still present on the primaryfirstand should not exhibit excessive vertical development ormolars to anchor the expansion appliance.anterior open bite. Assumingthese diagnostic criteria areDependingon the severity of the problem and the agecarefully observed, this treatment technique will produceof the patient, wearing the appliance 24 hr/day will usuconsistent results. The appliance mechanicsare relativelyally correct the problem within 4 to 8 months. The samesimple and can be managedeffectively by pediatric denresult can be achieved with 14-hr/day wear over a periodfists experienced in orthodontic diagnostic procedures.of 12 to 16 months.This treatment approach should be considered and, whenappropriate, offered to the patient and parents.PatientrecallThe patient should be seen approximately one weekDr. Major is an associate professor and chairman of the Division ofafter appliance insertion to evaluate patient compliance Orthodontics, Faculty of Dentistry, University of Alberta. Dr.and to ensure that the appliance is properly adjusted. TheE1Badrawyis a professor and chairman of the Division of Pediatricpatient can be evaluated at regular 4- to 6-weekintervalsDentistry, Faculty of Dentistry, University of Alberta.206 Pediatric Dentistry: May/June,1993 - Volume15, Number3
1. Harle GD:The prevalence of malocclusion in grade eight childrenin Edmonton. MScThesis, 1976.2. Ishii H, Morita S, Takeuchi Y, NakamuraS: Treatment effect ofcombined maxillary protraction and chincap appliance in severeskeletal Class III cases. AmJ Orthod Dentofacial Orthop 92:30412, 1987.3. Mitani H, FukazawaH: Effects of chincap force on the timing andamount of mandibular growth associated with anterior reversedocclusion (Class III malocclusion) during puberty. AmJ OrthodDentofacial Orthop 90:454-63, 1986.4. Ritucci R, NandaR: The effect of chin cup therapy on the growthand development of the cranial base and midface. AmJ OrthodDentofacial Orthop 90:475-83, 1986.5. Sugawara J, Asano T, Endo N, Mitina H: Long-term effects ofchincap therapy on skeletal profile in mandibular prognathism.AmJ Orthod Dentofacial Orthop 98:127-33, 1990.6. Wyatt WE: Preventing adverse effects on the temporomandibular joint through orthodontic treatment. AmJ Orthod DentofacialOrthop 91:493-99, 1987.7. Ellis E III, McNamaraJA Jr: Componentsof adult Class III malocclusion. J Oral Maxillofac Surg 42:295-305, 1984.8. Guyer EC, Ellis E IIL McNamaraJA Jr, Behrents RG: Componentsof Class III malocclusion in juveniles and adolescents. AngleOrthod 56:7-30, 1986.9. Sue GI, Chaconas SJ, Turley PK, Itoh JK: Indicators of skeletalClass III growth. J Dent Res 66:348, (Abstr 1932) 1987.10. :25863, 1979.11. Jacobson A: The "Wits" appraisal of jaw disharmony. AmJOrthod 67:125-38, 1975.12. McNamaraJA Jr: A method of cephalometric evaluation. AmJOrthod 86:449-69, 1984.13. Ricketts RM: Perspectivesin the clinicalapplication ofcephalometrics: the first fifty years. AngleOrthod 51:11 5-50,1981.14. Powell N, HumphreysB: Proportions of the Aesthetic Face. NewYork: Thieme-Stratton Inc, 1984.15. NandaSK: Patterns of vertical growth in the face. AmJ OrthodDentofacial Orthop 93:103-16, 1988.16. Solow B, Houston WJB:Mandibular rotations: concepts and terminology. Eur J Orthod 10:177-79, 1988.17. Siriwat PP, Jarabak JR: Malocclusion and facial morphology. re a relationship? An epidemiologic study. Angle Orthod55:127-38, 1985.Ranly DM:A synopsis of Craniofacial Growth: 2nd ED, Norwalk,CT: Appleton & Lange, 1988.Enlow DH: Handbook of Facial Growth. 2nd ED. Philadelphia:WBSaunders Co, 1982.Hata S, Itoh T, Nakagawa M, Kamogashira K, Ichikawa K,Matsumoto M, Chaconas S: Biomechanical effects of maxillaryprotraction on the craniofacial complex. AmJ Orthod DentofacialOrthop 91:305-11, 1987.Tanne K, Sakuda M: Biomechanical and clinical changes of thecraniofacial complex from orthopedic maxillary protraction. AngleOrthod 61:145-52, 1991.MermigosJ, Full CA, Andreasen G: Protraction of the maxillofacial complex. AmJ Orthod Dentofacial Orthop 98:47-55, 1990.Cozzani G: Extraoral traction and Class III treatment. AmJ Orthod80:638-50, 1981.SakamotoT: Effective timing for the application of orthopedicforce in the skeletal Class III malocclusion. AmJ Orthod 80:41116, 1981.Nanda R: Biomechanical and clinical considerations of a modified protraction headgear. AmJ Orthod 78: 125-39, 1980.Staggers JA, GermaneN, Legan HL:Clinical considerations in theuse of protraction headgear. J Clin Orthod 26:87-91, 1992.Wisth PJ, Tritrapunt A, Rygh P, B e OE, Norderval K: The effectof maxillary protraction on front occlusion and facial morphology. Acta Odontol Scand 45:227-37.de Alba y Levy JA, Caputo AA, Chaconas SJ: Effects of
Pediatric Dentistry: May/June, 1993 - Volume 15, Number 3 203 % Cauc Caucasian . Because the treatment objective is to optimize fadal esthetics, treatment decisions should be based more on the patient’