Transcription
A CLINICAL OVERVIEW1Sympatheticnervous systemand pain21
TOPICAL ISSUES IN PAIN 322
A CLINICAL OVERVIEW1A clinical overview of theautonomic nervous system,the supply to the gut andmind–body pathwaysLOUIS GIFFORD AND MICK THACKERIntroductionThe autonomic nervous system (ANS) is an ‘output’, ‘effector’ or ‘motor’system (see Gifford 1998b)—i.e. it responds to the demands of the sensorysystems and the central nervous system (CNS) by producing an effect on thetissues it supplies. There are no sympathetic or parasympathetic sensory(afferent) fibres as such, although a great many visceral sensory fibres dotravel in nerves like the vagus and splanchnic, which are commonly describedin parasympathetic and sympathetic sections of anatomy texts and oftenreferred to as ‘sympathetic afferents’ (see discussion of visceral afferentsbelow).Since the ANS is an output system, its role in pain states has to besecondary to its effects on sensory systems (see following chapters).ANS fibres create their ‘effects’ via electrochemical stimulation of smoothmuscles or glands. Their secretions also produce direct chemical effects onthe tissues they innervate and thus change their chemical characteristics.Any chemical or physiological tissue changes may in turn be fed back to theCNS via stimulation of sensory afferent pathways. This is important becauseANS activity has been implicated not only in producing and modulatingnociception and pain, but also as playing a role in the expression andconscious awareness of emotions (see Meyers 1986). Recent studies show,for example, that different emotions (anger, fear, disgust, sadness, happiness,surprise) can be distinguished to some extent on the basis of differentautonomic nervous system responses (like skin temperature and heart rate)(LeDoux 1998, p 292). We all know that strong emotions are expressed as23
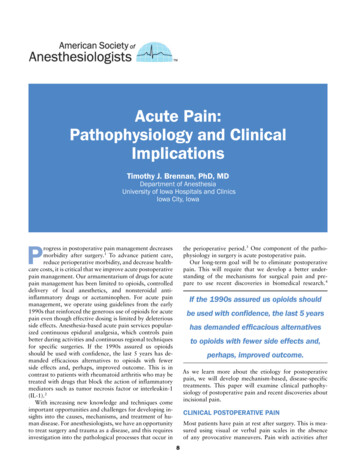
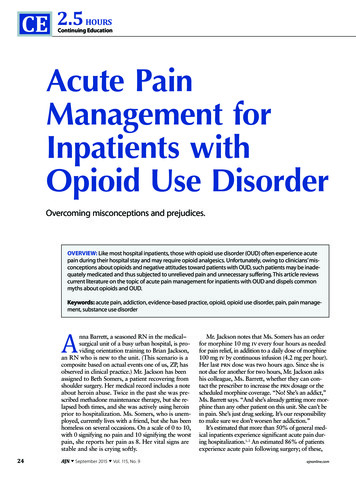
TOPICAL ISSUES IN PAIN 3bodily sensations and that ‘gut feelings’ play crucial roles in our emotionalexperiences and can have a strong impact on our decision making processes(Damasio 1995, LeDoux 1998, Damasio 2000).In their detailed overview of the ANS, Janig and Habler (1999) go out oftheir way to debunk the traditional descriptions of the ANS and the viewthat it is ‘all or nothing’ and general in its mode of action. In parallel with theneuroendocrine system, the ANS regulates target organs in order to maintainthe homeostasis of the body. Simply, it adapts, adjusts and co-ordinatesappropriate systems so as to produce the required physiological conditionsfor life, which includes, any required physical activity. In this way it isinvolved in producing and co-ordinating the necessary physiologicalresponses for activities like moving, resting, sleeping, feeding and digestion,sex, pregnancy and nurturing, growth and repair and all extreme responsesrelating to threatening and stressful situations. This includes responding totissue injury and to emsystemExternalworldFig. 1.1 A modified version of Janig and Habler’s model of the integration andrelationships of the brain and body. What it so nicely illustrates are the forward andback communication links between all levels of the nervous system, the body, and theenvironment. Communication is via neuronal, hormonal and humoral pathways.Adapted from: Janig W, Habler HJ 1999 Organization of the autonomic nervous system: structureand function. In: Appenzeller O (ed) Handbook of Clinical Neurology Vol 74 (30): The AutonomicNervous System Part 1: Normal Functions. Elsevier, Amsterdam24
A CLINICAL OVERVIEWANS activities can be viewed as being governed by the commands it receivesfrom the modules of the CNS that ‘scrutinise and appraise’ the sensory andincoming information received (Gifford 1998). Thus, environmental inputsfrom sense organs, electrochemical sensory inputs from body tissues andorgans, inputs derived from the immune system and inputs that derive fromthe thinking, analysing and planning centres of the brain, all serve to createspecific ANS driving stimuli. Thus, at least in part, the ANS is subservient tothe wishes and desires created in our mind. If you want to get up out of thechair and go for a walk—the ANS has to organise the physiological backupand supply networks that support the action demanded.Figure 1.1, taken from Janig and Habler (1999) and modified slightly,usefully illustrates where the ANS occupancy of the nervous/homeostaticsystems sits. The model, which is quite like the Mature Organism Model(Gifford 1998) in that it is ‘circular’—having input, processing and outputelements—nicely illustrates the integration of all elements of the bodyincluding the brain and its higher centres.The following example may help you/the reader appreciate the role ofthe ANS and the importance of models like these to clinical reasoning.In creation of hunger, ‘body organs’ relay information to the CNS aboutthe levels of glucose in the blood. Information may be via neural or humoral/endocrine systems and messengers. From the neural pathway perspective,it is known that special chemoreceptive sensory nerve fibre endings thatrespond to blood glucose levels exist in the pancreas and gastrointestinaltract as well as in the blood vessels of the third ventricle of the brain adjacentto the hypothalamus. The ‘sampled’ information is then relayed to specificregions of the CNS that scrutinise and deal with ‘actions’ relating to hungerand energy supply. The message is simply—‘energy levels low, pleaserestore.’ The CNS regions involved in scrutinising and mounting a coordinated response are thought to reside in the hypothalamus, in particular,the paraventricular and ventromedial nuclei and the lateral hypothalamicareas (Westmoreland et al 1994). ‘Output’ from these areas may be directedto the limbic and neocortical areas, creating the sensation of hunger, whichin turn drives food gathering behaviour via the musculoskeletal system andthence to the ‘external world’ as noted in Figure 1.1.At the same time: Autonomic output activates relevant regions of the alimentary tract inorder to make ready for food intake and digestion. Autonomic activity will also stimulate the pancreas and adrenal glands,both of which are important in the hormonal regulation of glucose andenergy metabolism. Autonomic activity will co-ordinate the cardiovascular system so that bloodsupply demands may be met from the musculoskeletal system whoseactivities are needed to gather food, prepare, eat, and metabolise it.As the process of food gathering and feeding proceed so the input,scrutinising, and output systems change their activities in response to thechanging situations.25
TOPICAL ISSUES IN PAIN 3It is often said that the sympathetic system ‘kicks into action duringemergencies’. Robert Salposky (1994) adds the (clinically) important caveat‘or what you think are emergencies’—that underlines the importance ofpersonal assessment of the situation we find ourselves in. Thus, how thesympathetic system responds is very much influenced by the emotional,cognitive and conscious brain—‘our’ interpretation of the situation we are inis hugely responsible for its activities. If you believe the pain you have signifiesa serious illness or condition you will have a far different ‘sympathetic’ reactionthan if you dismiss the pain and pass it off as trivial. If as a patient you thinkthat what the therapist is doing to you makes sense and feels right you willhave quite a different response from someone who might be feeling unsure oreven slightly anxious about what is being done to them (see also Chapter 4). Itis probable that a clinician’s most powerful effect on a patient’s sympatheticsystem activity is produced via the atmosphere of the therapeutic interaction.Importantly, this relates more to what the patient actually feels and interprets,than to what the clinician thinks they should feel or should have interpreted.The effect of a productive ‘therapeutic alliance’ on the activities of systemslike the ANS should never be underestimated (see the Placebo section in TopicalIssues in Pain 4.)Autonomic anatomy—from spinal cord outAs discussed, the sympathetic and parasympathetic systems are efferent—just like the somatic motor system they have an ‘effect’ on the tissues thatthey innervate. Simply, impulses radiate from the central nervous system totarget tissues in the body. While activity in somatic motor efferent neuronescause striated muscles to contract, those in the autonomic nervous systemhave a wide range of targets and effects. For example, via the sympatheticinnervation of smooth muscles in blood vessel walls sympathetic activitycan alter vessel lumen size and hence alter blood flow; it can cause secretoryglands to be activated or inactivated; and, via secretion of chemicals fromvesicles in its terminals, it can influence the chemical environment, the healthand the healing of the tissues innervated (see Chapters 2 and 3). As well ashaving the capacity to have quite massive effects, it also seems that theautonomic nervous system is capable of acting in a highly specific andlocalised way.The sympathetic systemThis section is intended to provide the reader with an overview of a poorlyunderstood system. Review of classic anatomical texts and overviews bycurrent leaders in the field of autonomic nervous system anatomy, physiologyand function reveals quite marked discrepancies and inconsistencies. Thereader would be well advised to read some of the papers and texts cited atthe end of this chapter for fuller accounts.26
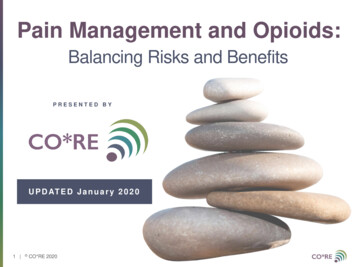
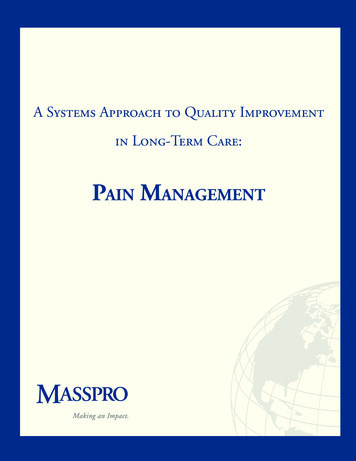
A CLINICAL OVERVIEWFig. 1.2The thoracic paravertebral sympathetic chain and its relationshipsAdapted from: Harati Y, Machkhas H 1997 Spinal cord and peripheral nervous system. In: Low PA(ed) Clinical Autonomic Disorders 2nd edn. Lippincott-Raven, PhiladelphiaThe best known parts of the sympathetic system are the two sympatheticchains or trunks that extend from the base of the skull to the coccyx. Thesetwo ‘paravertebral’ sympathetic chains lie on either side of the vertebralcolumn (Figs 1.2, 1.3, 1.4 & 1.5) but may come together and fuse in the sacralregion to form the ganglion ‘impar’. Each chain has about 22 or 23paravertebral ganglia which contain nerve axons and the cell bodies ofpostganglionic neurones. A ganglion is a swelling of a nerve due to the largenumbers of cell bodies it contains. Sympathetic ganglia can be thought of ascommunication boxes or relay stations where information in the form ofimpulses may be modulated and passed on, even prevented from passing27
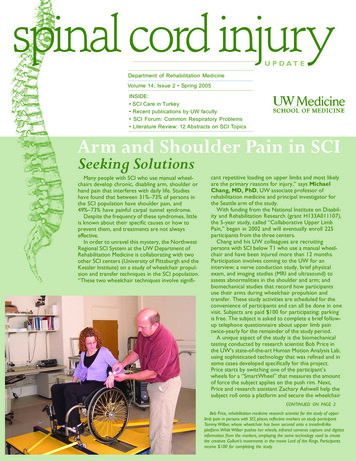
TOPICAL ISSUES IN PAIN 3Fig. 1.3 The organisation, layout, relations and basic supply of the peripheralsympathetic system. Dashed lines represent preganglionic fibres, continuous linesrepresent postganglionic fibres.Adapted from: Harati Y, Machkhas H 1997 Spinal cord and peripheral nervous system. In: Low PA(ed) Clinical Autonomic Disorders 2nd edn. Lippincott-Raven, Philadelphia28
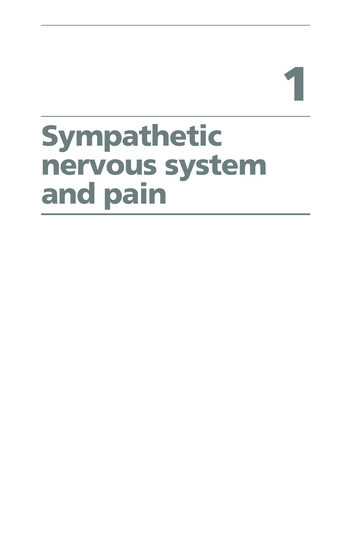
A CLINICAL OVERVIEWFig. 1.4 The origin and course of the sympathetic fibres to the arm. The diagram alsoshows the cervical sympathetic chain, roots and brachial plexus relationships. Thepreganglionic fibres from T2 and T7 are dotted because their supply to the upper limbis uncertain. The preganglionic fibres from T1 and T8 are dashed to show they arepresent but not involved in the upper limb sympathetic supply. The cervical roots haveno preganglionic fibres and the spinal nerves of the plexus that derive from these rootsonly have grey rami communicantes. SCG: superior cervical ganglion; MG middle cervicalganglion; SG stellate ganglion.Adapted from Grieve GP 1994 The autonomic nervous system in vertebral pain syndromes, Fig.20.4. In: Boyling JD, Palastanga N (eds) Grieve’s Modern Manual Therapy 2nd edn. ChurchillLivingstone, Edinburgh29
TOPICAL ISSUES IN PAIN 3Fig. 1.5 The sympathetic supply to the lower limbs following the principle of Fig. 1.4.The parasympathetic supply is also illustrated.Adapted from Grieve GP 1994 The autonomic nervous system in vertebral pain syndromes, Fig.20.5. In: Boyling JD, Palastanga N (eds) Grieve’s Modern Manual Therapy 2nd edn. ChurchillLivingstone, Edinburghon, or simply allowed to pass straight through unchecked. Many of theparavertebral ganglia relate to the cord segment from which they derive(Fig. 1.3). However, there are fewer in number than there are segments inthe spine as some of the ganglia are fused. In the cervical region there arenormally three ganglia—the most rostral being the superior cervical ganglion,below this is the middle cervical, and lowest of all, the stellate ganglia (Figs1.3, 1.4). The stellate ganglion consists of the fused inferior cervical ganglion30
A CLINICAL OVERVIEWwith the first thoracic ganglion. There are usually four ganglia in the lumbarpart of the chain and four or five in the sacral region.The spinal cord only connects to the sympathetic chain via the 14 spinalnerves that exit from the intervertebral foramen between T1 and L3 (i.e. viaroots T1–L2) (Figs 1.3, 1.4, 1.5). Hence its ‘outflow’ is said to be ‘thoracolumbar’. This means that all the peripheral sympathetic nerve pathways tothe target tissues and organs of the body have their origins in the spinal cordsegments of T1 to L3 (but see Grieve 1994, p 297).Although it has segmental origins, the SNS, to quite a marked extent,actually defies the traditional description of a segmental system (see below).Thus, sympathetic supply to the head and neck has its origins from the nerveroots of T1–T5 (mostly upper 2 or 3); the upper limb from roots T2–T6 (butpossibly as far as T7 or T8) (Fig. 1.4); the thorax from roots T3–T6; the abdomenfrom roots T7–T11 and the lower limbs from roots T10–L2 or L3 (Fig. 1.5).This supply may be an important consideration when investigating theconsequences of thoracic and high lumbar nerve trunk and nerve root injuriesor irritations. What can be applauded is the neat fact that these vital controlsupply lines exit and have their origins from parts of the spinal column thatare relatively rarely injured and well protected.The sympathetic supply involves a two neurone pathway from the spinalcord to the target tissues of the periphery (Fig. 1.6). These neurones are termedpreganglionic and postganglionic respectively.There is some evidence that the sympathetic ganglia contain interneurones, termed ‘SIF’ (small intensely fluorescent) cells that may servemodulatory functions, i.e. they aid in the integration or processing ofincoming and outgoing information (see Grieve 1994, p 299).The preganglionic neurones of the sympathetic system have their cellbodies in the lateral grey horn (Fig. 1.7), (also known as the intermediatezone, or interomediolateral cell column) of the spinal cord. As already noted,the cell bodies of these neurones are only found in segments T1 to L3(Westmoreland et al 1994) of the spinal cord. Its segmental origins are worthnoting since the sympathetic system innervates just about every tissue ofthe body via these spinal segments.Myelinated preganglionic fibres pass away from the spinal cord via theventral root and into the spinal nerve for a short distance, then via the whiterami communicantes they join the sympathetic trunk.Having reached the sympathetic trunk, the preganglionic sympatheticfibres may do several things (see Fig. 1.7). Some synapse with postganglioniccells in the paravertebral ganglion that lies at the same level from which theyexit the vertebral column (nos 1, 3 & 4 in Fig. 1.7). Others pass through theirsegmental ganglion and run up or down to more distant paravertebral gangliawhere they terminate and synapse with postganglionic fibres (no. 5 in Fig.1.7). Note how this defies the idea of ‘segmentalism’. It is commonly statedthat there is a pre to postganglionic neurone divergence ratio of anythingfrom 1:1 to 1:196 (see Grieve 1994, Williams et al 1995). In other words onepreganglionic fibre may terminate with only one postganglionic fibre, ormay have a massive terminal aborisation connecting to a great many. The31
TOPICAL ISSUES IN PAIN 3Fig. 1.6 The basic arrangement of the peripheral components of the sympatheticand parasympathetic systems. Note the long to short relationship of the pre to postganglionic sympathetic fibres and the opposite for the parasympathetic fibres. Cranialoutflow of the parasympathetic system not illustrated here. Classic neurotransmittersand receptor types for each system are illustrated: A-r adrenoreceptor; mr muscarinicreceptor; n nicotinic receptor; N-a noradrenaline/norepinephrine; Ach acetylcholine.reality is that there is anatomical convergence (many preganglionic fibres goingto one postganglionic fibre), as well as anatomical divergence (the opposite).Importantly, anatomical convergence/divergence does not mean that all theconnections are necessarily always functional. Just as elsewhere in thenervous system, there is a huge potential for a spread of effect or a focus ofeffect that is dependent on continuously fluctuating inhibitory and excitatorymodulatory controls. This attribute allows for both expansion and exquisiterefinement of autonomic outputs and argues against the blind acceptance ofthe generalised fight and flight-related function of this system. The possiblemodulatory role of ganglionic inter-neurones as well as branches fromreturning visceral sensory afferents (see below) may be important here.What we do know is that the SNS tends to be a functionally ‘divergent’system—where small numbers of preganglionic fibres have the potential toinfluence larger numbers of postganglionic fibres—hence the potential for asingle ‘action’ message producing far reaching effects on target organs and32
A CLINICAL OVERVIEWFig. 1.7 Diagrammatic representation of the various ‘pathways’ the sympatheticsystem can take from the thoracic cord to the periphery. Refer to text for details of nos1–5.Adapted from: Harati Y, Machkhas H 1997 Spinal cord and peripheral nervous system. In: Low PA(ed) Clinical Autonomic Disorders 2nd edn. Lippincott-Raven, Philadelphiatissues. The fact that there may be provision for control of this divergencehelps explain a degree of specificity, too.In a similar way to that described in the CNS, the potential for excessivereactivity and spread of effect due to maladaptively altered modulatorycontrols, or even loss of control, having far reaching effects on sympatheticactivity seems a reasonable possibility. Clinically this may provide a possibleexplanation for reports of localised patches of skin colour change, or localisedsweating or swelling disturbances that spread to larger areas over time.Many preganglionic fibres pass right through the sympathetic chain andparavertebral ganglia without synapsing on postganglionic fibre cells at all(no. 2 in Fig. 1.7). These continue out of the sympathetic chains in thesplanchnic nerves to reach remote ganglia situated nearer their target organs.These more distant ganglia are often called ‘prevertebral’ ganglia (Figs 1.3,1.7). Well known prevertebral ganglia supplied via the thoracic splanchnicnerves are the celiac, superior and inferior mesenteric ganglia. These ganglia33
TOPICAL ISSUES IN PAIN 3are situated in the abdomen anterior to the abdominal aorta close to the originof the celiac and mesenteric arteries. Via postganglionic fibres they form theceliac plexus that innervates abdominal, pelvic and perineal organs. Whilethe thoracic splanchnic nerves derive from branches arising from the lowereight thoracic paravertebral ganglia, the lumbar splanchnic nerves derive frombranches arising from the upper three lumbar paravertebral ganglia.One special group of preganglionic neurones pass directly to their targettissue (see Fig. 1.3). These innervate the adrenal medulla, seemingly omittingthe ‘postganglionic’ component of the pathway. In fact, the adrenal medullaresembles nervous tissue more than it does a typical endocrine gland. Its cellsbehave lik
Jun 01, 2013 · chair and go for a walk—the ANS has to organise the physiological backup and supply networks that support the action demanded. Figure 1.1, taken from Janig and Habler (1999) and modified slightly, . order to make ready for food intake and digestion. . no preganglionic fibres and the spinal nerves of the