Transcription
Copyright EMAP Publishing 2015This article is not for distributionNursing PracticeReviewPain managementKeywords: Adult/Assessment/Pain Thisarticle has been double-blindpeer reviewedPain is a personal experience but may be difficult to communicate. It is vital thatnurses know how best to assess it to ensure the optimal treatment is givenpart 3 of 3: pain managementThe importance ofassessing pain in adultsIn this article. ore elements of a pain assessmentC Tools to help patients self-report pain Common sites of referred painAuthor Amelia Swift is senior lecturer innursing at the University of Birmingham.Abstract Swift A (2015) Pain management3: The assessment of pain in adults.Nursing Times; 111: 41, 12-17.Pain affects patients physically andemotionally, so successfully managing thepain they experience is a key componentof their recovery. This third article in aseries on pain looks at why it is importantto assess pain in adults and how this canbest be done. The causes and symptomsof chronic and acute pain are detailed,along with the different assessment toolsthat can be used and for which patientsthey are suitable.AlamyPain is a personal experience, andevery experience of it is unique.It is not just a physical sensationbut is bound up with an emotional response and an act of reasoning;this is why pain is known as a multidimensional experience (Fillingim et al, 2014).Pain also has physical and emotional consequences; it can make us lead to fatigue,irritability, depression or inability to carryout activities of daily living (Leadley et al,2014). Chronic pain also affects social andeconomic wellbeing, restricting work andsocial activities (Morgan et al, 2011).Pain is difficult to explain and use ofanalogies is common (Schott, 2004). Forexample, “It feels like my head is in a vice”immediately communicates what thepatient is feeling, while “This pain iskilling me” demonstrates the psychological impact of pain. Patients need to communicate pain because they want others toknow how they feel because that iscomforting and elicits empathy and help(Buenaver et al, 2007). Health professionalswant to understand patients’ pain becausethat will help them to diagnose theproblem, select an effective treatment programme and monitor their progress.Purpose of pain assessmentA pain assessment is conducted to:» Detect and describe pain to help in thediagnostic process;» Understand the cause of the pain tohelp determine the best treatment;» Monitor the pain to determinewhether the underlying disease ordisorder is improving or deteriorating,and whether the pain treatment isworking.The content and scope of the assessment depends on its purpose and the typeof pain. Acute pain is caused by a shortlived pathological process, such as a surgical incision or a sprain. Provided thispain is treated and there is no nervedamage, it usually resolves as the bodyheals (Grichnik and Ferrante, 1991).Chronic pain lasts for a prolonged time –at least three months (this is the time atwhich tissue healing should be complete)(Hughes, 2008). The term describes complex pains where there may have been apathological trigger but, although healinghas taken place, the pain continues – forexample, chronic low back pain. Anothertype of chronic pain relates to ongoingpathological processes, such as osteoarthritis, and to pains that are caused bydamage to, or dysfunction of, the nervoussystem; this includes pains as diverse aspost-stroke pain and diabetic neuropathy.12 Nursing Times 07.10.15 / Vol 111 No 41 / www.nursingtimes.net5 keypoints12Pain can beacute or chronicin naturePainassessmentsare crucial toascertain the besttreatment andmonitor anyunderlying causalconditionPatients maynot alwaysvolunteerinformation aboutthe pain they areexperiencing somay need to beasked about itVarious painassessmenttools exist to caterfor patients’differentcapabilitiesPain severityshould bedocumented totrack efficacy oftreatments andinterventions andpatient recovery345Phrases like “my head feels like it’s in a vice”can help nurses get a sense of pain severity
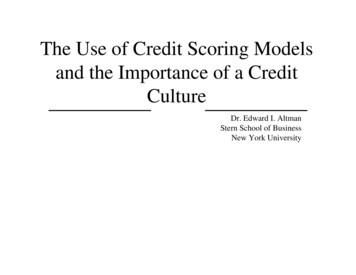
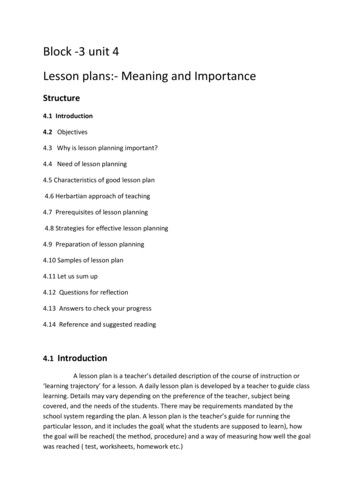
Copyright EMAP Publishing 2015This article is not for distributionNursingTimes.netBox 1. signs of painBehavioural signs Verbalisation (crying out, crying,sobbing) Agitation, restlessness Abnormal stillness, rocking, writhing Facial expression (tense, grimace,distorted) Position (guarding, curled, holdingtightly)Physiological signs Increased respiratory rate Increased heart rate Increased blood pressure Pallor Sweating Nausea VomitingInitial assessments will cover a lot ofground because they are used as part of amuch wider exercise designed to helphealth professionals understand whypatients are seeking treatment, whattreatment and interventions have beentried, and their understanding of theircurrent situation. Pain assessments afterthis point may focus on a smaller rangeof the pain experience to monitortreatment, the patient’s recovery or thecourse of the disease.Up to 20% of the European populationexperiences chronic pain (van Hecke et al,2013) and so it is likely that patients in theacute-pain setting may have both acutepain and chronic pain.Patient participationPatients vary in their ability to lead or participate in discussions about their painand it is important for nurses to considerthis before choosing the most appropriateassessment strategy. Self-report of painusing a guided question set is the best wayto assess pain (MacIntyre and Schug, 2014).When patients cannot verbally reportpain, there are a range of other options,including pain rating scales, to which thepatient can point if able to do so. TheWong-Baker FACES Pain Scale has beenendorsed by many groups as an effectivetool for use in people with mild-to-moderate cognitive impairment (Scherder et al,2009), even though it is better known as atool used with children.Some tools, such as the COMFORT scale(Bit.ly/COMFORTScale; Van Dijk et al, 2000),focus on behavioural signs of pain (Box 1),which may also include physiologicalchanges. When a person with dementia isFor more articles on pain management, goto nursingtimes.net/painfig 1. Cues used to prompt pain assessmentprocessesS SiteO OnsetProvoking or palliating factors PC CharacterQuality QR RadiationRadiation RSeverity STime TA AssociationsT Time courseE Exacerbating and relievingfactorsS Severityunable to participate in the assessmentprocess, it is recommended that a toolspecifically designed to assess pain in nonverbal older adults is used: a comprehensivereview of 17 of these can be found on theCity of Hope Pain and Palliative CareResource Center’s website (Bit.ly/PainNOA).Health professionals should not assumethat a patient cannot participate in a painassessment. People with dementia canoften use self-report pain scales but theymay need to be re-taught how to do so eachtime (Kaasalainen et al, 2013). Almostuniversally, patients change their “normal”behaviour when they are in pain, soknowing individual patients and theirnormal demeanour is vital.Common elements of theassessmentCore information is common to all painassessments. Mnemonics or initials can behelpful cues for remembering the contentsof the essential baseline information. Twoof the most popular cues are PQRST andSOCRATES (Fig 1).The emphasis placed on the differentcomponents of the assessment depends onthe context in which it takes place. As anexample, people with chronic pain canexperience long-term mood changes(Eccleston et al, 2013) and so the emotionalimpact of pain forms a major part of thetreatment plan – often more attention ispaid to these emotional components inchronic pain than in acute pain.Onset of painPain is often associated with an injury ordisease process but can also emerge slowly,usually in relation to a progressive diseaseor disorder, such as osteoarthritis ordegenerative nerve disorders. With somekinds of chronic pain, patients may not beable to identify an event that triggered itand the lack of an identifiable and treatablepathology can be worrying to them.Questions about onset of pain revealwhat patients know or believe about whatis happening to them. Their understandingcan have a significant influence on theirability to cope, follow instructions andrespond to treatment. Taking chest painas an example, many people associatethis with myocardial infarction andthere is evidence that, even when MI isruled out, patients still experience fear,stress and a sense of loss of strength(Jerlock et al, 2005).The cause of painIn order to select the most appropriatetreatment is necessary to identify themechanism of injury (how it happened).Some key questions include:» Is this pain related to tissue damage? Thistype of pain is called nociceptive pain,physiological pain, inflammatory painand tissue damage pain. It can becaused by direct trauma to the tissues(for example, burn, surgery, graze,sprain) or ongoing disease process(such as arthritis). It can be superficial(related to the skin and muscle), whichis called somatic pain, or deep andrelated to the organs (for example,bowel, pancreas, heart), which is calledvisceral pain.» I s this pain related to nerve damage or adisorder of the nerves or nervous system?This sort of pain is called neurogenicpain, neuropathic pain, central painand phantom pain. It can be causedby direct trauma to the nerves due tocompression, cutting or chemicalinsult; malfunction or disease-relateddamage of the nerves (such as diabeticneuropathy, alcoholic neuropathywww.nursingtimes.net / Vol 111 No 41 / Nursing Times 07.10.15 13
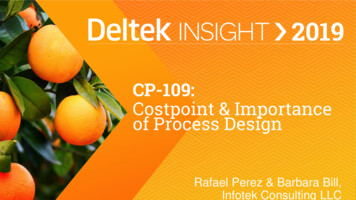
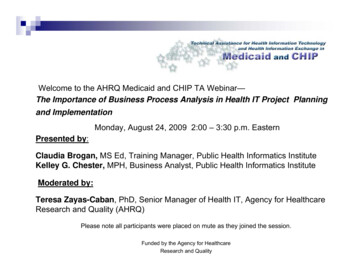
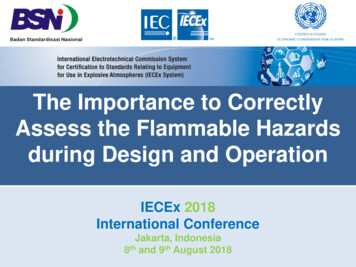
Copyright EMAP Publishing 2015This article is not for distributionNursing PracticeReviewBox 2. descriptorsfor painNociceptive wordsSomatic (cutaneous) Aching Stabbing Squeezing Throbbing Sharp Tender Dull HeavyVisceral (organs) Cramping Gnawing Aching Pressing PullingSources: Wylde et al, 2011; Dobratz, 2008)Neuropathic words (Lin et al, 2011) Burning Tingling Numb Sensitive Electrical Cold/cool Sharp Cramping Pressure Sore Shooting Achy Throbbing DullSources: Lin et al, 2011resulting from, for example, diabetesor excessive alcohol intake respectively,multiple sclerosis, spinal cord damage);damage to central nervous systemtissue (for example, stroke); or loss ofsensory input to the spinal cord andbrain (such as phantom pain, brachialplexus avulsion).» Is this pain a mixture of both of the above?This sort of pain is complex and it isoften difficult to differentiate betweenthe different components. A goodexample would be chronic (long-term)back pain.» Is there an absence of a pathologicalexplanation for the pain? Some forms ofchronic pain appear to have no obviouspathological cause, yet the pain is veryreal. This pain can be triggered by apainful episode after which the painnever resolved or alterations to the wayin which the nervous system managespain signals.The words patients use to describe theirpain can often help to differentiatebetween pain arising from either nociceptive or neuropathic mechanisms (Box 2),although there is some crossover and otherknowledge will need to be used to determine the main cause of the pain.Site and radiationThe site of pain often provides information about the patient’s diagnosis andtherefore informs future treatment. Pain isusually easier to locate accurately when itis acute and somatic – that is, related tosome sort of superficial tissue damage.Deeper pain and chronic pain tend to beharder to pinpoint.Pain may have a specific cause, such asosteoarthritis of the hip, but the pain fromthis is often felt in a number of placesincluding the back, groin and knee (Izumiet al, 2014). Pain that arises from diseaseor injury to hollow organs (viscera)may also be felt in a distant cutaneous site.Fig 2 gives examples of the locations ofreferred pain.In many cases, patients can explain orpoint to the site of pain but if that is notpossible – usually because of complexity –they can draw their pain onto a body diagram (Fig 3). This involves moving the siteof their pain and other sensory symptomssuch as pins and needles on a black bodydiagram. Patients spontaneously choose touse different types of shading to denotedifferent sensations, so these prove to bean effective communication tool.Body diagrams can also offer an insightinto the psychological impact of pain: distress and frustration are often markedwith shading that is very dense, withlonger lines that sometimes extend beyondthe body (Fishbain et al, 2003); again, thepatient makes a spontaneous choicewithout guidance to use the tool in thisway, providing health professionals with avaluable insight.Associations of pain withother symptomsSome types of pain are associated withspecific symptoms – for example,sweating, pallor, nausea and vomiting arecommon in patients experiencing abdominal pain, while aura (flashing lights,blurred vision, weakness, numbness, difficulty speaking) is often associated withmigraine. Noting these symptoms is therefore relevant when trying to diagnose thecause of a pain. Symptoms associated withpain should also be investigated, such asdisrupted sleep, depression, anxiety andinability to work.14 Nursing Times 07.10.15 / Vol 111 No 41 / www.nursingtimes.netChange in pain over timePost-operative pain is an example of anacute pain that should gradually improveover a relatively short period until thepatient is pain free and able to return to,more or less, normal levels of activity.However, many patients find that theiractivity, sleep and mood may be disruptedby pain for weeks following surgery(Leegaard et al, 2010; Wiggins, 2009).Althaus et al (2014) identified thegradual improvement in post-operativepain for most people, and also demonstrated that those who have poor rate ofimprovement in pain in the early days aremore likely to go on to develop a chronicpain state (pain that does not go away). It isimportant, therefore, not to just monitorpain over time but also ensure bothpatients and nurses understand the important of pain management.Variation in intensity of pain and i
of pain. Acute pain is caused by a short-lived pathological process, such as a sur-gical incision or a sprain. Provided this pain is treated and there is no nerve damage, it usually resolves as the body heals (Grichnik and Ferrante, 1991). Chronic pain lasts for a prolonged time –