Transcription
EVIDENCE-BASED OF PAIN MANAGEMENT IN POSTOPERATIVE PATIENTSA CASE STUDYChanif**) Lecturer at School of Nursing, Faculty of Nursing and Health Science, University of MuhammadiyahSemarang, Indonesia.Address e-mail: chanif ppzakky@yahoo.co.id.ABSTRACTPain is the main reason encountered by hospitalized patients in general and surgical patients in particular.Postoperative pain is caused by tissue damage as a consequence of the surgical procedure. Nurse has roleto control and relieve of acute postoperative pain. This study aim to describe the level of acutepostoperative pain and influencing factors among the surgical patients, and evaluate the outcomes ofevidence based practice interventions in relieving acute postoperative pain. Four patients who underwentsurgery, cooperative, able to communicate and follow up for at least three days were selected as a subject.The DDQ and NRS were used to collect the data. The findings showed that the pain score decreased aftersubject received pain management intervention both pharmacologic and nonpharmacologic. Painmedication alone is not effective; they need non-pharmacologic approach as well. This studyrecommended both pain management pharmacologic and non-pharmacologic can be used together inrelieving acute postoperative pain. To improve of knowledge, in clinical setting particularly in surgicalward, nurses have to try to apply the evidence based in managing pain.Evidence-Based Of Pain Management In Postoperative Patients A Case StudyChanif91
Background of the studyPain is a common symptom found inpatients with acute and chronic illness. Painis also the main reason encountered byhospitalized patients in general and surgicalpatients in particular. Tranmer, Heyland,Dudgeon, Sequires and Coulson (2003)reported that 74 % of 69 patients includedpostoperative patient in their studyexperienced pain. Postoperative pain iscaused by tissue damage as a consequenceof the surgical procedure.The source of postoperative pain is theinjury that induced release of chemicalmediators that occurs with the acuteinflammatoryresponses.Bradykinin,substance P, and prostaglandins are releasedfrom the injured cells. Pain stimuli sensitizepain receptors so that once the brief periodof injury is over; long standing changes intheneuronsmaintainthepainpostoperatively. Some authors believe that,despite the drugs and anesthetic techniquesavailable, the prevalence of postoperativepain is still high (Apfelbaum, Chen, &Mehta, 2003; Omote, 2007; Power, 2005).Acute postoperative pain has physiological,emotional, economical, social and spiritualimpacts. These issues are as a challenge fornurse in relieving acute postoperative pain.Nurse has role to control and relieve ofacute postoperative pain by administeringpain-relieving interventions including bothpharmacologic and non-pharmacologicapproaches.Pharmachologic alone may not fully relieveall aspects of acute postoperative pain.Complementary therapy as an adjuvanttherapy may have the potential to improvepain management and palliate acutepostoperative pain (Piotrowski, Paterson,Mitchinson, Myra, Kirsh, & Hinshaw,2003).In recent years, many complementarytherapies such as massage, soothing , herbal medicines, hypnosis,and therapeutic touch have proved decreasepain level to help manage pain (Smith,Collins, Cyna, & Crowther, 2003). Those92therapies can be used to manage pain andpromotehealthyliving,andthecombination of pharmacological and nonpharmacological intervention can improvepatient opportunities for self-control overmanifestation of pain (Black & Hawks,2005).Objectives of the studyThe objectives of this study are to:1. Describe acute postoperative painexperience of surgical patients.2. Examine factors influencing acutepostoperative pain among surgicalpatients.3. Apply and evaluate the outcomesevidence based interventions in relievingacute postoperative pain.Methods of the studySubjects in this study were patients whounderwent surgery associated with asignificant degree of acute postoperativepain. They were hospitalized in a malesurgical ward Songklanagarind Hospital.Criteria for case selection in this studyinclude: 1) patients who follow minor andmajor surgery. 2) cooperative and able tocommunicate. 3) Follow up for at leastthree days.Data collection tools were used in this studyconsisted of (1) Demographic DataQuestionnaire (DDQ) and (2) Numeric PainIntensity Scale. The DDQ was derivingfrom study that developed by Hooi (2007).From 35 items, the author revised andmodified the items to be 22 items thatrelevant for this study.The pain intensity was measured by usingNumeric Pain Intensity Scale. Each patientwas asked and then mark on the numberthat best describe how much pain intensityhe was experiencing at the moment, andthen the number was recorded. The left endof the line with number zero represented nopain, number 1 to 3 represented mild pain,number 4 to 6 represented moderate pain,and number 7 to 9 represented severe pain,and number 10 represented worst possiblepain (McCaffery&Beebe, 1993).Jurnal Keperawatan Medikal Bedah . Volume 1, No. 2, November 2013; 91-96
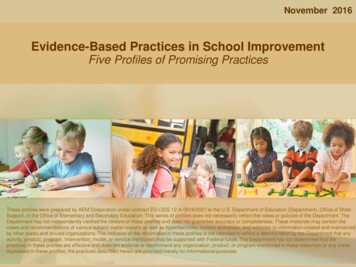
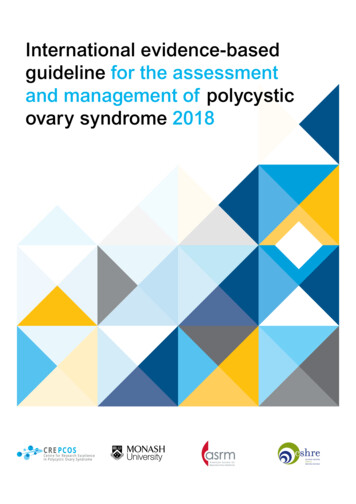
Data collection technique was based onnursing process, started from assessment,data analyzing, planning, implementation,and evaluation. In the assessment part, theinformation for DDQ were collected byusing interview method to the patient andfamily, conducted physical examination tothe patient, sought from hospitalinformation system (via computer), andpatient record. Then, continued withmeasure pain intensity by using NumericRating Scale (NRS). After collected thedata then was analyzed by using mindmapping technique to develop nursingdiagnosis related to patient problem.Furthermore, nursing care plan forintervention based on developing map toprovide holistic care and found appropriatepain intervention which suitable for patient.In term of relieving pain, beside patientreceive pain medication as usual care, nurseperformed the music therapy, foot massage,jaw relaxation and distraction technique ascomplimentary therapies and each patientcan select one intervention to beimplemented for at least 20 to 30 minutes.After the implementation, then nursereassessed the level of pain by usingNumeric rating Scale (NRS) to determinewhether those intervention effective or noteffective in relieving acute postoperativepain.FindingsTable 1Demographic data subject, data-related health, and data-related to postoperative painDemographic dataNo DataPatient 1Patient 2Patient 3Patient41Patient 4RaceThaiThaiThaiThai5Educational level Primary School Primary School Master degree Secondary cupationRubber farmer FarmerPolice retired Rubber farmerData-related healthNo8910DataAlcohol historySmoking historyPresence of family during hospitalizationData related to postoperative painNo111213DataPreoperativeinterventionPrevious surgeryMedical diagnosis14Surgicalintervention1516Type of surgeryDuration of surgery17Direction ofsurgical incisionPatient 1yesyesyesPatient 2yesyesyesPatient 3yesyesyesPatient4yesYesyesPatient 1yesPatient 2yesPatient Rightthoracotmy withbullectomyyesCa acotmy withbullectomyMajor2 hours, 25minutesVertical lateralincisionalMajor3 hours, 10minutesMidline aparatomyfor smallbowelresectionMajor3 hour, 55minuteMidlineincisionalIleocolectomywith sigmoid loopcolostomyMajor2 hour, 55minuteVertical lateralincisionalEvidence-Based Of Pain Management In Postoperative Patients A Case StudyChanif93
1819202122Length of incisionPresence ofincision drainTypes painmedicationcurrently usedTechnique ofanesthesiaNonpharmacologicalintervention20 cmICD25 cmJD20 cmICD25 ep breathingexerciseFoot siaDeep breathingexercise MusictherapyFoot massageMorphineFentanylGeneralanesthesiaDeep breathingexerciseMusic le 2Pre and post-test acute postoperative painNo1234Patient’sinitialMr. NS(POD 1-3)Mr. NS(POD 3-5)Mr. YP(POD 2-4Mr. SS(POD 3-5)Day 1Pre- Posttest -test53Day 2Pre- Posttest test43Day 3Pre- Posttesttest3172533163853434sleep121OutcomeThe average pain decreased until 2score after received interventionThe average pain decreased until 3score after received interventionThe average pain decreased until 4score after received interventionThe average pain decreased until 2score after received interventionTable 3Pain management in postoperative patientsNoPatient12Day 1Day 2Day 3Mr. NSPainmanagementPharmacologicMorphine sig 3 mgIV q 3 hrTramadol 50 mgcap sig 1x3 @pc-Mr. NSNonpharmacologicPhamacologicTramadol 50 mgcap sig 1x3 @pcParacetamol 500 mgtab sig 1 q 4 hrDeep breathing for10 minutesJaw relaxation for10 minutesand music for 20minutesFentanyl sig 30 mgIV q 3 hrMusic therapy for20 minutes-Foot massage for20 minutesMusic therapy for20 minutesDistraction readcomicNonpharmacologic34Mr. YPPharmacologicMr. orphine sig 3 mgIV q 3 hrDeep breathing for10 minutesFentanyl sig 30 mgIV q 3 hrFentanyl drip drip(0.1 mg/ml) sig 30mg IV q 3 hr, painscore is 3-Foot massage for20 minutes-Fentanyl sig 30mg IV q 3 hrFoot massage for20 minutes-Jurnal Keperawatan Medikal Bedah . Volume 1, No. 2, November 2013; 91-96
DiscussionAccording to explanation four cases above,some factors influence level of pain amongthose patients including age, gender, pastexperience with pain, culture, psychologicalfactor (anxiety) and coping mechanism due toacute postoperative pain. These factors haveinfluenced in relieving pain level from day today. In addition, preoperative intervention alsoinfluence on pain outcome that feel by thepatients.For age factor, basically ages will affects to theway of people respond to pain, whereasincreasing age is a risk factor to develop furtherpain in postoperative patient (Kehlet et al.,2006). From four cases, three cases are elderlyand one case is adult. Age factor may contributein the patient’s pain. Three cases with elderly,they had problem with pain. The pain score washigher than adult patient. The pain level wasmoderate pain. If compare with cases number 4,he is adult patient. He can manage his pain. Thelevel of pain was mild pain. A study found thatan inverse correlation between age andmorphine consumption to achieve a similarlevel of pain relief (Burns et al as cited inMamie and colleagues (2004).Gender is important factor in response to pain aswell. All of patient is men, so cannot comparewith women in this study. In this study, menpatient could manage the postoperative pain. Inone study was conducted by Berkley andHoldcroft (1999), gender was a significantfactor in the pain response, with men reportingless pain than women regardless of ethnicity. Insome cultures in the United States, boys andmen are expected to express pain less thanwomen. Men have higher tolerance with painthan women.Another factor that influence on patient’s painperception is psychological factor. Manypsychological factors that influence on painperception such as anxiety, depression. Anxietyrelated to feeling fear, dread, and worry. Two offour cases have problem with anxiety. Casenumber 2, during hospitalization, patient worryand afraid may he will suffer from the cancerdisease. He did not know about next medication.After surgery, patient will receive chemotherapyand radiation therapy. He seems stress andworry will suffer from the disease. It wassupported a study by Taezner et al., (2003).They stated that anxiety is related withpostoperative pain. Case number 4, he hadproblem anxiety as well. The fourth daypostoperative, the doctor told that he hadpotential a cancer disease. He was worry.Anxiety is often related to the meaning of thepain (Black & Hawks, 2005)The last factor that related to acutepostoperative is memory of past experienceswith postoperative pain. Two patients have pastsurgical history. Patient number 2 had surgicalhistory with cataract and patient number 4 hadsurgical history laparatomy ten years ago. Theyused past surgical history in managing his pain.A person who has had multiple or prolongedexperiences with pain will be less anxious andmore tolerant of pain than one who has had littlepain. Often, the more experience a person hashad with pain, the more frightened he is aboutsubsequent pain full events (Smeltzer & Bare,2000). Similarly a study found that pastexperience with pain affects the way currentpain is perceived. People who had a negativeexperience with pain as children have reportedgreater difficulties with managing pain (Porter,Grunau, & Anand as cited in Black & Hawks,2005).Patients were managed their pain and otherstressors in their life in many different ways.Some of them see themselves as self-sufficient,internally controlled, and independent. As aresult, they may deny or be slow to admit theyare in pain. While, others see themselves asinsufficient,externallycontrolled,anddependent on others to treat their pain(Hamilton, 2007). From this cases, culture, andethnicity can be a critical factors for patientrespond to pain (Black & Hawks, 2005). Cultureand ethnicity have an influence on how a personresponds to pain (how the pain is described orhow the patients have a response with pain).Individual factor also influence response topain, how they interpret of pain (Carvillo &Flaskerud as cited in Smeltzer & Bare, 2000).Conclusion and recommendationConclusionPain is a common problem encountered byhospitalized patients in surgical ward. Aftersurgery, its development can be predicted andshould be prevented and treated. Acutepostoperative pain can affect on physicalfunctioning, including the ability to cough andbreathe deeply, move, sleep, and perform selfcare activities. This m
Examine factors influencing acute postoperative pain among surgical patients. 3. Apply and evaluate the outcomes evidence based interventions in relieving acute postoperative pain. Methods of the study Subjects in this study were patients who underwent surgery associated with a significant degree of acute postoperative pain. They were hospitalized in a male surgical ward Songklanagarind .