Transcription
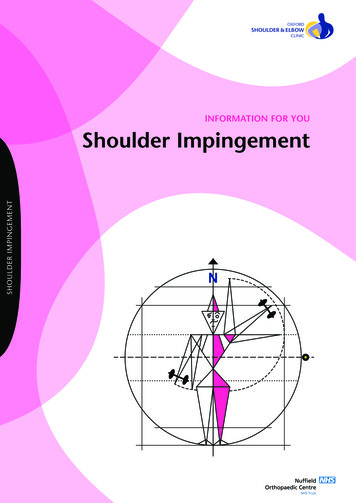
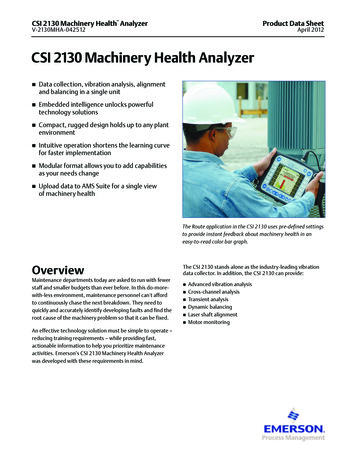
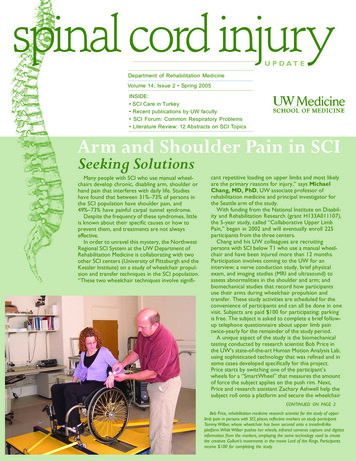
Department of Rehabilitation MedicineVolume 14, Issue 2 Spring 2005INSIDE: SCI Care in Turkey Recent publications by UW faculty SCI Forum: Common Respiratory Problems Literature Review: 12 Abstracts on SCI TopicsArm and Shoulder Pain in SCISeeking SolutionsMany people with SCI who use manual wheelchairs develop chronic, disabling arm, shoulder orhand pain that interferes with daily life. Studieshave found that between 31%–73% of persons inthe SCI population have shoulder pain, and49%–73% have painful carpal tunnel syndrome.Despite the frequency of these syndromes, littleis known about their specific causes or how toprevent them, and treatments are not alwayseffective.In order to unravel this mystery, the NorthwestRegional SCI System at the UW Department ofRehabilitation Medicine is collaborating with twoother SCI centers (University of Pittsburgh and theKessler Institute) on a study of wheelchair propulsion and transfer techniques in the SCI population.“These two wheelchair techniques involve signifi-cant repetitive loading on upper limbs and most likelyare the primary reasons for injury,” says MichaelChang, MD, PhD, UW associate professor ofrehabilitation medicine and principal investigator forthe Seattle arm of the study.With funding from the National Institute on Disability and Rehabilitation Research (grant H133A011107),the 5-year study, called “Collaborative Upper LimbPain,” began in 2002 and will eventually enroll 225participants from the three centers.Chang and his UW colleagues are recruitingpersons with SCI below T1 who use a manual wheelchair and have been injured more than 12 months.Participation involves coming to the UW for aninterview; a nerve conduction study, brief physicalexam, and imaging studies (MRI and ultrasound) toassess abnormalities in the shoulder and arm; andbiomechanical studies that record how participantsuse their arms during wheelchair propulsion andtransfer. These study activities are scheduled for theconvenience of participants and can all be done in onevisit. Subjects are paid 100 for participating; parkingis free. The subject is asked to complete a brief followup telephone questionnaire about upper limb paintwice-yearly for the remainder of the study period.A unique aspect of the study is the biomechanicaltesting conducted by research scientist Bob Price inthe UW’s state-of-the-art Human Motion Analysis Lab,using sophisticated technology that was refined and insome cases developed specifically for this project.Price starts by switching one of the participant’swheels for a “SmartWheel” that measures the amountof force the subject applies on the push rim. Next,Price and research assistant Zachary Ashwell help thesubject roll onto a platform and secure the wheelchairCONTINUED ON PAGE 2Bob Price, rehabilitation medicine research scientist for the study of upperlimb pain in persons with SCI, places reflective markers on study participantTammy Wilber, whose wheelchair has been secured onto a treadmill-likeplatform. While Wilber pushes her wheels, infrared cameras capture and digitizeinformation from the markers, employing the same technology used to createthe creature Gollum’s movements in the movie Lord of the Rings. Participantsreceive 100 for completing the study.
spinal cord injuryUPDATECONTINUED FROM FRONT PAGEso the rear wheels are in contact with two metal cylinders thatallow the wheels to turn without moving forward. “It’s basicallya treadmill for wheelchairs,” Price explained. (See photo onfront page.)Reflective markersare placed at strategiclocations on thesubject’s head, shoulder, neck, wrist, elbow,and on the hub andrim of the wheel.While the subjectpushes the wheels,information from themarkers is captured byfive infrared camerasplaced around theroom and transmittedto a computer. Software developed by Price quantifies theparameters of the markers and joint angles, reconstructs thepositions in 3-D space, and superimposes pushrim force datafrom the SmartWheel.“This is the same technology used to create Gollum’smovements in the Lord of the Rings movie and the Tom Hankscharacter in Polar Express,” Price said. On the computer screen,the markers show up dramatically as little points of light—likestars in a constellation—in motion against a black background.Subjects perform this activity for 30-60 seconds at threedifferent speeds. They also are asked to carry out acceleration,braking and transferring activities while data are recorded.These data, along with information about upper limb pain anddisability from questionnaires, MRIs, etc., are sent to the study’scoordinating center in Pittsburg for analysis.“We’re trying to correlate evidence of injury to the way peopleare using their wheelchairs,” Price said. “Eventually we want tosee what variables are relatedto injury and abnormalities. Ifwe understand the injurymechanism, hopefully we canimprove propulsion techniques and wheelchairdesigns to prevent these kindsof injuries.” The researchersneed a large number ofsubjects in order to get areliable and complete pictureof what’s causing theseproblems.While participants don’tget any direct personal benefit from taking part in the study(aside from 100), contributing toward a worthy research efforthas other rewards. “Research is really important,” said TammyWilber (seen in photo), who participated in the study andrecommends others give it a try. “If you can give a few hours tobenefit the lives of people with SCI, it’s worth it. Plus, it’s fascinating! When I watched (the documentary about) how they madeGollum in the movie, I could say, ‘Hey, I did that!’”For more information about participating in this study, pleasecontact Zachary Ashwell at 206-543-3720.This is the same technology usedto create the Gollum character’s movementsin the movie Lord of the Rings.See more photos in the online version of this article 5 spring.htmlSpinal Cord Injury Care In TurkeyBilge Yilmaz, MD, (see photo) is spending a year at the University ofWashington as a rehabilitation medicine fellow with Dr. Diana Cardenas.Yilmaz is a rehabilitation medicine physician in the SCI Unit of the TurkishArmed Forces Rehabilitation Center (www.rehab.gata.edu.tr) in Ankara,Turkey.We asked him to tell us about himself and SCI care in Turkey.The Turkish Armed Forces Rehabilitation Center (TAFRC) where I work is amodern facility serving persons withdisabilities from all over Turkey andneighboring countries. It is the largestrehab facility in the country—a state-ofthe-art center that is probably amongthe most comprehensive in the world. Itincludes a wide range of services, fromgait analysis and cardiopulmonaryexercise testing laboratories to bonedensitometer and a hyperbaric chamber.There are two gymnasiums, five exerciserooms dedicated to orthopedic rehab,neurologic rehab, hand therapy,outpatient therapy and pediatric rehab;2 VOLUME 14, ISSUE 2two large and two small aquaticrehabilitation pools; vocational,occupational and recreationaltherapy units; speech andcognitive therapy; as well ashydrotherapy and electrotherapy.TAFRC serves 400 SCIpatients per year and houses 200 activepatient beds, 50 nursing home beds, anda 50-bed patient hotel. In addition to anacute care unit, TAFRC has separaterehabilitation units for patients with SCI,brain injury, stroke, amputation, andrheumatology.S P I N A L C O R D I N J U RY U P DAT EThe annual incidence of SCI in Turkeyis about 12.7 cases per million population, significantly lower than the U.S.rate of 40 per million. Approximately71% percent of injuries in Turkey occuramong males, compared to 78.2%among males in the U.S. The average ageCONTINUED ON PAGE 3SPRING 2005
spinal cord injuryUPDATECONTINUED FROM PAGE 2at injury is 35.7 years, (38 years in theU.S.), and like the U.S., the mostcommon causes of injury in Turkey aremotor vehicle accidents, followed byfalls, violence and sports-related injuries.The most common level of injury in bothcountries is C5.The total length of hospital stay (acuteand rehab) for SCI patients in Turkey islonger than in the U.S. (95 versus 55,respectively), mainly because PT and OTservices in Turkey are primarily availableonly in the hospital setting.Patients at our center can takevocational and recreational courses suchas computer sciences, marbling, woodand metal works, painting and sculpture.These are provided by the TurkishMinistry of Education. The center has awheelchair basketball team, an amputeesoccer team, an archery team and agoal-ball team (a sport for people withvisual impairments); many of these teamsrepresent our country in theParalympics.Turkey’s health care system consistsof both public and private entities.About 85% of the citizenry has somekind of health insurance coverage, eitherthrough federal programs like the SocialInsurance Organization and the Retirement Fund, or through private insurance. Most health facilities (63%) areoperated by the Ministry of Health, 19%are private, 10% are run by the SocialInsurance Organization, and theremainder are operated by the militaryand other public institutions.In Turkey, we have a lifelong follow-upprogram for patients with SCI and invitethose people to come back at least oncea year for overall check-ups. Reproductive services such as in vitro fertilizationare offered to SCI patients through theDepartment of Gynecology and Obstetrics at Gulhane Military Medical Schoolin Ankara.This is my first visit to the UnitedStates. TAFRC sent me here to improvemy clinical skills in SCI rehabilitation,learn more about the U.S. health caresystem, observe the strategies used toreintegrate people with SCI into thecommunity, and to open wide a door forcollaborative studies. I chose Seattlebecause of the distinguished reputationsof Dr. Cardenas and her colleagues inthe UW Department of RehabilitationMedicine. Right away I saw that I madethe right decision in choosing the UWand that I am lucky to have the chanceto live in such a beautiful city.My special research interests are inbone mineral metabolism and theprevention and treatment of osteoporosis in SCI. While in Seattle, I am helpingDr. Cardenas with her UTI preventionresearch study and together we aredeveloping an osteoporosis study.—Bilge Yilmaz, MDSee photos from Turkey in the online version of this article at: http://depts.washington.edu/rehab/sci/updates/05 spring.htmlRecent SCI-related publications by UW faculty Bombardier CH, Stroud MW, Esselman PC, Rimmele CT. Do preinjury alcohol problems predict poorer rehabilitationprogress in persons with spinal cord injury? Arch Phys Med Rehabil 2004; 85(9):1488-1492. Bombardier CH, Richards JS, Krause JS, Tulsky D, Tate DG. Symptoms of major depression in people with spinal cord injury:implications for screening. Arch Phys Med Rehabil 2004; 85(11):1749-1756. Burns SP, Weaver FM, Parada JP, Evans CT, Chang H, Hampton RY, Kapur V. Management of community-acquired pneumonia in persons with spinal cord injury. Spinal Cord. 2004 Aug;42(8):450-8. Cardenas DD, Hoffman JM, Kirshblum S, McKinley W. Etiology and incidence of rehospitalization after traumatic spinal cordinjury: a multicenter analysis. Arch Phys Med Rehabil 2004; 85(11):1757-1763. Cardenas DD, Bryce TN, Shem K, Richards JS, Elhefni H. Gender and minority differences in the pain experience of peoplewith spinal cord injury. Arch Phys Med Rehabil 2004; 85(11):1774-1781. Vaccaro AR, Kim DH, Brodke DS, Harris M, Chapman JR, Schildhauer T, et al. Diagnosis and management of sacral spinefractures. Instr Course Lect 2004; 53:375-385. Deyo RA, Nachemson A, Mirza SK. Spinal-fusion surgery - the case for restraint. N Engl J Med 2004; 350(7):722-726. Hastings J, Goldstein B. Paraplegia and the shoulder. Phys Med Rehabil Clin N Am 2004; 15(3):vii, 699-vii, 718. Panagos A, Jensen M, Cardenas DD. Treatment of Myofascial Shoulder Pain in the Spinal Cord Injured Population UsingStatic Magnetic Fields: A Case Series. J Spinal Cord Med 27(2):138-142, 2004. Jensen MP, Hanley MA., Turner JA, Cardenas DD. Pain and other sensations in persons with spinal cord injury: Frequencyand association with depression and pain interference. Psychologica 37:129-143, 2004. Masedo AI, Hanley M, Jensen MP, Ehde D, Cardenas DD. Reliability and Validity of a Self-Report Functional IndependenceMeasure (FIM-SR) in Persons with Amputation or Spinal Cord Injury and Chronic Pain. Am J Phys Med Rehabil 84:167-176, 2004. Little JW, Ditunno JF, Jr. Soleus H-reflex in spastic spinal cord injury patients. Arch Phys Med Rehabil 2004; 85(12):2070-2071. Ditunno JF, Little JW, Tessler A, Burns AS. Spinal shock revisited: a four-phase model. Spinal Cord. 2004 Jul;42(7):383-95. Han JJ, Massagli TL, Jaffe KM. Fibrocartilaginous embolism—an uncommon cause of spinal cord infarction: a case report andreview of the literature. Arch Phys Med Rehabil 2004; 85(1):153-157. Bryden AM, Kilgore KL, Lind BB, Yu DT. Triceps Denervation as a Predictor of Elbow Flexion Contractures in C5 and C6Tetraplegia. Arch Phys Med Rehabil 2004; 85(11): 1880-1885.U N I V E R S I T Y O F W A S H I N G TO N S C H O O L O F M E D I C I N ED E PA RT M E N T O F R E H A B I L I TAT I O N M E D I C I N E 3
forum reportThe SCI Forum is an evening presentation and discussion series on topics of interest to persons with spinal cord injury and their family members,friends, and caregivers, held monthly at the University of Washington Medical Center during the fall, winter and spring. To learn about upcoming SCIForums or read reports of past forums, consult our Web site at http://depts.washington.edu/rehab/sci/forum.html. Contact Cynthia Salzman (email:csalzman@u.washington.edu; phone: 206-685-3999) if you wish to be added to the SCI Forum mailing list.Common Respiratory Problems in SCIWhat You Need to KnowOctober 12, 2004—Respiratoryproblems that aren’t usually severe inthe general population can be quiteserious or even life-threatening inpersons with SCI, according to StephenBurns, MD, assistant professor in theUW Department of RehabilitationMedicine.“Respiratory infections, especiallypneumonia, are the leading cause ofdeath (about 20%) in SCI,” said Burns,but account for less than 3% of deathsin the general population. Sleep apnea—pauses in breathing while sleeping—isanother problem that is more commonand more severe in the SCI population.These problems are preventable andtreatable, Burns added, but many healthcare providers aren’t aware they can bemore severe and require differenttreatments in people with SCI.Pneumonia—why is it socommon and severe in SCI?Part of the answer lies in an understanding of the way SCI affects breathingmuscles. Breathing is a two-step process:inspiration (breathing in) and expiration(breathing out). While inspiration isaffected mainly in those at C5 andabove, expiration is a problem with allinjury levels down to T12.“People with injuries down to T12may have sufficient ability to move air inand out during regular breathing, but aprofound weakness in their ability tocough,” Burns said. “If you can’t coughwell, you can’t bring up phlegm (mucus)from your lungs, and it starts poolingthere.” It’s harder to treat respiratoryinfections in SCI patients because theycan’t clear their own secretions adequately. In time, breathing becomesharder as lungs fill with more secretions.This can lead to pneumonia.When the cough ability is weak,secretions have to be mobilized (removed) in some other way, such assuctioning or quad coughing. Thesemethods clear some but not all secretions.4 VOLUME 14, ISSUE 2A better method is the Mechanicalinsufflator-exsufflator (MI-E). “This isessentially a very expensive ( 4,000)reversible shop-vac,” Burns said. Itinflates the lung, then simulates a coughwhen the flow is reversed. “The air flowis similar in velocity to a cough, so it’svery effective in pulling secretions out ofthe lungs. Not surprisingly, it’s stronglypreferred by patients over suctioning.”Sleep ApneaTreatment and preventionof pneumoniaSleep apnea in SCIcan cause depression,high blood pressure,poor wound healing, andeven sudden death.Pneumonia in SCI patients should betreated aggressively with strong intravenous antibiotics that are effective againstthe highly resistant bacteria Pseudomonas—rare in the general population, butmore widespread in SCI. Because of theseverity of pneumonia in the SCIpopulation, Burns believes that “anybodywith a complete cervical injury oranyone with a motor incomplete injurybut a weak cough should be hospitalized” if they get pneumonia.“Some pneumonias are probablypreventable with the vaccinePneumonvax,” Burns said. “Everybodywith SCI should receive it once,” andpossibly again after age 65 if more than5 years have elapsed since the lastvaccination.Prevention strategies include dailyclearing and inflating lungs. “Thesemethods need to be stepped up if apatient develops a cold, bronchitis, orsome sort of upper respiratory infection,to keep it from developing into apneumonia,” Burns said.Influenza vaccines“The flu can make you just as sick (aspneumonia), and people can die fromthe flu,” Burns stated. “Even if youconsider yourself healthy, people withSCI are considered a priority group, andwe recommend that they receive fluvaccine yearly.”S P I N A L C O R D I N J U RY U P DAT ESleep apnea is defined as pauses thatoccur in the breathing at night, alongwith severe snoring and/or excessivedaytime sleepiness, Burns said. “Yoursleep is disrupted, sometimes hundredsof times a night, and you’re not gettingrestful sleep because your brain ishaving to wake up to tell your body tokeep breathing.” People usually have noawareness that they are waking up.Sleep apnea causes excessive daytimesleepiness, cognitive dysfunction (troublethinking and concentrating), high bloodpressure, cardiac and pulmonarydisease, and motor vehicle accidents. “Ifsomeone has high blood pressure thatdoesn’t respond to the usual medications, there’s a very good chance theperson has sleep apnea,” Burns noted.While sleep apnea occurs in about3% of the general population, it is tentimes more common in the SCI population. Up to 40% of persons with tetraplegia (quadriplegia) have sleep apnea.Sleep apnea in the SCI populationcauses all the problems of the generalpopulation, but also has the arguablymore serious consequences of interfering with learning and improvementduring the rehabilitation period; depression and difficulty with emotionalCONTINUED ON PAGE 5SPRING 2005
forum reportspinal cord injuryUPDATECONTINUED FROM PAGE 4adjustment; ulcer formation and poor wound healing due tolow oxygen at night; and even sudden death.The harm caused by sleep apnea depends on its severity,namely, “how frequently your breathing stops, how long itstops, how low your oxygen level goes,” Burns said. “For somepeople it’s mild; for others, it’s going to shorten their lives.”Sleep apnea can be diagnosed with a sophisticated sleepstudy called a polysomnography, or at a minimum, a sleep testthat records your oxygen levels at night.The most common treatment is Continuous Positive AirwayPressure (CPAP) therapy, which consists of a bedside unit andhose that keeps the airway open by delivering pressurized airinto the lungs through a mask worn over the mouth and nose.Since persons with limited hand function may not tolerate thistreatment well because of the inability to reposition the maskindependently during the night, an occupational therapist canwork with patients to modify the mask with a hook or ring sothe user can make adjustments independently.Burns reported that once CPAP treatment begins, patientsusually notice a benefit right away and “don’t want to bewithout (the CPAP equipment) or to travel without it. They feelmore alert. That’s the main thing people perceive. Heartproblems like high blood pressure are more likely to creep upon people.”Issues to discuss with your health careprovider Everyone with SCI has a high risk for pneumonia andinfluenza and should request immunization from their
tion Center (TAFRC) where I work is a modern facility serving persons with disabilities from all over Turkey and neighboring countries. It is the largest rehab facility in the country—a state-of-the-art center that is probably among the most comprehensive in the world. It includes a wide