Transcription
Acute Pain:Pathophysiology and ClinicalImplicationsTimothy J. Brennan, PhD, MDDepartment of AnesthesiaUniversity of Iowa Hospitals and ClinicsIowa City, Iowathe perioperative period.3 One component of the pathophysiology in surgery is acute postoperative pain.Our long-term goal will be to eliminate postoperativepain. This will require that we develop a better understanding of the mechanisms for surgical pain and prepare to use recent discoveries in biomedical research.4rogress in postoperative pain management decreasesmorbidity after surgery.1 To advance patient care,reduce perioperative morbidity, and decrease healthcare costs, it is critical that we improve acute postoperativepain management. Our armamentarium of drugs for acutepain management has been limited to opioids, controlleddelivery of local anesthetics, and nonsteroidal antiinflammatory drugs or acetaminophen. For acute painmanagement, we operate using guidelines from the early1990s that reinforced the generous use of opioids for acutepain even though effective dosing is limited by deleteriousside effects. Anesthesia-based acute pain services popularized continuous epidural analgesia, which controls painbetter during activities and continuous regional techniquesfor specific surgeries. If the 1990s assured us opioidsshould be used with confidence, the last 5 years has demanded efficacious alternatives to opioids with fewerside effects and, perhaps, improved outcome. This is incontrast to patients with rheumatoid arthritis who may betreated with drugs that block the action of inflammatorymediators such as tumor necrosis factor or interleukin-1(IL-1).2With increasing new knowledge and techniques comeimportant opportunities and challenges for developing insights into the causes, mechanisms, and treatment of human disease. For anesthesiologists, we have an opportunityto treat surgery and trauma as a disease, and this requiresinvestigation into the pathological processes that occur inPIf the 1990s assured us opioids shouldbe used with confidence, the last 5 yearshas demanded efficacious alternativesto opioids with fewer side effects and,perhaps, improved outcome.As we learn more about the etiology for postoperativepain, we will develop mechanism-based, disease-specifictreatments. This paper will examine clinical pathophysiology of postoperative pain and recent discoveries aboutincisional pain.CLINICAL POSTOPERATIVE PAINMost patients have pain at rest after surgery. This is measured using visual or verbal pain scales in the absenceof any provocative maneuvers. Pain with activities after8
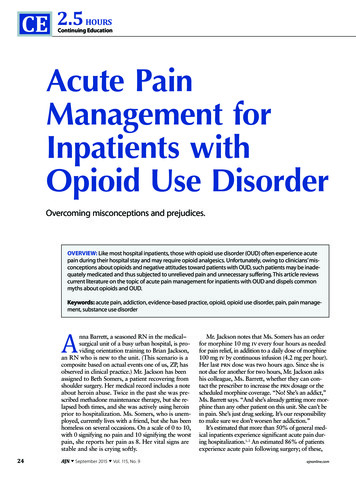
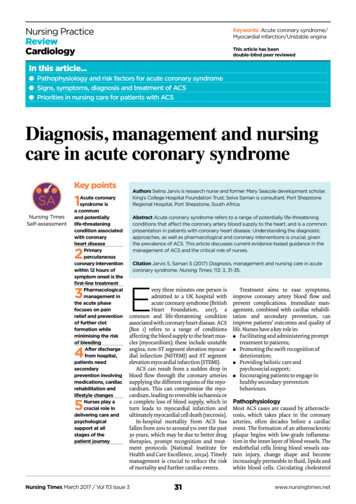
9Acute Pain PhysiologyFigure 1. A, Pain at rest pain and during flexion after unilateral total knee arthroplasty: visual analog scale (VAS) pain scores at rest and during knee flexionafter total knee replacement and optimized pain treatment with patient-controlled analgesia using opioids (Adapted from Singelyn FJ, et al.: Anesth Analg1998; 87:88–92).5 Small squares connected by lines are VAS scores and large squares are the degree of flexion associated with the pain score. B, Pain at restand during cough after hysterectomy: schematic of VAS pain scores at rest and during cough after abdominal hysterectomy and optimized pain treatment withpatient-controlled analgesia using morphine. (Reprinted with permission and adapted from Moiniche S, et al.: Acta Anaesthesiol Scand 1997; 41:785–9.)6surgical operations should be measured using functionswhich are related to morbidity. For example, pain withknee flexion after total knee replacement is a measure ofevoked pain (Figure 1A).5 Early improvement in pain withflexion and improved range of motion have been shown toproduce sustained increases in function for weeks tomonths after surgery.After abdominal and thoracic surgical procedures,patients complain of pain at rest that is typically presentfor 3-5 days after surgery (Figure 1B).6 In some cases, theduration may be greater. Pain measured with activitiesvaries depending on the type of surgery. For abdominalsurgical procedures, pain evoked by coughing, movement,and pressure is also present. Such evoked pain is greaterthan pain at rest, tends to be poorly responsive to opioids,and is present for a longer period of time especially withmore extensive upper abdominal and thoracic procedures(Table 1).Other Pain MeasurementsOther pain tests have been explored in patients to attemptto understand sensitization and further quantitate post-Table 1. Methods to Measure Pain in Patients AfterSurgery and Example Surgery for Each MeasurementClinical Postoperative PainClinical ExamplePain at restAny surgeryPain during activities: standingHip replacementPain during activities: ambulationHip replacementPain during activities: cough, spirometryAbdominal or thoracic surgeryPain during activities: kneeflexion/extensionKnee replacementPressure pain thresholdAbdominal surgeryArea of mechanical hyperalgesiaNephrectomyFlexion response to mechanical stimuliPediatric hernia repairSwallowingTonsillectomyoperative pain. One of these tests is punctate secondaryhyperalgesia, usually mapped or quantified by a smallpunctate mechanical stimulus applied outside the areaof an incision, for example, after nephrectomy7 or colectomy.8 In some cases the force required to provoke painafter surgery is quite small indicating a touch stimulus hasbeen converted to pain by the surgery.7 This remote hyperalgesia is secondary because the test site is outside thearea injured by the incision, the area of primary hyperalgesia (Figure 2). Central nervous system sensitizationcauses pain in the secondary zone because the sensory fibers function normally outside the area of injury.9 Evidence indicates ketamine administration intraoperativelyand in the immediate postoperative period produces sustained inhibition of secondary hyperalgesia after surgery(Figure 2).In one study of pediatric patients, the primary punctateforce for the abdominal flexion reflex was measured inchildren after herniorraphy.10 A weak force provoked aflexion response after surgery and the response magnitudewas increased as well. Using a different mechanical testafter hysterectomy, a blunt probe was applied near or distant to the incision and the threshold pressure that evokedpain was recorded.6 Again a widespread area of sensitivitycan be measured and this persisted for up to 1 week aftersurgery. These tests have the advantage in that the stimulusintensity can be quantified.In clinical postoperative studies, analgesics must beavailable as needed and therefore, superimposed on painscales and measurements is the patients analgesic consumption, which may confound the detection of a noveltreatment. Furthermore, a problem with some evoked painmeasures such as pain during cough is that there is difficulty to standardize the effort.PREEMPTIVE ANALGESIAThe search for preventive analgesic treatments with prolonged benefits continues in part because pain research has
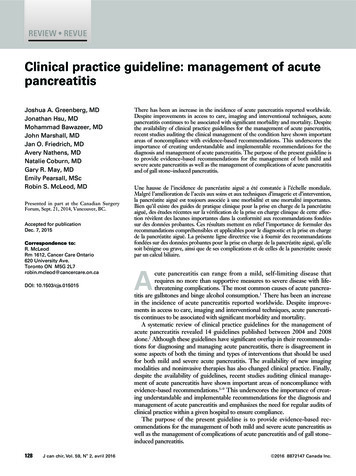
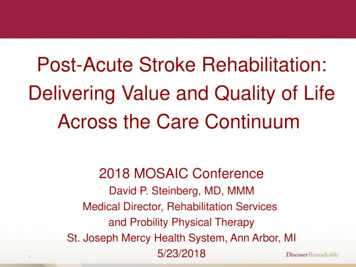
10BrennanFigure 2. A, Area of hyperalgesia to von Frey filament applications in patients after nephrectomy treated with opioids for postoperative pain control. B, Area ofhyperalgesia in patients after nephrectomy treated with opioids and ketamine infusion for postoperative pain. (Adapted from Stubhaug A., et al.: ActaAnaesthesiol Scand 1997; 41:1124–32.)7emphasized the plasticity of the nociceptive system andpain memory. The perioperative period is ideal for translating concepts such as pain memory, plasticity, and preventive treatments because the nature of the injury(surgery), its onset, duration and degree are generallyknown; in addition, the patients can be assessed before theinjury to evaluate the role of predisposing factors (genetic,psychosocial, etc.).The perioperative period is ideal fortranslating concepts such as painmemory, plasticity, and preventivetreatments because the nature of theinjury (surgery), its onset, duration anddegree are generally known; inaddition, the patients can be assessedbefore the injury to evaluate the roleindicate short-term benefits of regional anesthesia.12 Forexample, in a study comparing nerve block to generalanesthesia after upper extremity surgery, patients whoreceived nerve block bypassed the postanesthesia care unitmore frequently, reported less pain, ambulated earlier, andwere ready for home discharge sooner (Figure 3).13 Forfollow-up, there was no significant difference betweengroups in pain scores and medication use.We must be careful and not conclude that plasticity andpain memory have little role in postoperative pain. It isimportant to note that clinical plasticity may depend on avariety of issues such as the kind of surgery, the type andduration of the treatment strategy, the analgesic or painmodality tested and the characteristics of the patient beforesurgery. The exact model for sensitization and plasticity inperioperative care has not been determined. Plasticity maybe present on nociceptive nerve terminals producingenhanced responses in these primary afferents–peripheralsensitization. A much greater emphasis has been made onplasticity of pain transmission in the central nervous system. In the future, it is important for anesthesiologists andsurgeons to determine how these plasticity models shouldapply to perioperative care. Furthermore, what treatmentsare effective and the duration of neuroplasticity treatmentmust be determined.of predisposing factors (genetic,psychosocial, etc.).Thus, an important goal in perioperative medicine is topretreat postoperative pain so that long-term benefits canbe gained.11 Trials of preemptive analgesia compare theeffect of drugs administered before injury with the sametreatment administered after injury.Clinical trials of preemptive analgesia using randomized, controlled protocols strongly indicate that conventional treatments such as local anesthetics and opioids donot exhibit significant preemptive analgesic effects forpostoperative pain. Most studies evaluating short-termand long-term effects of local/regional anesthesia largelyFigure 3. Pain evaluation and treatment of patients undergoing outpatientupper extremity surgery under regional (Reg) or general (Gen) anesthesia.Percent of patients with visual analog scale pain score greater than 3 andpercent of patients requiring treatment in the recovery room are shown.Marked short-term benefits in regional anesthesia are noted. Benefitsbeyond the day after surgery were not apparent.13 There was no laterreduction in pain and opioid use. (Adapted from Hadzic A, et al.:Anesthesiology 2004; 101:127–32.)
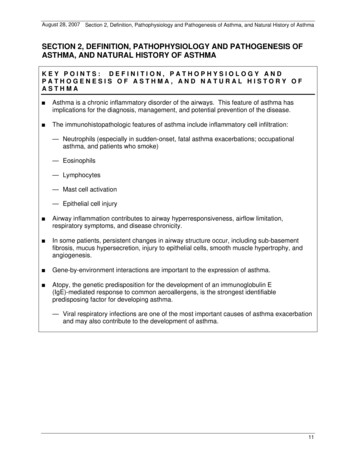
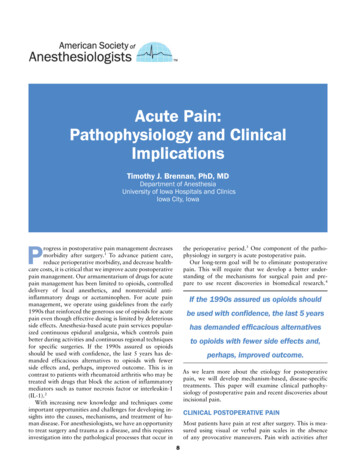
Acute Pain Physiology11Acute Opioids Tolerance and HyperalgesiaEarly studies examined preemptive and preventativeopioid analgesia for postoperative pain relief after majorsurgeries. These results largely were lacking in positiveresults. More recent studies suggest there may be negativeeffects of early administration of high-dose opioids in theintraoperative period. Some studies indicated that administration of a high but not a low intraoperative opioid dosewas associated with either increased pain or greater opioidconsumption in the postoperative period. Not all studiesare in agreement with these findings. Further studies willbe needed to determine whether the development of acutetolerance in patients exposed to a high intraoperativeopioid dose occurs and if acute opioid-induced hyperalgesia develops in the postoperative period.The direction of perioperative medicine must emphasizepreventative analgesia studies, and: Pretreatment analgesia studies using novel treatmentstrategies.Examine the potential long-term benefits of analgesictreatments by better understanding persistent painthat occurs for up to 6 weeks after surgery.Modification of the development of chronic pain aftersurgery.Nonopioid analgesic treatments.Therapies that modify the acute and chronic opioidstolerance.HUMAN MODELS FOR INCISIONALPOSTOPERATIVE PAINKawamata et al.14 subjected volunteers to a small incisionin the volar forearm to examine the etiology of pain causedby incisions (Figure 4). Experiments such as these contribute to our understanding of the mechanisms for postoperative pain and make an important link betweenclinical postoperative pain and basic research in animalson pain mechanisms caused by incisions. Spontaneousongoing pain was maximal when the incision was madeand then it decreased and disappeared within 30 minutes(Figure 4A). There was no sustained spontaneous painafter incision. Primary hyperalgesia was apparent immediately after incision and maintained for several days.This study indicates that small 4-mm incisions in humansproduce only transient ongoing pain but persistent hyperalgesia for several days (Figure 4B). The disappearance ofpain at rest and maintenance of pain with activities and inresponse to mechanical stimuli at the wound site is alsopresent in patients after surgery.6 Furthermore, evokedpain in patients is longer lasting than ongoing pain. Boththis translational study and other clinical studies show thatpain at rest caused by incisions and evoked pain are likelytransmitted by different afferent fiber populations and/ordifferent receptors. For incisions, enhanced responsivenessof central neurons and pain require ongoing afferent inputfrom the incision.Figure 4. A, Pain after skin incision: average visual analog scale pain score atrest after incision in the volar forearm of volunteers. B, Primary hyperalgesiaafter skin incision: pain threshold for primary mechanical hyperalgesia afterincision in the volar. Box and whisker plots indicate data expressed as median(horizontal line) with first and third quartiles (boxes), and 10th and 90thpercentiles (whiskers). C, Areas of mechanical pain after skin incision: averagearea of hyperalgesia after incision in the forearm. Reprinted with permissionfrom Kawamata M, et al.: Anesthesiology 2002; 97:550–9.Infiltration with a local anesthetic to block the painbefore the experimental incision initially prevented ongoing pain and the primary mechanical hyp
physiology in surgery is acute postoperative pain. Our long-term goal will be to eliminate postoperative pain. This will require that we develop a better under-standing of the mechanisms for surgical pain and pre-pare to use recent discoveries in biomedical research.4 If the 1990s assured us opioids should beusedwithconfidence,thelast5years