Transcription
Pain Management and Opioids:Balancing Risks and BenefitsPRESENTED BYU P D AT E D J a n u a r y 2 0 2 01 CO*RE 2020
ACKNOWLEDGMENTSPresented by the American Society of Addiction Medicine, a member ofthe CO*RE Collaborative, nine interdisciplinary organizations workingtogether to improve pain management and prevent adverse outcomes.This curriculum fully covers to the September 2018 FDA Blueprint.3 CO*RE 2020
THE CO*RE COLLABORATIVE4 CO*RE 2020
FACULTY ADVISORY PANELDavid Bazzo, MDRon Crossno, MDU C S AN D I E G OKINDRED AT HOMEKatherine Galluzzi, DO Carol Havens, MD Randall Hudspeth, APRNPHILADELPHI A COLLEGEOF OSTEOPATHIC MEDICINEK AI S E R P E R M AN E N T EPRACTICE CONSULTANTCO*RE FACULTY ADVISORSAND ALL PLANNERSHAVE NORELEVANT FINANCIALRELATIONSHIPS5 Dennis Rivenburgh, PA-C Edwin Salsitz, MDBarb St. Marie, ANPJ O H N S H O P K I N S S C H O O L MOUNT SINAI BETH ISRAELOF MEDICINEUNIVERSITY OF IOWA CO*RE 2020
BY THE END OF THIS SESSION YOUWILL BE ABLE TO Describe the pathophysiology of pain as itrelates to the concepts of painmanagement. Accurately assess patients in pain. Develop a safe and effective pain treatmentplan. Identify evidence-based non-opioid optionsfor the treatment of pain. Identify the risks and benefits ofopioid therapy. Manage ongoing opioid therapy. Recognize behaviors that may beassociated with opioid use disorder.6 CO*RE 2020
WHY ARE WE HERE?7 CO*RE 2019
CO*RE STATEMENTMisuse, abuse, diversion, addiction, and overdose of opioids in theUnited States have created a serious public health epidemic.When prescribed well, and used as prescribed, opioids can be valuabletools for effective pain management.There is potential for unintended consequences of inadequatelymanaged pain from far-reaching prescribing restrictions.This course does not advocate for or against the use of opioids. Weintend to help healthcare providers manage pain without puttingvulnerable patients at risk for misuse or opioid use disorder. The goal is tokeep our patients, our communities, and ourselves SAFE.8 CO*RE 2020
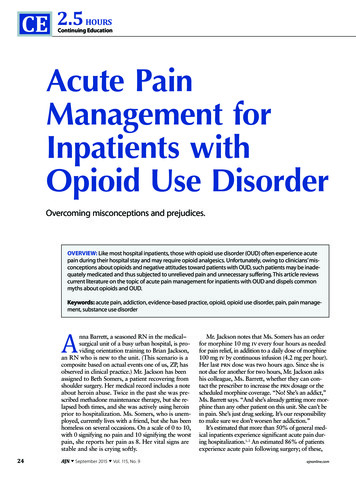
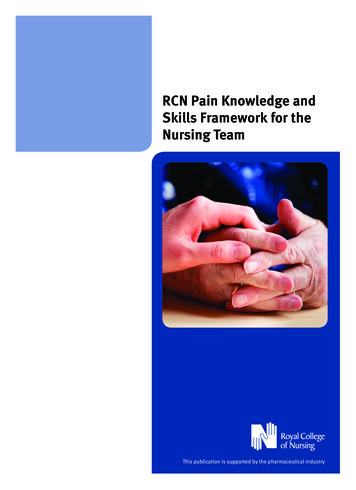
PRESCRIBING PATTERNS AND OPIOID-RELATED DEATHSLegally prescribed opioids9 CO*RE 2020SOURCE: CDC Opioid Overdose Death data, IQVIA opioid prescribing data, Sullum data.htm
DEA SCHEDULED DRUGSSCHEDULEDESCRIPTIONEXAMPLESIHigh potential for abuse; nocurrently accepted medical useHeroin, LSD, cannabis, ecstasy, peyoteIIHigh potential for abuse, whichmay lead to severe psychologicalor physical dependenceHydromorphone, methadone, meperidine,oxycodone, fentanyl, morphine, opium,codeine, hydrocodone combination productsIIIPotential for abuse, which maylead to moderate or low physicaldependence or high psychologicaldependenceProducts containing 90 mg codeine perdose, buprenorphine, benzphetamine,phendimetrazine, ketamine, anabolic steroidsIV“Low potential” for abuseAlprazolam, benzodiazepines, carisoprodol,clonazepam, clorazepate, diazepam,lorazepam, midazolam, temazepam, tramadolVLow potential for abuseCough preparations containing 200 mgcodeine/100 mlComplete list of products covered under the Opioid Analgesic REMS available at: https://opioidanalgesicrems.com/RpcUI/products.u10 CO*RE 2020
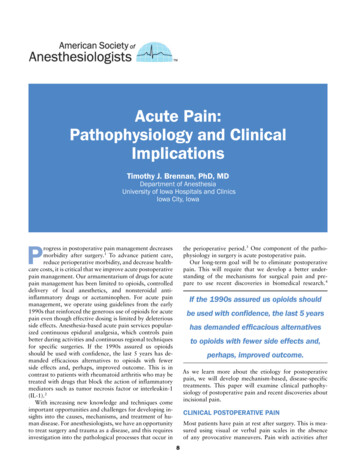
FENTANYL AND FENTANYL ANALOGUESOverdose deaths from street fentanyl and fentanyl analogues, such ascarfentanil, have increased 540% in three years.Street fentanyl is illegally manufactured; it is generally NOT a divertedpharmaceutical product.Two causes of fentanyl OD death: opioid-induced respiratorydepression and rigid chest wall syndrome; higher or repeated doses ofnaloxone are required to reverse a fentanyl overdose.Fentanyl is also unknowingly mixed with heroin, cocaine, and methamphetamine, whichcontributes to OD deaths.11 CO*RE 2020Photo source: New Hampshire State Police Forensic Laboratory
RISKS VERSUS BENEFITS OF PRESCRIBED OPIOIDSRISKSBENEFITS Misuse, diversion, and addiction Abuse by patient or household contacts Interactions with other meds and substances Risk of neonatal abstinence syndrome Inadvertent exposure/ingestion by householdcontacts, especially children Life-threatening respiratory depression Overdose, especially as ER/LA formulationscontain more MME than IRAnalgesia- Reliable pain control- Quick analgesia(particularly with ImmediateRelease) Continuous, predictable(with ExtendedRelease/Long-Acting)Improved function Improved quality of lifeSOURCE: Nicholson, B. Pain Pract. 2009;9(1):71-81. 2500.2008.00232.x/abstract12 CO*RE 2019
CHAPTER 1PAIN13 CO*RE 2020
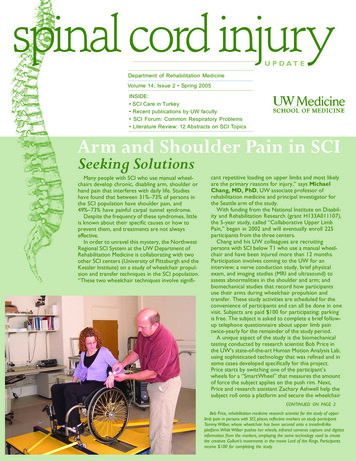
THE NEUROMECHANISMS OF PAINPeripheral PainModulators: Histamines Prostaglandins Cytokines Bradykinin Substance P OthersDescendingNeurotransmitters: Serotonin Norepinephrine Endogenous opiates Others14 CO*RE 2020
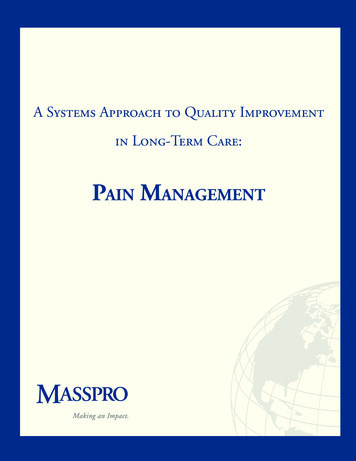
MEDIATORS OF PERIPHERAL NOCICEPTIONFeeling physical pain is vitalfor survival; pain is the body’searly warning system.With thanks to Allan Basbaum and David Julius, University of California, San Francisco15 CO*RE 2020
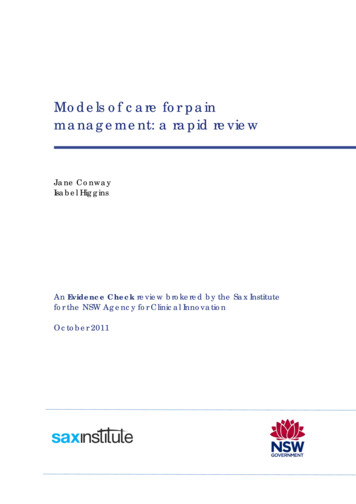
OPIOID RECEPTOR LOCATIONS16 CO*RE 2020
TYPES OF PAINNOCICEPTIVE /INFLAMMATORYPain in response toan injury or stimuli;typically acutePostoperative pain,sports injuries,arthritis, sickle celldisease,mechanical lowback painNOCIPLASTICPain that arises fromaltered nociceptivefunction; typicallychronicFibromyalgia,irritable bowelsyndrome, nonspecific low backpainNEUROPATHICPain that developswhen the nervoussystem is damaged;typically chronicPost-herpeticneuralgia, trigeminalneuralgia, distalpolyneuropathy,CRPS, neuropathiclow back painPossible development of chronic pain after an acute injury.17 CO*RE 2020MIXED TYPES(NOCICEPTIVE /NEUROPATHIC)Primary injury andsecondary effects
THE BIOPSYCHOSOCIAL SPIRITUAL CONTEXT OF nal statusBIOLOGICALSOCIALWork GICALSPIRITUALValues*ACEs Adverse Childhood ExperiencesExperience of PainCO*RE 2020Religious faithExistential issuesSpiritual distressFamily DepressionSufferingFinances18 ACEs*GriefConditioningPrevious painexperienceResilienceEmpathyfromHCP
PAIN CATASTROPHIZING “Tell me about your pain ” Listen for rumination,feelings of hopelessness, oranticipation of negativeoutcomes. These feelings are importantto identify because they canprolong and intensify pain; orlead to higher levels ofsuffering and alteredperception of pain. If identified, shift to “tell meabout your life.”SOURCE: Pain Catastrophizing Scale 2009 Dr. Michael JL SullivanMapi Research Trust, Lyon, France. Internet: https://eprovide.mapi-trust.org19 CO*RE 2020
CHAPTER 2TERMINOLOGY20 CO*RE 2020
WORDS MATTER: LANGUAGE CHOICE CAN REDUCE STIGMA“If you want to care for something, you call it a flower; if you want to killsomething, you call it a weed.”―Don CoyhisCommonly Used TermPreferred TermAddictionSubstance use disorder (SUD)[from the DSM-5 ]Drug-seeking,aberrant/problematic behaviorUsing medication not asprescribedAddictPerson with substance usedisorder (SUD)Clean/dirty urinePositive/negative urine drugscreenSOURCES: SAMHSHA Resource: sources/sud-stigma-tool.pdfScholten W. Public Health. 2017;153:147-153. DOI: 10.1016/j.puhe.2017.08.02121 CO*RE 2020
WORDS MATTER: DEFINITIONSMisuseUse of a medication in a way other than the way it is prescribedAbuseUse of a substance with the intent of getting highToleranceIncreased dosage needed to produce a specific effectDependenceState in which an organism only functions normally in the presence of asubstanceDiversionTransfer of a legally controlled substance, prescribed to one person, toanother person for illicit (forbidden by law) useWithdrawalOccurrence of uncomfortable symptoms or physiological changes causedby an abrupt discontinuation or dosage decrease of a pharmacologicagentMMEMorphine milligram equivalents; a standard opioid dose value based onmorphine and its potency; allows for ease of comparison and riskevaluationsChronic noncancer pain(CNCP)Any painful condition that persists for 3 months, or past the time ofnormal tissue healing, that is not associated with a cancer diagnosisSOURCES: SAMHSHA Resource: sources/sud-stigma-tool.pdfWorld Health Organization, Ensuring Balance in National Policies on Controlled lity safety/GLs Ens Balance NOCP Col EN sanend.pdf22 CO*RE 2020
CHAPTER 3ASSESSMENT23 CO*RE 2020
HOW IS PAIN RESOLVED?24 CO*RE 2020
PAIN ASSESSMENTDESCRIPTION OF ns/patterns/rhythmsWHAT RELIEVES THE PAIN?What relieves the pain?WHAT CAUSES OR INCREASES THE PAIN?EFFECTS OF PAIN ON PHYSICAL, EMOTIONAL AND PSYCHOSOCIAL FUNCTIONPATIENT’S CURRENT LEVEL OF PAIN AND FUNCTIONSOURCES: Heapy A, Kerns RD. Psychological and behavioral assessment. In: Raj's Practical Management of Pain. 4th ed. 2008:279-295;Zacharoff KL, et al. Managing Chronic Pain with Opioids in Primary Care. 2nd ed. Newton, MA: Inflexion, Inc.;2010.25 CO*RE 2020
PAST MEDICAL AND TREATMENT HISTORYNONPHARMACOLOGIC STRATEGIES AND EFFECTIVENESSPHARMACOLOGIC STRATEGIES AND EFFECTIVENESSRELEVANT ILLNESSESPAST AND CURRENT OPIOID USE Query your state’s Prescription Drug Monitoring Program(PDMP) to confirm patient report Contact past providers and obtain prior medical records For opioids currently prescribed, note the opioid, dose, regimen,and duration Determine whether the patient is opioid-tolerantGENERAL EFFECTIVENESS OF CURRENT PRESCRIPTIONS26 CO*RE 2020
PRESCRIPTION DRUG MONITORING PROGRAMS (PDMPs)PDMPs are state-run, electronic databases that track controlledsubstance prescriptions in a state.PDMP DATABASES Provide a full accounting ofthe controlled substanceprescriptions filled by apatient Nearly all are availableonline 24/7 Required in most states;know your state lawsBENEFITS Identify potential drug misuse/abuse Discover existing prescriptions notreported Opportunity to discuss with patient Determine if patient is using multipleprescribers/pharmacies Identify drugs that increase overdoserisk when taken together (such asbenzodiazepines and opioids)* Multiple prescriptions from different providers is most predictive of opioid abuse or misuse.27 CO*RE 2020
OBTAIN A COMPLETE SOCIAL AND PSYCHOLOGICAL HISTORYSOCIAL HISTORYEmployment, cultural background, social network, relationship history, legalhistory, and other behavioral patternsPSYCHOLOGICAL HISTORYScreen for:28 Mental health diagnoses, depression,anxiety, PTSD, current treatments Alcohol, tobacco, and recreational drug use History of adverse childhood experiences Family history of substance use disorder andpsychiatric disorders Depression and anxiety can be predictors ofchronic pain CO*RE 2020
PHYSICAL EXAM AND ASSESSMENTSeek objective dataGeneral: vital signs,appearance, and painbehaviorsNeurologic examConduct physicalexam and evaluatefor painMusculoskeletal exam Inspection Gait and posture Range of motion Palpation Percussion Auscultation ProvocativemaneuversOrder diagnostictests (appropriate tocomplaint)Cutaneous ortrophic findingsSOURCES: Lalani I, Argoff CE. History and Physical Examination of the Pain Patient. In: Raj's Practical Management of Pain.4th ed. 2008:177-188; Chou R, et al. J Pain. 2009;10:113-130.29 CO*RE 2020
PAIN ASSESSMENT TOOL n Assessment ToolsBPI or 5 A’sFunctional AssessmentSF-36, PPS, Geriatric AssessmentPain intensity, Enjoyment of life, General activityPEGAdverse Childhood Experience QuestionnaireACEAssessment in Advanced DementiaPAINADPsychological Measurement Tools (PHQ-9, GAD-7, etc.)30 CO*RE 2020Brief Pain Inventory (BPI)
CHAPTER 4CREATING THE PAINTREATMENT PLAN31 CO*RE 2020
COMPONENTS OF A MULTIMODAL TREATMENT PLAN FOR PAIN32 CO*RE 2019
PAIN MANAGEMENT GOALS AND TREATMENT OPTIONS:A MULTIMODAL APPROACHReduce PainCOGNITIVE BEHAVIORALTHERAPYBehavioral modificationMeditationCognitive TMENTSNerve blocksSteroid injectionsStimulatorsTrigger point injections33 CO*RE 2020SelfcarePHYSICAL TREATMENTSExerciseAcupunctureMovement therapiesManual ulsantsTopicals (e.g., lidocaine)Improve Qualityof Life
EVIDENCE-BASED NONPHARMACOLOGIC TREATMENTSWhat is appropriatefor your patient? Tai Chi Yoga CBT and ACT Acupuncture PT/OT/aquatic Mindfulness meditation OMT Massage therapy Chiropractic Neuromodulation or surgicalapproaches (in some situations)CBT cognitive behavioral therapy; ACT acceptance commitment therapy; OMT osteopathic manipulative therapy34 CO*RE 2020
PHARMACOLOGIC TREATMENTS BY TYPE OF PAINNOCICEPTIVE /INFLAMMATORYNOCIPLASTICIR opioidsNerve blocksNSAIDsTopical / transdermalAnticholinergicAnticonvulsantsTCAs and SNRIsOther serotonin agentsNEUROPATHICAnticonvulsantsIR and ER/LA opioidsNerve blocksTCAs and SNRIsTransdermal opioidsCONTINUE EFFECTIVE NONPHARMACOLOGIC OPTIONS35 CO*RE 2020
POTENTIAL SITES OF ACTION FOR ANALGESIC AGENTSPeripherallyMediated Pain: Acetaminophen NSAIDs Opioids Topical anestheticsCentrallyMediated Pain: Alpha-2 agonists Anticonvulsants Ca channelantagonists NMDA RAs Opioids TCA/SNRIantidepressantsEven though the central nervous system is always involved in pain perception,pain can be mediated peripherally.36 CO*RE 2020
DRUG CHARACTERISTICS TO CONSIDER BEFORE PRESCRIBINGRoute ofadministrationKey instructions(indications, uses,contraindications)FormulationSpecific druginteractionsSpecific information about productconversions, if availableStrengthMOA*Use in opioidtolerant patients*MOA Mechanism of actionOpioid product information available 37 CO*RE 2020Dosing intervalProduct-specificsafety concernsRelativepotency tomorphine
CONSIDER AN OPIOID ONLY WHEN:Potential benefits are likely tooutweigh risksPatient has failed to adequatelyrespond to non-opioid andnonpharmacological interventionsPatient has moderate to severenociceptive or neuropathic painBegin as a therapeutic trialSOURCES: Chou R, et al. J Pain. 2009;10:113-130. Department of Veterans Affairs, Department of Defense.VA/DoD Clinical Practice Guideline for Management of Opioid Therapy for Chronic Pain. 2010.38 CO*RE 2020
OPIOID MISUSE RISK ASSESSMENT OOLS FOR PATIENTS CONSIDERED FOR OPIOID THERAPYORT-OUD Opioid Risk ToolSOAPP Screener and Opioid Assessment for Patients with PainDIRE Diagnosis, Intractability, Risk, and Efficacy scoreTOOLS FOR SUBSTANCE USE DISORDERCAGE-AID Cut down, Annoyed, Guilty, Eye-Opener tool, Adapted to Include DrugsRAFFT Relax, Alone, Friends, Family, TroubleDAST Drug Abuse Screening TestCTQ Childhood Trauma QuestionnaireACEs Adverse Childhood Experiences39 CO*RE 2020
A CLOSER LOOK AT THE ORT-OUDSubstance use disorderhistory does not prohibittreatment with opioids, butmay require additionalmonitoring and expertconsultation or referral.Scoring: 2: low risk 3: high riskSOURCE: Cheatle, M., et al. JPain 2019; Jan 26.40 CO*RE 2020
OPIOID SIDE EFFECTS AND ADVERSE EVENTSSIDE EFFECTSADVERSE EVENTSRespiratory depressionDeathOpioid-induced constipation (OIC)AddictionMyoclonus (twitching or jerking)OverdoseSedation, cognitive impairmentHospitalizationSweating, miosis, urinary retentionDisability or permanent damageAllergic reactionsFalls or fracturesHypogonadismTolerance, physical dependence,hyperalgesiaPrescribers should report serious AEs and medication errors to the FDA:https://www.fda.gov/media/76299/downloador 1-800-FDA-108841 CO*RE 2020
OPIOID-INDUCED RESPIRATORY DEPRESSIONMORE LIKELY TO OCCUR: In elderly, cachectic, or debilitatedpatientsHOW TO REDUCE RISK: Ensure proper dosing and titration Do not overestimate dose when If given concomitantly with otherdrugs that depress respiration (suchas benzodiazepines*) In patients who are opioid-naïve orhave just had a dose increase Opioids are contraindicated inpatients with respiratory depressionor conditions that increase riskconverting dosage from another opioidproduct– Can result in fatal overdose withfirst dose Avoid co-prescribing benzodiazepines* Instruct patients to swallowtablets/capsules whole– Dose from cut, crushed, dissolved, orchewed tablets/capsules may befatal, particularly in opioid-naïveindividuals42 CO*RE 2020*Greatest risk of respiratory depression
TRANSDERMAL/TRANSMUCOSAL DOSAGE FORMSDo not cut, damage, chew, or swallowPrepare skin: clip (notshave) hair and washarea with waterRotate location ofapplicationNote that metal foil backings are notsafe for use in MRIsDo not apply buccal filmproducts if film is cut,damaged, orchanged in any way -- usethe entire filmMonitor patients with fever forsigns or symptoms of increasedopioid exposureNote that exertion or exposure to external heat can lead to fatal overdose43 CO*RE 2020
FOR SAFER USE: KNOW DRUG INTERACTIONS, PHARMACODYNAMICSAND PHARMACOKINETICSCNS depressants can potentiatesedation and respiratory depression(e.g. benzodiazepines)Opioid use with MAOIs may increaserespiratory depression44 Some ER/LA products rapidly releaseopioid (dose dump) whenexposed to alcoholSome drug levels may increasewithout dose dumpingOpioid use can reduce efficacyof diureticsCertain opioids with MAOIs can causeserotonin syndrome (e.g. Tramadol)Inducing release of antidiuretic hormoneMany opioids can prolong QTcinterval, check the PI;methadone requires extra cautionDrugs that inhibit or induce CYPenzymes can increaseor lower blood levels ofsome opioidsCO*RE 2020
OPIOIDS AND CYP450 ENZYME INTERACTIONSMetabolism of several commonly used opioids occurs through thecytochrome P450 systemBe aware of potential inhibitors (e.g., macrolides, azole antifungals) andinducers (e.g., carbamazepine)Genetic and phenotypic variations in patient response to certain opioidsRefer to product-specific information in the drug package insert beforeprescribingSOURCE: https://dailymed.nlm.nih.gov/dailymed/index.cfm45 CO*RE 2020
DRUG INTERACTIONS COMMON TO OPIOIDSOther CNS Depressants Increased risk of respiratorydepression, hypotension,profound sedation, or coma Avoid concurrent use with fullopioid agonist Reduce initial dose May reduce analgesic effectand/or precipitate withdrawalSkeletal Muscle RelaxantsAnticholinergic Medication Concurrent use may enhanceneuromuscular blocking actionand increase respiratorydepression Concurrent use increases riskof urinary retention andsevere constipation*Buprenorphine46 Partial Agonists* or MixedAgonist/Antagonists †CO*RE 2020†pentazocine,nalbuphine, butorphanol May lead to paralytic ileus
SPECIALPOPULATIONS47 CO*RE 2019
OLDER ADULTSRISK FOR RESPIRATORY DEPRESSION Age-related changes in distribution, metabolism,excretion; absorption less affectedACTIONS Monitor Initiation and titration Concomitant medications (polypharmacy) Falls risk, cognitive change, psychosocial status Reduce starting dose to 1/3 to 1/2 the usual dosage in debilitated,non-opioid-tolerant patients Start low, go slow, but GO Routinely initiate a bowel regimen Patient and caregiver reliability/risk of diversionSOURCE: American Geriatrics Society Panel on the Pharmacological Management of Persistent Pain in OlderPersons. J Am Geriatr Soc. 2009;57:1331-46. Chou R, et al. J Pain. 2009;10:113-30.48 CO*RE 2020
WOMEN OF CHILDBEARING POTENTIALNeonatal opioid withdrawal syndrome is a potential risk of opioid therapyGIVEN THIS POTENTIAL RISK, CLINICIANS SHOULD: Discuss family planning, contraceptives, breast feeding plans with patients Counsel women of childbearing potential about risks and benefits of opioidtherapy during p
KAISER PERMANENTE David Bazzo, MD Carol Havens, MD UC SAN DIEGO PHILADELPHIA COLLEGE OF OSTEOPATHIC MEDICINE Katherine Galluzzi, DO KINDRED AT HOME Ron Crossno, MD MOUNT SINAI BETH ISRAEL Edwin Salsitz, MD PRACTICE CONSULTANT . NMDA RAs Opioids TCA/SNRI antidepressants