Transcription
Pulmonary Nodules: When toworry, when to ‘chill’Douglas ArenbergAssociate ProfessorPulmonary & Critical Care
Disclosure MDCH Grant Funds to improvetobacco cessation service in theMichigan Medicine Health System Past paid serviceConsultant/Advisory panel memberfor Nucleix, a company developinglung cancer biomarkers I will not be discussing any specificproducts or medications relevant toeither of these financial relationships
Objectives Recognize features of the patientand the nodule that predict alikelihood of malignancy Understand the indications for(and limitations of) lung nodulebiopsy
Let’s start with an exercise Each of the nextfew slides has twonodules found onCT scans There are somedifferencesbetween thenodules Select which oneyou think is morelikely to bemalignant (A or B),and (in your head)think of one or twowords why youchose your answer
Which of these is more likelymalignant?AB
Which of these is more likelymalignant?AB
Which of these is more likelymalignant? 65 year old manA 32 year old manB
Which of these is more likelymalignant? 65 year old heavysmokerA 64 year old nonsmokerB
What features did you use to guess whichone was more likely to be cancer? Features about the nodule?– Size– Edge characteristics? Features about the patient?– Age– Social history
n-calculatorSwensen et al. Archives of Internal Medicine 1997; 157:849-855.Google “Swensen SPN calculator”
Approach to the patient with anoduleYounger ageSmallSmooth bordersFat or calciumNon-smokerLower lobeNegative PETOlder ageLargeSpiculatedbordersHeavy smokerUpper lobeFDG-avid on PETDefinitelyBenignLow ityHighprobability
What do we do with this“probability”?FleischnerZonePET scan zone“Is this more orless likely to becancer?DefinitelyBenignLow probabilityPET scan zone“This is cancer.What stage hprobability
PET scan:Correlates anatomic and metabolic data 95% sensitivity formalignancyFalse negativesGround glassSmall lesions ( 8-10mesions close to thediaphragmFDG-PETFalse (15-20%)ANYTHINGinflammatoryDon’t get PET inpatients with recentsymptoms ofinfection
A case scenario63 yo former smokerotherwise healthy with a 3.5cm RML mass.what wouldyou do next?A.Biopsy the massB.PET scanC.Refer for surgicalresectionD.MediastinoscopyE.Trick question take ahistory
63 yo former smokerotherwise healthy with a 3.5cm RML mass.what wouldyou do next?E. Trick question takea historyHe presented withabrupt onset chestpain, fever,diaphoresis andproductive coughHow soon would you repeat the CT?
You’ve determined a pre-testprobability of lung cancerNow what?Goal:DefinitelyBenignLow probability 5-15% or lessYounger ageSmallSmooth bordersFat or calciumNon-smokerLower lobeNegative PETOlder ageLargeSpiculated bordersHeavy smokerUpper lobeFDG-avid on HighProbability 60%
You’ve determined a pre-testprobability of lung cancerNow what?Proof of benign:Take it outTime (radiographicobservation)Proof of Malignancy:Any tissue under themicroscope (Biopsy orresection)Goal:DefinitelyBenignLow probability 5-15% or yHighProbability 60%
#1. ANY TIME YOU NEED TO PROVE ITSCANCERCorollary: Biopsy cannot prove you don’t have cacer.Absence of evidence is not evidence of absenceWHEN IS BIOPSYINDICATED?
When is it appropriate to biopsy apatient with a lung nodule? Biopsy is of no use in patients with a high risk ofcancer who are good surgical candidates For this group, the “biopsy” is a surgical procedure Biopsy people who need a diagnosis to facilitatetreatment Medically or anatomically unresectable Make sure biopsy yields an unequivocal stage Suspicion of Small cell lung cancer or metastasis
When do we biopsy?What is a biopsy?Surgical “biopsy”
Don’t let this happen to you FEV1 2.40 (73% of predicted), FVC 3.88 (93% of predicted)DLCO 14.5 (72% of predicted)
What is wrong with this picture?
What do we do with this “probability”?Is there a single answer?Biomarkers with highNPVBenign imagingfeaturesSafersurgery/Betteroutcomes?High patient anxiety,safer biopsytechniques, PositivePETSerial CTObservationHigher surgical riskor poorer outcomesDiagnostic testing (PET) or biopsySurgery orinvasive staging
When to chill? When there is evidenceof benignity** Characteristics ofbenign nodules– CT is more sensitive fordetection of Ca – Detection of fat suggestsa benign cause– Important for nonradiologists to recallpatterns that are NOTpredictive of benignbehavior**How to you pronounce this?
How do you prove a nodule is benign?What tools do we have? Calcium or fat Time Cold hard steel
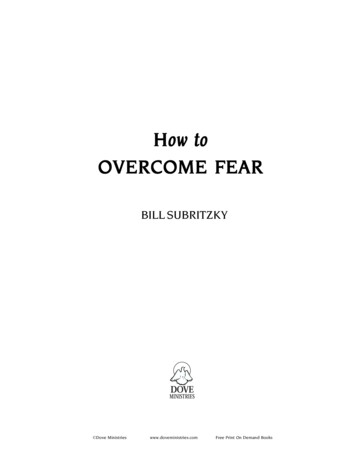
Characteristics of benign nodules:Perifissural nodulesde Hoop B et al. Radiology 2012;265:611-616Pulmonary Perifissural Nodules on CT Scans: Rapid GrowthNot a Predictorof Malignancy. 2012Isby RadiologicalSociety of North America
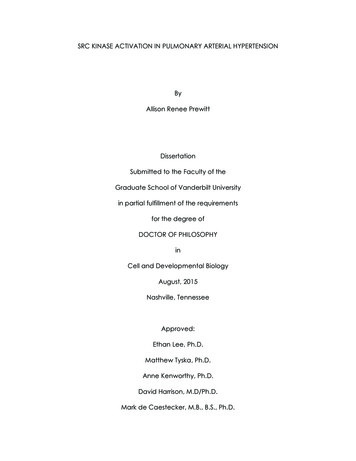
Not all GGOs arecreated equallyHow good are we atidentifying solidcomponents?How long shouldthese be followed?20062010Journal of Thoracic Oncology 2013 8, 309-314
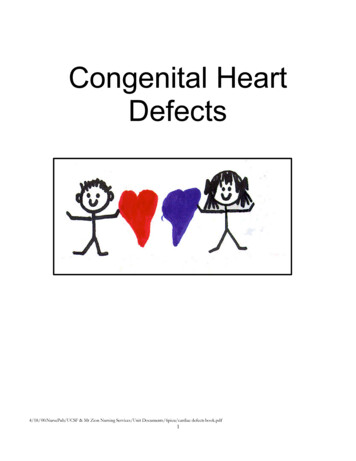
How Long Should Small Lung Lesions of Ground-Glass Opacitybe Followed?108 total non-solidlesions from 61subjects followed for amedian period of 4.2years82 of the followedlesions were recordedas “pure GGO”Of these 82, 18 grewduring observationJournal of Thoracic Oncology 2013 8, 309-314
‘Disarming’ language Nodules are common The VAST majority, even in peopleat very high risk for cancer, arebenign “Lung freckles” Patient education materials
/resources/lung-nodules-online.pdf
Take Home Points Nodule and patient features can be used toestimate the probability of malignancy This probability can determine the next step(s) Long term follow up, PET scan, Surgery,etc., The PET scan has a very high NPV in the rightscenario Benign features of nodules should allowconservative management
When is it appropriate to biopsy a patient with a lung nodule? Biopsy is of no use in patients with a high risk of cancer who are good surgical candidates For this group, the "biopsy" is a surgical procedure Biopsy people who need a diagnosis to facilitate treatment Medically or anatomically unresectable Make sure biopsy yields an unequivocal stage