Transcription
4/18/2018DISCLOSURE (AND DISCLAIMER)PEDIATRIC PULMONARYHYPERTENSIONPHARMACOTHERAPY I have no conflicts of interests to disclose Unless otherwise noted, all medications to be discussed are off-label11th International Conference Neonatal & Childhood Pulmonary Vascular Disease ・April 19, 2018Angelica J. Ng, PharmD, BCPS, BCPPSPediatric Clinical PharmacistUCSF Benioff Children’s Hospital2UCSF BENIOFF CHILDREN’SHOSPITALOVERVIEW Brief overview of pulmonary hypertension as a disease state Pharmacologic management of pulmonary hypertension – targetedtherapies Pharmacotherapeutic considerations in the perioperativemanagement of pediatric pulmonary hypertension Pediatric Pulmonary Hypertension Pharmacotherapy183-bed quaternary care teaching hospital- 24 pediatric cardiac ICU/ TCU beds, 32 PICU/TCU beds and 58NICU beds- Medication safety and regulatory considerations3Pediatric Pulmonary Hypertension Pharmacotherapy 4Nationally ranked in pediatric cardiology and pulmonology (US News& World ReportPediatric Pulmonary Hypertension Pharmacotherapy1
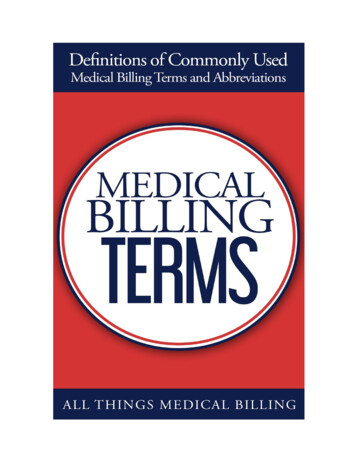
4/18/2018UCSF PEDIATRIC PULMONARYHYPERTENSION PROGRAMPULMONARY HYPERTENSION Established 2011 1st PHA-Accredited Pediatric Center for Comprehensive Care on thewest coastDefined as an increase in mean pulmonary arterial pressure 25mmHg at rest as assessed by right heart catheterization Pediatrics: 149 – 200 patients being actively managed- Same definition, (slightly) different etiologies- Most commonly associated diagnoses: congenital heart disease,congenital diaphragmatic hernia, idiopathic, bronchopulmonarydysplasia- Catch-22: worse outcomes if left untreated but lack of data forpediatric-specific therapeutic strategies 20 – 29 patients on IV/SQ prostacyclin s/ucsf/. Accessed March 29, 20185Pediatric Pulmonary Hypertension Pharmacotherapy6GOALS OF THERAPYselective pulmonaryvasodilation, restoration ofnormal endothelial function, andreversal of remodeling of thepulmonary vasculaturePediatric Pulmonary Hypertension PharmacotherapyFDA APPROVAL TIMELINEreduce right ventricular afterloadand prevent right (Flolan )Bosentan(Traceleer )Treprostinil(Remoudlin )Iloprost(Ventavis )Sildenafil(Revatio )20072008LetairisEpoprostenol(Ambrisentan )(Veletri )20092012Treprostinil(Tyvaso )Sildenafilsuspension(Revatio )Tadalafil(Adcirca )Ultimately, improved survival and allowance of normal activities of childhoodwithout the need to self-limit7Pediatric Pulmonary Hypertension Pharmacotherapy2013Treprostinil(Orenitram )Riociguat(Adempas )2015Selexipag(Uptravi )2017Bosentan tabletfor oralsuspension(Tracleer )Macitentan(Opsumit )8Pediatric Pulmonary Hypertension Pharmacotherapy2
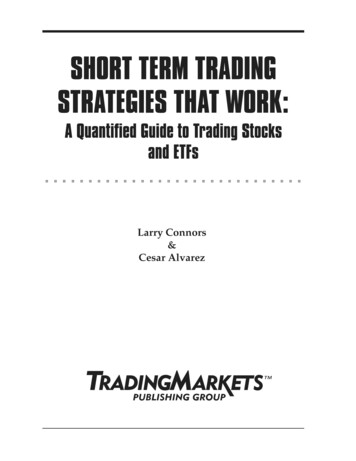
4/18/2018ENDOTHELIAL PATHWAYSENDOTHELIN -hypertension-Three-main fig1 49646627. Accessed March 26, 20189Pediatric Pulmonary Hypertension Pharmacotherapy10ENDOTHELIN PATHWAYENDOTHELIN RECEPTORANTAGONISTSEndothelin 1 is a potent vasoconstrictor- ET-1 ETA vasoconstriction Endothelin Receptor Antagonists- Bosentan (Tracleer ) – non-selective- Ambrisentan (Letairis ) – selective for ETA- Macitentan (Opsumit ) – non-selective Biology of ET-1 and ET receptors is complex- Is “selectivity” better? Pediatric Pulmonary Hypertension PharmacotherapyBosentan (Tracleer )Ambrisentan(Letairis )Macitentan(Opsumit )FDA approved 2017Phase III trialsuspended*Phase III trial recruitingTwice dailyOnce dailyOnce dailyTeratogenicYesYesYesREMS programYesYesYesAdverse EffectsAnemiaElevated LFTsEdema / -Pediatric Data or FDAApprovalDosing FrequencyET-1 – Endothelin 1ETA – Endothelin Receptor AETB – Endothelin Receptor B11Pediatric Pulmonary Hypertension Pharmacotherapy*as of March 30, 201812Pediatric Pulmonary Hypertension Pharmacotherapy3
4/18/2018REMSBOSENTANRisk Evaluation and Mitigation StrategyFDA requirement for manufacturers; ensures that benefit of amedication outweigh its risks Provider must be enrolled in REMS program; restricted distribution In a nutshell: BosentanAmbrisentan, MacitentanPatient enrollmentMale and female patients enrolledFemale patients enrolledLiver ToxicityCounsel patients on risk of liver toxicityLFTs on initiation then monthlyN/ATeratogenicity13THE BASICS Counsel on teratogenicityPregnancy test before initiation and monthly thereafter (and 1 month afterdiscontinuation); yearly pregnancy status updatePediatric Pulmonary Hypertension Pharmacotherapy14BOSENTAN Dosing is no longer straightforward! Historically (UCSF Practice):DOSING - Initial: 1 mg/kg/dose BID, maintenance: 2 mg/kg/dose BID Pediatric Pulmonary Hypertension PharmacotherapyBOSENTANDOSING Non-selective endothelin receptor antagonistAdministration: oral/enteralPharmacokinetic and pharmacodynamic considerations:- Bioavailability: 50%- Metabolism: Hepatically via CYP2C9 and CYP3A4 (active metabolite)- Drug Interactions: Induces CYP2C9 (weak) and CYP3A4 (moderate)Adverse Reactions: hepatic dysfunction, anemia, edemaAccess: only available through specialty pharmaciesFUTURE-1 study: Bosentan plasma concentrations achieved inchildren are lower than those in adults (even at 4 mg/kg/dose BID)FUTURE-3 study: can dose Bosentan up to three times dailyNew labeling:Initial (4 weeks)MaintenancePatients 12 years of age and 40 kg62.5 mg twice daily125 mg twice dailyPatients 12 years of age and 40 kg62.5 mg twice daily62.5 mg twice dailyPatients 12 years of age 4-8 kg 8-16 kg 16-24 kg 24-40 kg16 mg twice daily32 mg twice daily48 mg twice daily64 mg twice daily16 mg twice daily32 mg twice daily48 mg twice daily64 mg twice dailyhttp://www.tracleer.com/assets/PDFs/Tracleer Full Prescribing Information.pdf. Accessed March 27, 2018.15Pediatric Pulmonary Hypertension Pharmacotherapy16Pediatric Pulmonary Hypertension Pharmacotherapy4
4/18/2018BOSENTANBOSENTANDOSAGE FORMS & MED SAFETYDOSAGE FORMS & MED SAFETYLack of pediatric-friendly dosage form until very very recently!Conundrum:”hazardous” medication that needsto be compounded AND needs to beprovided by a specialty pharmacy cannot prescribe as a suspension(since outpatient pharmacy onlyable to provide tablets) To split or not to split tablets? Patient education sheet developed byUCSF Pediatric Pulmonary HypertensionProgram Required constant vigilance at transitionsof care to make sure correctdose/instructions an-625-mg-ml-oral-suspension. Accessed March 27, 2018.17Pediatric Pulmonary Hypertension Pharmacotherapy18BOSENTANPediatric Pulmonary Hypertension PharmacotherapyBOSENTANDOSAGE FORMS & MED SAFETYDOSAGE FORMS & MED SAFETYTablet for oralsuspensionaccompaniedpediatric labelingSeptember 2017Availability of 32 mg soluble tablet and dosing recommendations basedon age and weight categories promote “cleaner” inpatient orders andoutpatient prescriptions (so far )http://www.tracleer.com/px/about-tracleer. Accessed March 27, 2018.19Pediatric Pulmonary Hypertension Pharmacotherapy20Pediatric Pulmonary Hypertension Pharmacotherapy5
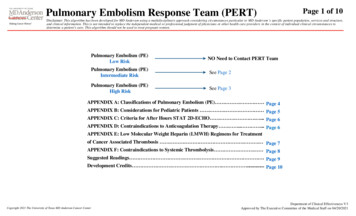
4/18/2018NITRIC OXIDE-cGMP PATHWAYNITRIC OXIDE-cGMPPATHWAYSoluble GuanylateCyclase Stimulator Increasing cGMP production stimulatesvasodilation and antiproliferation Achieved by:- Stimulating cGMP production (inhaled NO,SGC stimulator)- Preventing cGMP breakdown by PDE-5(PDE-5 Inhibitors)NO – Nitric OxidePDE – PhosphodiesteraseSGC – Soluble Guanylate Cyclase21Pediatric Pulmonary Hypertension Pharmacotherapy22NITRIC OXIDE-cGMP MEDICATIONSSildenafil (Revatio )Tadalafil (Adcirca )Riociguat (Adempas )ClassPDE-5 InhibitorPDE-5 InhibitorSGC stimulatorPediatric Data or FDAApprovalPhase III trialscompletedPhase III trials inprogressPhase III trial inprogressThree times daily(usually)Once dailyN/Aheadache, nausea,myalgia, nasalcongestion, flushingheadache, nausea,myalgia, nasalcongestion, flushingDosing FrequencyAdverse Effects23Pediatric Pulmonary Hypertension PharmacotherapyPediatric Pulmonary Hypertension PharmacotherapySILDENAFILTHE BASICS Phosphodiesterase-5 Inhibitor Administration: oral/enteral (IV in some cases) Pharmacokinetic and pharmacodynamic considerations:- Bioavailability: 40% (tablets and suspension are bioequivalent)- Metabolism: Hepatically via CYP2C9 and CYP3A4N/A- Drug Interactions: weak inhibitor of CYP2C9; major substrate ofCYP3A4 (remember bosentan?)24Pediatric Pulmonary Hypertension Pharmacotherapy6
4/18/2018SILDENAFILSILDENAFILTHE BASICS 25DOSINGAdverse Reactions: Not straightforward either!- headache, nausea, myalgia, nasal congestion, flushing Generally: 1 mg/kg/dose TID- Hypotension? Reflux? Vision changes? Titrate based on “tolerability” (ex. decrease to 0.75 mg/kg/dose Q6H)Access: available through community pharmacies Children and adolescents 18 years oldPediatric Pulmonary Hypertension Pharmacotherapy26WeightDose8 to 20 kg10 mg three times daily 20 kg to 45 kg20 mg three times daily 45 kg40 mg three times dailyPediatric Pulmonary Hypertension Pharmacotherapy“SILDENAFILSTARTS-1 AND STARTS-2 TRIALS“In summary, although children randomized to [high sildenafil] had anunexplained increased mortality compared to [lower sildenafil], multipleanalyses raised uncertainty about the survival/dose relationship; all dosegroups displayed favorable survival for children with PAH. STARTS-1efficacy results and the long-term survival rates favor use of lowersildenafil doses.”Barst RJ et alon behalf of the STARTS-2 investigators27Pediatric Pulmonary Hypertension Pharmacotherapy28Pediatric Pulmonary Hypertension Pharmacotherapy7
4/18/2018SILDENAFILSILDENAFILSTARTS-1 AND STARTS-2 – THE FALLOUTDOSAGE FORMS & MED SAFETY (& ECONOMICS)Discard 60 daysafter reconstitutionAugust 2012October 2012March 2014Generic Sildenafil tablets 25 mg (30): 1,993.91( 2.60/mg)29Pediatric Pulmonary Hypertension Pharmacotherapy30TADALAFILPhosphodiesterase-5 Inhibitor Administration: oral/enteral Pharmacokinetic and pharmacodynamics considerations:THE BASICS - Metabolism: Hepatically via CYP3A4Pediatric Pulmonary Hypertension PharmacotherapyAdverse Reactions:- headache, nausea, myalgia,nasal congestion, flushing- Half-life: 15 – 17.5 hours31Pediatric Pulmonary Hypertension PharmacotherapyTADALAFILTHE BASICS 10 mg/mL (112 mL): 9,883.76 ( 8/mg)32 Access: available throughcommunity pharmacies Dosing: 1 mg/kg/dose once dailyTadalafil tablets 20 mg (60): 4,809.60 ( 4/mg)Pediatric Pulmonary Hypertension Pharmacotherapy8
4/18/2018PROSTACYCLIN PATHWAY ProstacyclinreceptoragonistPROSTACYCLIN PATHWAYEndogenous prostacyclin synthesized fromarachidonic acid increased cAMP vasodilation (but also inhibits platelet activityand smooth muscle cell growth)PROSTACYCLIN THERAPYPROSTACYCLIN tric Pulmonary Hypertension Pharmacotherapy34PROSTACYCLIN MEDICATIONSClassPediatric Dataor ric Pulmonary Hypertension PharmacotherapyINHALED PROSTACYCLINSEpoprostenol(Flolan , Veletri )Treprostinil(Remodulin ,Tyvaso ,Orenitram )Iloprost(Ventavis )Selexipag(Uptravi linanalogueProstayclin IPReceptor nce forinhaled/parenteralroutesPhase II trial for POClinicaldata/experienceMinimal clinicaldata/experienceIV (inhaled?)IV, SQ, inhaled, POInhaledPOPediatric Pulmonary Hypertension CLINRECEPTORAGONIST36Pediatric Pulmonary Hypertension Pharmacotherapy9
4/18/2018EPOPROSTENOLEPOPROSTENOLFLOLAN , VELETRI – THE BASICSFLOLAN , VELETRI – THE BASICS Synthetic prostacyclin Initiate at 2 ng/kg/min and titrate upwards as tolerated Administration: continuous IV infusion (requires central access) Pharmacokinetic and pharmacodynamic considerations:Dose-limiting side effects: nausea, diarrhea, vomiting, hypotension,headache, jaw pain Access: only available through specialty pharmacies- Metabolism: rapidly hydrolyzed- Half-life: 6 mins abrupt withdrawal or sudden large dosereductions can cause severe rebound pulmonary hypertension;possible death37Pediatric Pulmonary Hypertension Pharmacotherapy38EPOPROSTENOLTREPROSTINILFLOLAN , VELETRI – LOGISTICS39Pediatric Pulmonary Hypertension PharmacotherapyREMODULIN – THE BASICS Central access increased risk of infection Synthetic prostacyclin analogue Flolan only stable for 8 hours at room temperature (needs ice packsfor 24-hour administration) Administration: IV, SQ Pharmacokinetic and pharmacodynamic considerations: Flolan only compatible with Flolan -specific diluent- Metabolism: hepatically via CYP2C8 Veletri is room-temperature stable but limited data in pediatrics- Half-life: 4 hours Very short half-life need back ups of everything! (i.e. medication, IVaccess, pump and associated supplies)Pediatric Pulmonary Hypertension Pharmacotherapy40Pediatric Pulmonary Hypertension Pharmacotherapy10
4/18/2018TREPROSTINILTREPROSTINILREMODULIN – THE BASICSREMODULIN – LOGISTICS Initial infusion rates vary (typically 1.25 ng/kg/min); pediatric patientsmay require higher starting rates (2-4 ng/kg/min) Titrate upwards as tolerated Longer half-life ( 4 hours) and room-temperature stable- No back-up cassette/cartridge- Does not have to be refrigerated or hung with ice packs- Dose-limiting side effects similar to epoprostenol Flexibility of IV or SQ administrationAccess: only available through specialty pharmacies Benefits of SQ administration- Less risk of infection- May change cartridges as infrequently as Q72hours41Pediatric Pulmonary Hypertension Pharmacotherapy42PARENTERAL PROSTACYCLINSPARENTERAL PROSTACYCLINSUCSF PRACTICE Pediatric Pulmonary Hypertension PharmacotherapyUCSF PRACTICEPrimarily use SQ Remodulin - ”Soft max” rate of 0.03 mL/hr43Pediatric Pulmonary Hypertension Pharmacotherapy Patients transitioned to hospitalsupplied pump and medication Requires use of order set; orderingprivileg
5 Pediatric Pulmonary Hypertension Pharmacotherapy UCSF PEDIATRIC PULMONARY HYPERTENSION PROGRAM Established 2011 1st PHA-Accredited Pediatric Center for Comprehensive Care on the west coast 149 – 200 patients being actively managed - Most commonly associated diagnoses: congenital heart disease, congenital diaphragmatic hernia, idiopathic, bronchopulmonary