Transcription
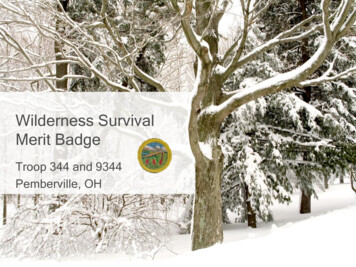
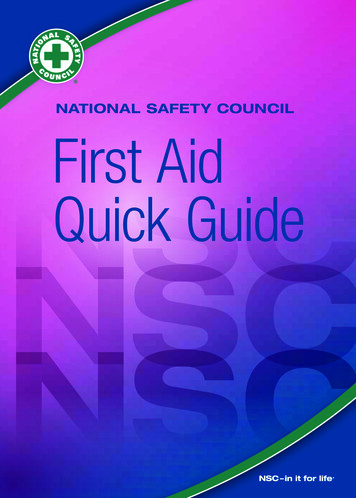
Wilderness First AidReference CardsPulse/Pressure PointsCarotidBrachialPrepared by:Andrea Andraschko, W-EMTOctober 2006RadialFemoralPosteriorTibialAbdominal Quadrants(Looking at Patient)RIGHT UPPER:ANTERIOR:GALL BLADDERLIVERLEFT UPPER:ANTERIOR:STOMACHSPLEENPOSTERIOR:R. KIDNEYPOSTERIOR:PANCREASL. KIDNEYRIGHT ss in a quadrant suggests potentialinjury to the organ indicated in the chart.DorsalisPedisAirway Anatomy
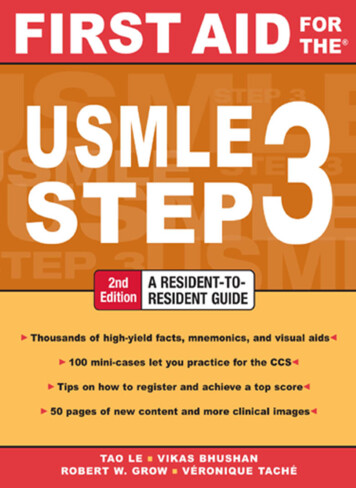
Patient Assessment SystemScene Size-upMOI Major trauma Environmental MedicalSafety/Danger Move/rescue patient Body substance isolation Remove from heat/cold exposure Consider safety of rescuersResources # Patients # Trained rescuers Available equipment (incl. Pt’s)BLSRespiratory Air in and out AdequateNervous AVPU Protect spine/C-collarCirculatory Pulse Check for and Stop Severe BleedingSTOP THINK:A – Continue with detailed examVPU– EVAC NOWPatient Level of Consciousness (LOC)Reliable Pt:CalmCooperativeSoberAlertCauses of Abnormal icityAltitudeToxinsAVPUA Awake and CooperativeA- Awake and lethargic or combativeV Responds with sound to verbalstimuliV- Obeys simple commands with verbalstimuliP Pulls away from source of painP-Moves toward source of painU Totally unresponsiveSOAP Note Information (Focused Exam)Pt. InformationMOIEnvironmental conditionsPosition pt. foundInitial Px: ABCs, AVPUInitial TxSAMPLESymptomsAllergiesMedicationsPast/pertinent HxLast oral intakeEvent leading to incidentPhysical (head to toe) exam: DCAP-BTLS,OPQRSTNormal VitalsPulse: 60-90Respiration: 12-20, easySkin: Pink, warm, dryLOC: alert and orientedPossible Px: Trauma, Environmental, MedicalCurrent PxAnticipated PxField TxS/Sx to monitorEvac levelShock AssessmentHypovolemic – Low fluid (Tank)Cardiogenic – heart problem (Pump)Vascular – vessel problem (Hose)Volume Shock (VS) early/compensated pulse Pale skin respiration rate Normal AVPUVolume Shock late/decompensated pulse Pale skin respiration rate AVPUComment:If a pulse drops but does not returnto ‘normal’ (60-90 bpm) within 5-25minutes, an elevated pulse is likelycaused by VS and not ASR.Tx: Stop visable bleeding, elevate legs,keep warm, manage psychologicalfactors, ventilate if respirations areinadequate, give O2 and IV fluids ifavailable and appropriately trained.
Acute Stress ReactionSympathetic (fight or flight) pulse Pale skin respiration rate Normal AVPU Pain masking Looks like early VS(neumonic SASR Spin up)Parasympathetic (rest and digest) pulse Pale skin respiration rate May feel light headed, dizzy,nauseous, faint, anxious(neumonic PASR passout)Tx: For either condition, calm patient and remove stressors as much as possibleHead InjuriesConcussion:Patient must be awake, cooperative,improving, and have amnesia.S/Sx Patient is awake now Amnesia Can’t have S/Sx of ICP Nausea/vomiting (once) 2 toP-ASR Headache TiredWound CleaningSpine Ruling Out Process (WFR or WEMT)Patient must: Be reliable Report no pain when focused onspine Report no tenderness when spinepalpated Have normal motor exam Have normal sensory exam Report no shooting, tingling orelectric “pain” radiating fromextremitiesMotor Exam: Compare strength in bothhands and feet. Have pt. resist: finger squeeze; pushing down onhand push ‘gas pedal’; pull up on footSensory Exam: compare pt’s ability todistinguish between pin prick and softtouch on back of hand and shin Use pin to prick Use cloth for soft touchIn cases where the spine can’t be ruled out but the injury can be localized to thelumbar area, consult medical direction regarding need to continue c-spinestabilization. ICP:S/Sx – early Patient is A- or lower C/O headache Persistent vomiting AtaxiaS/Sx – late Patient is VPU Vomiting persists Seizure Coma Cardiac and respiratory arrestPartial thickness: Soap and water wash Scrub to remove particles 10% P.I. Keep moist Dress lightlyFull thickness, low to moderate risk: Clean w/in 2 hours of bleeding end Clean around area with 10% P.I. Pressure flush with drinkable water inshort bursts along axis Bring edges toward(not touching) eachother and hold in place with an occlusivedressing and/or steri-strips etc.Full thickness, high risk:Clean as previous, PLUS: Remove dead skin and tissue Remove foreign material Finish flushing process with 1% P.I.solution (strong tea or amber beer) Do not close in field Pack with thin layers of gauzesoaked in 1% P.I. Remove andrepack bid Dress with several layers of gauze.May place 10% P.I. between layers,but not directly on wound Consider splinting if wound is over ajoint.
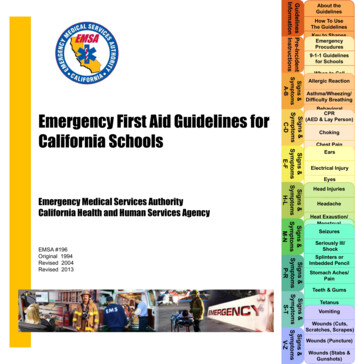
Common Causes of Pulse ChangesStrong, Slow: Normal sleep Simple fainting Early ICP Well-conditioned athlete HypothyroidWeak, slow: Hypothermia Late ICPStrong, fast: Early heat stroke Fever Hyperthyroid Early shock ASR Strenuous physical activityWeak, fast: Overwhelming infection Late heat stroke Late shock Diabetic coma Some types of heart diseaseIrregular: Sinus arrhythmia Heart diseaseHypothermia98.6 to 90 :Pt will be A to A-, shivering, have urine output, coordination anddexterity 90 :Pt will be V, P or U; shivering will stop;HR and respirations will decrease; Ptmay appear deadTx:Active rewarming – give food (carbsfirst), liquids, remove from elements,exercise, shelter, layers, add externalheat (heat packs or hot water bottles)Tx:Passive rewarming – add insulatinglayers (hypowrap), handle with care,no rapid warming or movement, no CPR(AED may be used). PPVs may begiven.Focused Survey AcronymsFrom Patient:Observed by Rescuer:SAMPLE Signs/Symptoms,CMS Circulation, Motion,Allergies, Medications,Previous Injury, Last Meal/Drink,EventsPt PatientHx HistoryPx ProblemS/Sx Signs/SymptomsTx TreatmentSensationOPQRST Onset, Provocation,Quality (dull, sharp), Radiation,Severity (1-10), TimeDCAP-BTLS Deformities,Contusions, Abrasions,Punctures/Penetrations,Burns/Bleeding, Tenderness,Lacerations, SwellingHeat Related SymptomsIf heat is identified as a potential MOIand patient exhibits irrational behavior:Heat exhaustion:A-(irritable), temp. 99 -104 , pale1) ALWAYS COOL PATIENT FIRST2) Assess hydration status If dehydration is established,hydrate with electrolyte solution If hx includes copious H2O, giveelectrolytes only3) Complete focused survey4) Treat symptoms as indicated bysurvey; continue to support coolingmechanismsHeat stroke (early):A- (irritable, combative), temp. 105 ,pale if dehydrated, flushed if hydratedHeat stroke (late):V,P or U, seizures, coma, deathElectrolyte Sickness:A-, V, P or U; Hx of H2O but no food;can rapidly progress to ICP
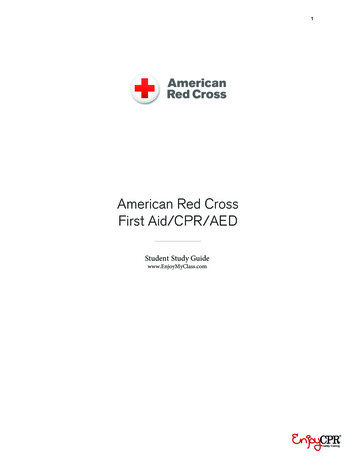
Patient SOAP NoteName:Patient ene Size-Up:Past relevant medical Hx relate to MOIRescuer:Major TraumaFemaleLast food & fluids intake & outputDate:H2OCalorieElectrolyteTime:Urine colorUrine outputStoolPhone:Events Patient’s description of what happenedEnvironmentalAmnesia Yes / NoMedicalDescribe MOIDescribe Environmental ConditionsObjective Information What you seePosition Patient FoundR / L sideInitial PxFront / backLaying / Sitting / StandingA V P U on arrivalNo respirationsNo pulseUnstable spineSevere BleedingVomitingBlocked AirwayPhysical Exam look for discoloration, swelling, abnormal fluid loss & deformity. Feel fortenderness, crepitus & instability. Check ROM and CSM.TimeInitial TxSubjective Information What the patient tells youSymptoms Describe onset, cause & severity (1-10) of chief complaintsTimeAllergies Local or systemic, cause, severity & TxVital Signs get a baseline, then record changesTimePulseRespBPMedications Rx, OTC, herbal, homeopathic & recreationalDrugReasonDoseCurrentYes / NoYes / NoNotesSkinTempAVPU
Assessment What you think is wrongPossible PxTraumaUP ICP / ConcussionTimeCurrent PxAnticipated PxPlan what you are going to doField TxRespiratory DistressVolume ShockUnstable SpineTrunk InjuryUnstable Extremity InjuryStable Extremity InjuryWoundsEnvironmentalDehydration / Low NaHypothermia / ColdHeat Stroke / ExhaustionFrostbite / BurnsLocal / Systemic ToxinLocal / Systemic AllergyNear DrowningAcute Mountain SicknessLightning InjuriesSCUBA / Free DivingMedical inaryMusculoskeletalSkin / Soft TissueEars/Eyes/Nose/ThroatTeeth / GumsEvacuationLevel 1 2 3 4GPS / Grid CoordinatesRequest ALS: Yes / NoMonitor
Additional NotesAdditional vitalsTimePulseRespBPRadio ReportSkinTempAVPUBase, this is withI have a year old male/female whose chief complaint is:as a result of:Patient is currently A V P U and was found Laying/Sitting/Standingon R/L/Front/Back side. Patient exam revealedSpinal assessment revealedPatient statesInitial vitals were: HR: RR: Skin: BP:Current vitals are: HR: RR: Skin: BP:Treatments given are:Anticipated problems during transport are:Evacuation priority is: 1 2 3 4We require: Litter / More People / Helicopter / ALS /Our evacuation plan isOur GPS coordinates are:LZ GPS coordinates are:
Wilderness First Aid Reference Cards Prepared by: Andrea Andraschko, W-EMT October 2006 Abdominal Quadrants (Looking at Patient) RIGHT UPPER: ANTERIOR: GALL BLADDER LIVER POSTERIOR: R. KIDNEY . RIGHT LOWER: ANTERIOR: APPENDIX . LEFT UPPER: ANTERIOR: STOMACH