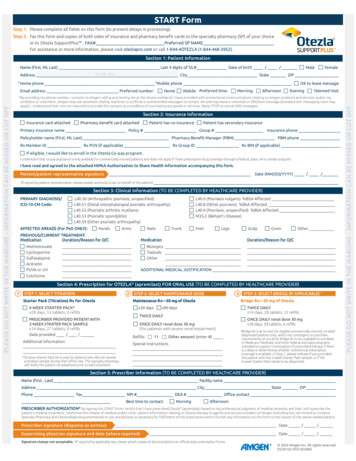
Transcription
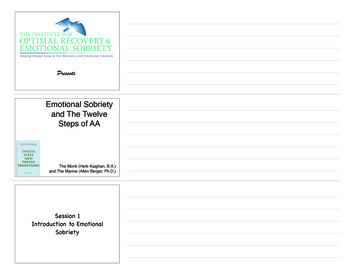
START FormSTART FormStep 1. Please complete all fields on this form (to prevent delays in p 2.1. TFormStepthiscompleteform andallcopiesbothand pharmacybenefit cardsto the specialty pharmacy (SP)Step 1.StepStep 2.1.Step 2.Step 2.Pleasecompleteallfields onthis formof(toprevent delaysin completeform andinsuranceand tyspecialtypharmacypharmacy(SP)(SP)of your choice. preventofyourchoiceor m (todelaysin ybenefit cardsSPtoNAMEthe specialty pharmacy (SP)FAXPreferred SP NAMEor to#OtezlaSupportPlus . FAX# PreferredFax thisform and copies of both sides ofTMinsuranceandbenefit cards to the specialty pharmacy (SP)FAX#SP pharmacyNAME or.Preferredofchoice ororto l 1-844-4OTEZLA(1-844-468-3952).TM visit.of yourchoice o.comorcall1-844-4OTEZLA(1-844-468-3952).FAX # Preferred SP NAMESection1: Patient InformationFor assistance or more information, please visit otezlapro.comorPatientcall For assistance or more information, please visit otezlapro.com or call 1-844-4OTEZLA (1-844-468-3952).Name (First, MI, Last) Last 4 digits of SS # Date of birth / /MaleFemaleSection 1: Patient InformationName (First, MI, Last)4 digits ofSS # Date of birth / /MaleFemaleSectionLast1: PatientInformationNo P.O. BoxAddressCityState ZIPName (First,MI, Last)Last 4 digitsof SS #Date of birth//MaleFemaleNo P.O. BoxAddressCityStateZIPName (First,Last)Last 4phonedigitsof SS #Date of birth//Female* Home*MobilephoneMI,OKMaleto leave messageNo P.O. BoxAddressCity State ZIPNo P.O. BoxHomephoneMobile phoneOK to leave messageAddressCityState ZIPInsurance card attachedPharmacy benefit card attachedPatient has no insurancePatient has secondary insuranceSection2: InsuranceInformationInsurance card attachedPharmacy benefit card attachedPatientno insurancePatient has secondary insurance2:hasInsuranceInformationPrimary insurance name Policy #SectionGroup # Insurance phoneInsurancecard attachedPharmacy benefit card attachedPatient has no insurance GroupPatienthas secondary insurance Insurance phonePrimaryinsurancenamePolicy##Insurancenamecard attachedPharmacybenefit card attachedPatient has First, MI, Last)PharmacyBenefitPatientManagerPBM phonePrimary insurancenamePolicy , Last)Pharmacy licy #Group#InsuranceRxMemberIDRx PCN (if applicable)Rx Group IDRx BIN (if BenefitManager(PBM)PBMphoneRxMember IDRx PCN (if applicable) PharmacyRx Group BenefitIDRx BIN (if applicable)Policyholder(First,Manager (PBM)PBMphoneIf eligible,nameI wouldlikeMI,to Last)enrollin the Otezla Co-pay program.Rx able)If eligible,Iwouldlike ssistanceonly availableforOtezlacommerciallyinsuredpatients and does not apply ifRxI haveprescriptiondrug coverage through a federal,state,or similar program.MemberIDco-payRx(ifapplicable)GroupIDRx BIN(if forOtezlacommerciallyinsuredpatientsand doesnot applyif I have prescriptiondrug coverageIf eligible,I wouldlikein theCo-payprogram.II understandhavereadthatandagreedto totheattachedHIPAAAuthorizationto ShareHealthInformationaccompanyingthis throughform. a federal, state, VA or similar program.If eligible, I would like to enroll in the Otezla Co-pay program.co-payassistanceis onlyavailableHIPAAfor commerciallyinsured patientsand doesnot applyif I have prescriptiondrug coverageI understandhave readthatandagreedto theattachedAuthorizationto ShareHealthInformationaccompanyingthis throughform. a federal, state, VA or similar program.I understand that co-payassistance is only availablefor commerciallyinsured patients and does not apply if I have prescription drug coverage through a federal, state,VA orsimilar program. / YYYY)I have read and agreed to the attached HIPAA Authorization to Share Health Information accompanying this form.representativesignatureDate (MM/DD/YYYY) / /IPatient/patienthave read and agreedto the attachedHIPAA Authorizationto Share Health Information accompanying this form.(If signed by patient representative, please explain authority to act on behalf of the patient)Patient/patient representative signature Date (MM/DD/YYYY) / /(If signed by patient representative,please explainauthority to act on behalf of the patient)Patient/patientrepresentativesignatureDate (MM/DD/YYYY) / /Section3: Clinical Information (TO BE COMPLETED BY HEALTHCARE PROVIDER)(If signed by patient representative, please explain authority to act on behalf of the patient)Section3:actClinicalInformation(TO BE COMPLETED BY HEALTHCARE plainauthoritytoonbehalfofthepatient)PRIMARY DIAGNOSIS/L40.50 (Arthropathic psoriasis, unspecified)L40.0 (Psoriasis vulgaris) %BSA AffectedSection 3:psoriasis,Clinical unspecified)Information (TO BE COMPLETEDBY(PsoriasisHEALTHCAREPROVIDER)PRIMARY DIAGNOSIS/L40.50 .8psoriasis)AffectedSection3: ClinicalpsoriaticInformation(TO BE 40.8(Otherpsoriasis)%BSAAffectedPRIMARY DIAGNOSIS/L40.50 (Psoriatic(Arthropathicpsoriasis,unspecified)L40.0 RY DIAGNOSIS/L40.50 (Arthropathic psoriasis, unspecified)L40.0 (Psoriasis vulgaris) %BSA AffectedL40.52arthritis mutilans)L40.9unspecified)AffectedICD-10-CM Code:L40.51 (Psoriatic(Distal interphalangealpsoriatic arthropathy)L40.8 (Psoriasis,(Otherpsoriasis)%BSA ease)ICD-10-CM Code:L40.51 (Distal interphalangeal psoriatic arthropathy)L40.8 (Other psoriasis) %BSA ��s unspecified)Disease)L40.52 (Otherarthritismutilans)L40.9 (Psoriasis,%BSA AffectedL40.59psoriaticarthropathy)L40.52 (Psoriatic arthritis mutilans)L40.9 (Psoriasis, unspecified) %BSA ylitis)M35.2 (Behçet’sDisease)AFFECTED AREA(S) (For PsO GroinOtherL40.53 (Psoriatic spondylitis)M35.2 (Behçet’s Disease)psoriatic arthropathy)AFFECTED AREA(S) (ForPsO GroinOtherPREVIOUS/CURRENTTREATMENT:L40.59 (Other psoriatic ionDuration/ReasonAFFECTED AREA(S) (ForPsO ONLY):HandsArmsNailsTrunkFeetLegsScalpGroinfor D/C OtherPREVIOUS/CURRENTTREATMENT:AFFECTED AREA(S) (ForPsO ONLY):HandsArmsNailsTrunkFeetLegsScalpGroinfor D/C on/Reason for D/CMedicationDuration/Reason for tionDuration/Reason for D/CMedicationDuration/Reason for AcitretinSulfasalazineOtherPUVAor UVADDITIONALMEDICAL JUSTIFICATIONSulfasalazineOtherPUVAor UVADDITIONALMEDICAL JUSTIFICATIONAcitretinColchicineAcitretinPUVA or UVADDITIONAL MEDICAL JUSTIFICATIONColchicine PUVA or UVADDITIONALMEDICALFORORALJUSTIFICATIONUSE (TO BE COMPLETEDBY HEALTHCARE PROVIDER)Section4: Prescription for OTEZLA (apremilast)Colchicine Section4: Prescription for OTEZLA (apremilast) FOR ORAL USE (TO BE COMPLETED BY HEALTHCARE PROVIDER)Colchicine2 STEP2: SELECT MAINTENANCE DOSE3: SELECT BRIDGE (IF APPLICABLE)†1 STEP 1: SELECT TITRATION(apremilast)FOR ORAL USE (TO BE COMPLETED3 BYSTEPHEALTHCAREPROVIDER)Section 4: Prescription for OTEZLA 2STEP EPSELECT(IF R)1 Starter(Titration) Rx for OtezlaMaintenance Rx—30 mg of OtezlaBridge 3:Rx—30mgBRIDGEof Otezla2 MaintenanceSTEP 1:PackSELECTTITRATIONSTEP 2: SELECTMAINTENANCEDOSESTEP 3:SELECTBRIDGE(IF APPLICABLE)†3 Bridge1 AILY BRIDGE (IF APPLICABLE)†2 STEP1: SELECTTITRATIONSELECTx90MAINTENANCEDOSE3: SELECT3 STEP1 STEPStarterPack(Titration)for OtezlaMaintenancemg of OtezlaBridgeRx—30of Otezlax28 days,55tablets,0 Rxrefillsx14days,28 mgtablets,12 refills4-WEEKSTARTERPACK*x30 days Rx—30x90 daysTWICEDAILYStarter Pack (Titration) Rx for OtezlaMaintenanceRx—30 mg of OtezlaBridge Rx—30 mg of OtezlaTWICE DAILYx28 days,STARTER55 tablets,0 refillsx14days,28 tablets,12 refills4-WEEKPACK*x30 daysx90 daysTWICEDAILYPRESCRIBERPROVIDEDPATIENT WITHONCEDAILYrenaldose30 mgTWICEDAILY days4-WEEKSTARTERPACK*x30daysTWICEDAILYx28 days,STARTER55 tablets,0 refillsx14days,28 0renal dose 30 mgx28days,28612refillsPRESCRIBERPROVIDEDPATIENT WITHONCEDAILYrenal dose30 fillsTWICEDAILYx14days,STARTER27 tablets,0 enalseveredose 30mgimpairment)x2828costtablets,6 refills†TWICEDAILYwithPRESCRIBERPROVIDEDPATIENT WITHONCErenaldose30 mgBridgeRxdays,is DAILYat nofor eligiblecommerciallyinsured, on-labelx14days,27 xdays,ispatientsat noforandeligibleinsured,on-labelRefills:11 renalOtheramount(enter #)requirementsofanykind.BridgeRxisnotavailableto 28days,28tablets,6refillsDateprovided/0/x14 days,27 tablets,refills(For patients with severe renal impairment)diagnosed patients only, and is not contingent on irment)x14 days,27 tablets, 0 refillsSpecial instructions†requirements of any kind. Bridge Rx is not available to enrolleesBridgeRxtoispatientsatno costforandeligiblecommerciallyinsured,on-labelDate provided/ /diagnosedonly,is ntprescribedtherapyif thereAdditionalinformationin Medicare,Medicaid,and otherfederaland stateprogramsRefills: instructions11Other amount (enter #)SpecialDate provided / /diagnosedpatientsonly,andis notcontingenton lprescriptionintended to support continuation of prescribed therapy if there11Other amount (enter #)Refills:Additional informationrequirementsof any kind.BridgeRxis caid,otherfederalstateprogramscoverageis available.InandStep1, pleaseif ,Medicaid,and other federalandstate*AdditionalTitration StarterPack Rx is only for patients who did not ckprescribedthepatientwiththe 2-weeksample,orprogramsifprovidedtheif thereSpecial instructionscoverageisIn StepStarter1, portcontinuationof prescribedtherapy if therea titrationsampleduringvisit. Thespecialtyis a acktoStarterbe dispensed.*TitrationStarterPackRx istheironlyofficefor patientswhodid notpharmacyreceivethepatientwiththeneeds2-weekPack sample,or if ionwillnotify thepatientvia theirtelephoneeachshipment.coverageis available.In Stepindicate if you providedatitrationsampleduringofficepriorvisit. toThespecialtypharmacy4-weekStarterPack needsto1,bepleasedispensed.coverageis available.In StepStarter1, pleaseindicateif you*TitrationStarterPack Rxonly for patientsnot receivethe patientwith the 2-weekPacksample,or ifprovidedthewill notifythe patientviaistelephoneprior towhoeachdidshipment.*TitrationStarterPackRx istheironlyofficefor patientswhodid notpharmacyreceivethepatientwithPackthe needs2-weektoStarterPack sample, or if thea titrationsampleduringvisit. ThespecialtyStarterbe dispensed.Section5: PrescriberInformation (TO BE COMPLETED BY HEALTHCARE t. toThespecialtypharmacy4-week Starter Pack needs to be dispensed.notify samplethe patientvia theirtelephoneeachshipment.Section5: PrescriberInformation (TO BE COMPLETED BY HEALTHCARE PROVIDER)will notifythe, Last)patient viatelephone prior to eachshipment.Name(FirstFacility nameSection5:PrescriberInformation (TO BE COMPLETEDBY HEALTHCAREPROVIDER)Name (First, Last)FacilitynameSection 5: Prescriber Information (TO BE COMPLETEDBY HEALTHCAREPROVIDER) State ityState ZIPPhoneFax NPI # DEA #Office contactName (First, Last)Facility nameAddressCityState ZIPPhoneFax BestNPI #DEA#Office contacttimetocontact:MorningAfternoonAddress City State ZIPPhoneFaxNPI#DEA#OfficecontactBest time to oneFax NPI # DEA # Office contactBysigning this STARTForm I certify that I have prescribed Otezla (apremilast)professional judgmentof medical necessityand that I will supervise the patient’s medical treatment. I authorize the release ofBest basedtime onto Bestandtimeto mycontact:MorningAfternoonmedicaland/orother patientinformationrelatingto Otezlatherapyto agentsserviceprovidersof Amgen(includingbut notlimitedto CovancePharmacyand Otezla-dispensingpharmacies)and of Bysigningthis STARTForm I certifythat I ljudgmentof medicalnecessityandthat I willSpecialtysupervisethe patient’smedical treatment.I authorize totheusereleasePRESCRIBERAUTHORIZATION*discloseas necessaryforfulfillmentof therelatingprescriptionand tofurnishtoanyinformationon thisform tooftheinsurerof the above-named patient. (including but not limited to Covance Specialty Pharmacy and Otezla-dispensing pharmacies) to use andmedical and/orotherpatientinformationto thisOtezlatherapyprovidersAmgenBy signingSTARTIagentscertifyandthatserviceI onhaveOtezla(apremilast)on myjudgmentmedicalnecessityand thatI will supervisethe ofPRESCRIBERAUTHORIZATION*By signing this STARTForm I certify that I haveprescribedOtezla entof medicalbasednecessityandprofessionalthat I will supervisetheofpatient’smedicaltreatment.I authorizethe release discloseasmedicalnecessaryforfulfillmentof theprescriptionandto furnishany informationonmythisprofessionalform to hisSTARTFormI certifythatI cessityandthatwillSpecialtysupervisethe patient’smedicaltreatment.I authorizethereleasepatient’streatment.I toofOtezlatherapyto agentsand Iserviceprovidersof Amgen(includingbut relatingto Otezlatherapyto agentsandserviceproviders ofrelatingAmgen (includingbutnotlimitedto CovancePharmacyand Otezla-dispensingpharmacies)useand e//Covancemedicalotherandpatientinformationto ingbut notandlimitedto CovanceSpecialty Pharmacyand Otezla-dispensingpharmacies)to )useandtodiscloseasnecessaryforfulfillmentof thetopatient.furnishany informationon this formto the insurer of theabove-nameddisclose and/orasPharmacynecessaryforfulfillmentof non thisformtooftheinsurerofprescriptionthe above-namedPrescribersignature(dispenseas written)Date / /disclose as necessaryfor fulfillmentof the prescriptionand(whereto furnishany information onthis form to the insurer of the above-named patient.Supervisingphysiciansignatureand daterequired)Date / /Prescriber signature (dispense as written)Date / and date ps not acceptable.*If requiredwritten)by applicable law,please attach copies of all prescriptions on official state prescription quired)Date / ialstateprescriptionforms.Supervising physician signature and date (where required)Date / /Signature stampsnot acceptable. *If requiredFax:by applicablelaw, please attach copies ofPhone:all prescriptionson official state prescription forms.OTEZLASUPPORTPLUS 1-855-850-29551-844-468-3952Signature stamps not acceptable. *If required by applicable law, please attach copies of all prescriptions on official state prescription forms.OTEZLASUPPORTPLUS Fax: 1-855-850-2955 Phone: 1-844-468-3952OTEZLA SUPPORTPLUS Fax: 1-855-850-2955 Phone: 1-844-468-3952OTEZLA SUPPORTPLUS Fax: 1-855-850-2955 Phone: 1-844-468-3952 2019 Amgen Inc. All rights reserved05/202019US-OTZ-20-0605Amgen Inc.Inc. AllAllrightsrightsreserved.reserved 2020Amgen05/20US-OTZ-20-0605US-OTZ-20-0605 2019Amgen Inc. All rights reserved 2019US-OTZ-20-0605Amgen Inc. All rights reserved05/2005/20 IONMISSEDORCUTOFFPLEASEDONOTWRITEINTHEMARGINS- OTWRITEWRITEININTHEMARGINSMARGINS- ONOTNOTWRITEWRITEININTHEMARGINSMARGINS- NCANBEMISSEDMISSEDORCUTOFFMorningtime: AfternoonVisitMobile Preferred time: PreferredEmail address Preferred number:HomeMorning EveningAfternoonTelemedEveningHome phone Mobile phoneOK to leave messageEmailaddressPreferredPreferred time:HomeMorningAfternoonEvening* HomeBy providingmyphonenumber, I consent to Amgen calling and textingme atnumber:the phone Mobilenumber(s)I have Mobileprovided with promotional communicationsrelating to Amgenproducts andservicesand/ormyphonephoneOKto leavemessageSection2:HomeInsuranceconditionor treatment.Amgen may use automatic dialing machinesor artificialor prerecordedmessages Mobileto Informationcontact me and may leave a voicemailor SMS/text(standard textmessaging ratesmayEmail addressPreferrednumber:Preferredtime: edtime:HomeMorningAfternoonEveningapply). I understand that I am not required to provide this consent as a condition of purchasing any goods or services. Reply STOP to cancel SMS messages.
Patient Authorization to Share Health InformationPlease present this Authorization to the patient/patient representative and obtain the required signature.Uses and Disclosure of Personal InformationI authorize Amgen and its contractors and business partners(“Amgen”) to use and/or disclose my personal information,including my personal health information, only for thefollowing purposes: To operate, administer, enroll me in, and/or continue myparticipation in Amgen’s Otezla SupportPlus program orany other Amgen-affiliated patient support services andactivities related to my condition or treatment (for example,co-pay card programs, reimbursement assistance programs,drug coverage verification, nurse educator services,adherence program and disease management support); To contact, with my permission, my doctor and the rest ofmy health care team and share with them my healthinformation that may be useful for my care; To provide me with informational and promotionalmaterials relating to Amgen products and services,and/or my condition or treatment; and/or To improve, develop, and evaluate products, services,materials and programs related to my condition ortreatment.In order for Amgen to provide me with the servicesand/or programs described above, Amgen needs to collectand use my personal information, including my personalhealth information. I understand that my personal healthinformation may include any information, in electronic orphysical form, in the possession of or derived from a healthcare provider, health care plan, pharmacy, pharmaceuticalcompany, laboratory and/or their contractor (“Health CareProvider”). This may include select information from or aboutmy medical history and general health, my health care planbenefits, payment limits or restrictions covered by my healthcare plan policy, and/or my adherence to my treatment.I authorize my Health Care Providers to disclose my personalhealth information to Amgen, and between themselves, asnecessary, but only for the purposes stated above in thisAuthorization. I understand that certain of my Health CareProviders (such as pharmacies and specialty pharmacies)may receive remuneration from Amgen in exchange fordisclosing my personal health information and/or for usingmy information to contact me with communications aboutAmgen products which have been prescribed to me (forexample medication reminder programs) and other patientsupport services.Expiration, Right to Obtain a Copy and Right to CancelI understand that by signing this form, I authorize myHealth Care Providers or others who might hold my healthinformation to only release it to Amgen employees, as wellas to its contractors and business partners, who areperforming the services set forth in this Authorization.I also understand I am authorizing my personal information,including my personal health information, to be used for thepurposes described above. I understand and agree thatby signing below, I am authorizing those who rely on thisAuthorization to release my personal health information forthe earlier of five (5) years or until my participation in theprogram ends through my cancellation, unless a shorter timeperiod is required by state law.I understand that I can obtain a copy of this Authorizationor cancel this Authorization at any time by calling Amgenat 1-844-468-3952 or by writing to PO BOX 13185, La Jolla,California, 92039. If I cancel my consent, I will no longer qualifyfor the services described. I also understand that if a HealthCare Provider is disclosing my personal health information toAmgen on an authorized on-going basis, my cancellation withAmgen will be effective with respect to any such Health CareProviders as soon as they receive notice of my cancellation.No Effect on TreatmentI understand I do not have to sign this Authorization andthat my enrollment in any of the services and/or programsdescribed above is entirely voluntary. I understand thatAmgen, as well as Health Care Providers, cannot require me,as a condition of having access to medications, prescriptiondrugs, treatment or other care, to sign this Authorization.Federal Law (including HIPAA) requires a signed authorizationin order for Amgen to collect this information from my HealthCare Providers. I understand I cannot participate in the listedservices and/or programs without signing this Authorization oran equivalent authorization with my Health Care Providers.Information Received from Health Care ProvidersI understand that once my personal health information hasbeen disclosed to Amgen, federal privacy laws may no longerapply and protect it from further disclosure. Amgen agrees,however, to protect my personal health information by onlyusing and disclosing it as stated in the Authorization or asotherwise allowed or required by law.Authorization to ContactI understand and consent to Amgen contacting me usingthe contact information provided in this form to enroll mein, operate, and administer Amgen patient support servicesand/or programs as described above other than promotionalcommunications by telephone or SMS/text (which I canseparately opt-in below). I understand that the operationand administration of certain of these services and/orprograms may require that Amgen contact me by telephoneor SMS/text.OTEZLA SUPPORTPLUS Fax: 1-855-850-2955 Phone: 1-844-468-3952 2020 Amgen Inc. All rights reserved.05/20 US-OTZ-20-0605
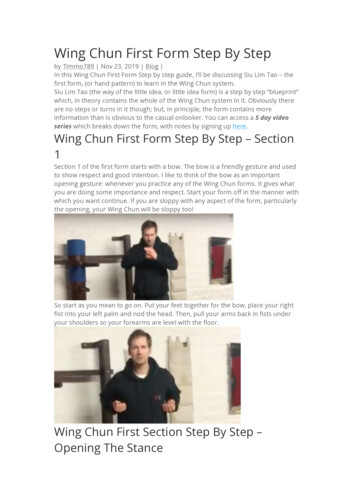
Filling an Otezla prescriptionPRESCRIBEPrescribe Otezla (apremilast) 30-mg tablets for an appropriate patientPREPARE1. Collect patient information, including prescriptionbenefit information2. Select a Specialty Pharmacy (SP) to process the Rxor choose Otezla SupportPlus (OSP) to initiate theprescription processNo StarterPack?Request StarterPack in section 4 ofthe START Form orfrom your OtezlaSales Representative3. Provide Starter Pack, if appropriateSUBMIT1. Complete the Otezla START Form or the SPenrollment form. Send with copies of the medicaland prescription benefit card to the SP or OSPPA is notrequired2. S P or OSP conducts the benefit verification anddetermines if Prior Authorization (PA) is requiredBenefitverification iscomplete.PA isrequiredSubmit PA form along with other requireddocumentation to the insurerPA isapprovedPA isdeniedAPPEALAppeal the denial by submitting the Letter of MedicalNecessity and other required documentation to the insurer.Find this document on OtezlaPro.com, or contact OSP,1-844-4OTEZLA (1-844-468-3952) 8 AM – 8 PM ET,Monday – FridayShouldappeal(s) bedeniedRefer patient to OSP to determine eligibility for thePatient Assistant ProgramAppeal isapprovedSP coordinatesco-pay collectionand direct mailshipment ofmedication tothe patient
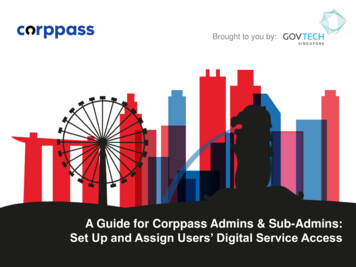
Otezla SupportPlus can help with accessThis support network includes resources for you and your patients.REIMBURSEMENT SUPPORTPATIENT SUPPORT Benefits investigation and PA assistance 24/7 access to specially trained nurses Assessment of patient eligibility forMedicare coverage 0 co-pay* enrollment and follow-up Appeals support for coverage denials Updates on prescription status Specialty pharmacy triage and coordination Shipment of free bridge to maintenance supplyduring potential reimbursement delays forcommercially insured patients Status updates on prescription fulfillment Live insurance supportFinancial assistance optionsCOMMERCIALLY INSUREDOtezla Savings ProgramEligibility requirements: Commercially insured(no Medicare or Medicaid)MEDICARE & MEDICAIDUNINSURED OR UNDERINSUREDIndependent Co-payFoundations &State ProgramsPatient Assistance ProgramEligibility requirements:Eligibility requirements: On-label diagnosis Patient must be a US resident(may vary by foundation): For uninsured or underinsuredpatientsBe sure to remind your patientsthat they may be eligible fora 0 co-pay,* and to ask theirspecialty pharmacy aboutfinancial offers that may beavailable to them. Each fund has its ownenrollment process Patient must be a US resident Patients can receivefunding as needed Patient must meet financialrequirements* Certain restrictions apply. This offer is not valid for persons eligible for reimbursement of this product, in whole or in part, under Medicaid,Medicare, or similar state or federal programs. Offer void where prohibited by law.Questions? Need more information?Call Otezla SupportPlus at 1-844-4OTEZLA (1-844-468-3952)8 AM – 8 PM ET, Monday – Friday
The right information speeds the processAny incorrect or missing information on the START Form can delay the approval process.Did you remember toFax completed and signed Otezla START Formto Otezla SupportPlus (Patient signature is notrequired during a telemedicine visit.)Indicate permission to leave a message withpatientNote the patient’s titration start date if youprovided the Starter Pack directly to your patientInclude copies of both sides of the patient’s(1) prescription benefit card and (2) medicalbenefit cardCheck “Bridge Rx – 30 mg of Otezla (apremilast)”in section 4 of the START FormFax any clinical notes helpful i
*If required by applicable law, please attach copies of all prescriptions on official state prescription forms. OTEZLA SUPPORTPLUS Fax: 1-855-850-2955 Phone: 1-844-468-3952 Starter Pack (Titration) Rx for Otezla 4-WEEK STARTER PACK* x28 days, 55 tablets, 0 refills 4-WEEK STARTER PACK*PRESCRIBER PROVIDED PATIENT WITH 2-WEEK STARTER PACK SAMPLE