Transcription
Advances in Type 2 Diabetes CareNeelima Chu, MD, FACESharp Rees-StealyDepartment of Endocrinology
Objectives Review the pathophysiology of Type 2 Diabetes Understand the goals of diabetes care Review the older diabetes medications Learn the mechanism of action of the newerdiabetes medications (including injectables) Assess the use and safety during inpatientadmission
Pathogenesis of Type 2 Diabetes The environmental risk factors: increased weight gain anddecreased physical activity Three key fundamental defects to the development andprogression of T2DM: impaired insulin secretion from pancreatic β-cells decreased glucose uptake in peripheral tissues increased hepatic glucose production (HGP) Treatment is based on targeting these defects
American Diabetes AssociationsRecommendations Glycosylated hemoglobin: 7.0% Pre-prandial plasma glucose: 90-130mg/dl Postprandial plasma glucose: 180mg/dl
UKPDS Results The overall HbA1c achieved was 0.9% lower in theintensive compared with the conventional (7.0% vs. 7.9%) The difference in glycemic control was associated with areduction in the risk of microvascular complications(retinopathy, nephropathy, neuropathy) A trend toward reduced rates of myocardial infarction
Patient-centered care is defined as an approach to“providing care that is respectful of and responsive toindividual patient preferences, needs, and values andensuring that patients values guide all clinical decisions”
SulfonylureasMeglitinides Most widely used drugs The SFU ( glyburide, glipizide, glimepride) andmeglitinides (Prandin, Starlix) are structurallydifferent but act similarly by increasing insulinsecretion
Metformin Decreases gluconeogenesis Increases insulin-mediated glucose utilization inperipheral tissues (such as muscle and liver)
Thiazolidinediones (TZD)(Actos, Avandia) TZDs bind to and activate peroxisome proliferatoractivated receptors (PPARs) TZDs increase insulin sensitivity by acting onadipose, muscle, and liver to increase glucoseutilization and decrease glucose production
α- Glucosidase Inhibitors(Acarbose, Miglitol) These drugs slow absorption of glucose The main side effects are flatulence anddiarrhea
Bromocriptine (Cycloset) The mechanism of action in reducing blood sugaris unknown Not generally recommended for the treatment oftype 2 diabetes
Colesevelam (Welchol) A bile acid sequestrant Mechanism of action to improve glycemic controlis uncertain Generally not recommended to improve glycemiccontrol
GLP-1 Analogs The incretin hormones GLP-1and GIP are secreted from theintestine in response to meals Slows gastric emptying Inhibits post-meal glucagonrelease and reduces food intake GLP-1 exhibits a short half-lifeof one to two minutes due todegradation by the enzymedipeptidyl peptidase 4 (DPP-4)
GLP-1 AnalogsDaily Exenatide (Byetta) Liraglutide (Victoza)Weekly Exenatide (Bydureon) Albiglutide (Tanzeum) Dulaglutide (Trulicity)
DPP-4 Inhibitors They increase the GLP-1 levels Stimulates the release of insulin Decreases the levels of glucagonin the circulation Can be administered orally No risk of hypoglycemia
DPP-4 Inhibitors Sitagliptin (Januvia) Saxagliptin (Onglyza) Linagliptin (Tradjenta) Alogliptin (Nesina)
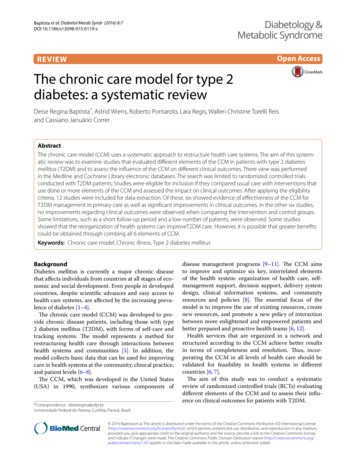
SGLT-2 (Sodium-Glucose Co-Transporter-2)GG GGGG GGGGGGGGGGGGGGGGGGGG90% ReabsorptionLimited ReabsorptionChao and Henry. Nature Rev 9:2010:551-9
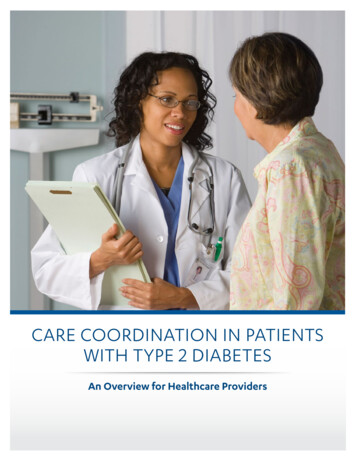
Glucose excretionLower Blood Glucose LevelsGGGGGGGGGGGGGGGGGGGGGGGGGGGSGLT-2 InhibitorGGGGGGGGG
SGLT-2 Inhibitors Canagliflozin ( Invokana) Dapagliflozin (Farxiga) Empagliflozin (Jardiance)
SGLT-2 Inhibitors:Caution and Side Effects SGLT2 inhibitors should not be used in: Type 1 diabetes Type 2 diabetes and eGFR 60 mL/min( dapagliflozin) or 45mL/min (canagliflozin, empagliflozin) Ketosis-prone type 2 diabetes The most common side effects: vulvovaginal candidal infectionsand hypotension, acute kidney injury, urinary tract infections,euglycemic diabetic ketoacidosis
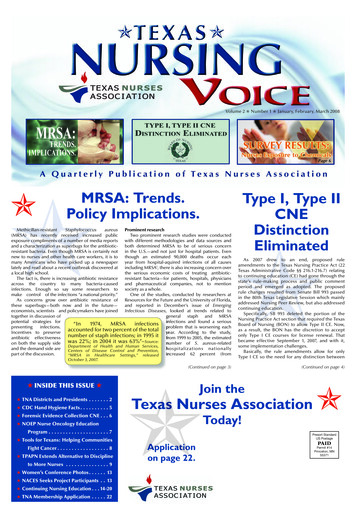
Traditional Insulins And Their Time Course Of ActionPremixed insulin alsoAvailable (70/30, 75/25)InsulinOnsetPeakDurationRapid-acting10-15 mins60-90 mins4-5 hrRegular30-60 mins2-4 hours5-8 hrNPH1-3 hr5-8 hours12-18 hrDetemir90 minsRelativelyPeakless12-24 hrGlargine90 minsPeakless24 hrInsulin LevelsRapid-actingRegular Glargine1800200022002400Lepore M et al. Diabetes. 2000;49:21 42-21 48; Howey DC et al. Diabetes. 1994;43:396-402; Plank J et al. Diabetes Care.2005;28:1107-1112;; Wittlin SD et al. Insulin Therapy. Marcel Dekker, Inc.;2002:73-85.Hours
Newer Insulins Afreeza U 300 Glargine: Tresiba Degludec U 100, U200: Tresiba U 500 Humulin Pen
Afrezza: Rapid Acting Inhaled Insulin Administered at the start of ameal Dissolves immediately uponinhalation Peak insulin levels areachieved within 12 to 15minutes of administration
Dosing Units For Inhaled Insulin
U300 Glargine:Toujeo 3x concentration of Glargine U300 is a new formulation of insulin glargine thatis expected to last up to 40h Lower risk of hypoglycemia Get more insulin with smaller volume More stable levels than Lantus
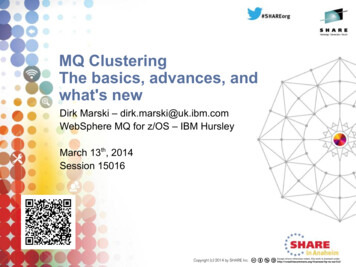
Toujeo (U-300) vs Lantus (U-100)Hours1. Flatter and longer duration of action2. Less peaks and valleys3. Less hypoglycemiaBecker RHA et al. Diabetes Care. 2014; Published ahead of print: doi: 10.2337/dc14-0006
Degludec:Tresiba U100,U200 Onset of action is 2 hours Duration of effect: 40 hours No peak effect Less hypoglycemia
Degludec: Tresiba
Humalog U-200 Kwik Pen Concentrated Humalog, short acting insulin Comes in a pen only 2x concentrated as Humalog 100u/ml You take the same dose but inject less volume andthe pen will last longer
U 500 Humulin Concentrated insulin indicated to improve glycemiccontrol in those requiring more than 200 units ofinsulin per day Comes in a 20 ml Vial or Pen 5x concentrated regular insulin Usually given 2-3 x day
U100, U200, U300, U500Are U confused? U100 100units of insulin/1ml U200 200units of insulin/1ml U300 300units of insulin/1ml U500 500units of insulin/1mlIf you want to give a pt 100unitsU100 100units 1cc 1mlU200 100units 1/2cc 0.5mlU300 100units 1/3cc 0.3mlU500 100units 1/5cc 0.2ml
Why is Volume Important?U300 U500U200U100
Medtronic530G/EnliteDexcomG4 & G5PlatinumContinuous GlucoseMonitoring Devices
EfficacyMedicationChange in A1cSFU1-2%Metformin1.5%Actos0.5-1.4%α Glucosidase 0.5%GLP-1 Analogs0.9-1.9%DPP-4 Inhibitors0.5-1.5%SGLT-2 Inhibitors0.5-0.7%InsulinsUnlimited
Transition into Hospital Insulin is the preferred treatment for glycemiccontrol In certain circumstances, it may be appropriate tocontinue home regimens Diabetes self-management in the hospital may beappropriate for select youth and adult patients Important to keep side effects in mind
Key Points Glycemic targets and therapies must be individualized Diet, exercise, and education remain the foundation ofany type 2 diabetes treatment Combination therapy with 1–2 oral or/and injectableagents is reasonable, aiming to minimize side effectswhere possible All treatment decisions should be made in conjunctionwith the patient, focusing on their preferences, needs,and values
Questions
U100, U200, U300, U500 Are U confused? U100 100units of insulin/1ml U200 200units of insulin/1ml U300 300units of insulin/1ml U500 500units of insulin/1ml If you want to give a pt 100units U100 100units 1cc 1ml U200 100units 1/2cc