Transcription
ASSOCIATION HEALTH PLAN2021 Benefits and Financials
Group Number(s): 59617Rating Period: 8/1/2021 - 7/31/2022Rate Summary for Platinum PlanEmployeeEmployee SpouseEmployee ChildrenFamilyRatefor GoldPlan PlanRateSummarySummaryfor GoldEmployeeEmployee SpouseEmployee ChildrenFamilyRate Summary for Silver PlanEmployeeEmployee SpouseEmployee ChildrenFamilyRate Summary for Bronze PlanEmployeeEmployee SpouseEmployee ChildrenFamilyBCBS MedPlusExpiring Rates 535 1,049 972 1,457Renewal Rates 560 1,120 1,016 1,574BCBS MedplusRenewal Rates 515 1,021 932 1,437Expiring Rates 494 968 895 1,371BCBS MedplusRenewal Rates 490 966 887 1,360Expiring Rates 381 742 688 1,049BCBS-NO Secondary InsuranceRenewal Rates 430 839 778 1,186
Group Number(s): 59617Rating Period: 8/1/2021 - 7/31/2022Rate Summary for Dental ValueEmployeeEmployee SpouseEmployee ChildrenFamilyCurrent Rates 21 38 43 63Renewal RatesCurrent RatesRenewal Rates 23 43 49 72Rate Summary for Dental CompleteEmployeeEmployee SpouseEmployee ChildrenFamily 29 54 62 92 32 61 71 105Rate Summary for VSP VisionEmployeeEmployee SpouseEmployee ChildrenFamilyCurrent Rates 8 12 12 19Renewal Rates 8 12 12 19
Two cards, ONE benefit!Make sure you present both yourBlueCross card and your MedPlus cardwhen using your benefits.Sample BCBS AL CardSample Medplus Card**The sample ID card shown is for illustrative purposes only and does not include valid plan information
MedPlus Claim ProcessDefinition of Terms:EOB Explanation of BenefitsPrimary Insurance *Other*Secondary Insurance Gulf Guaranty MedPlus
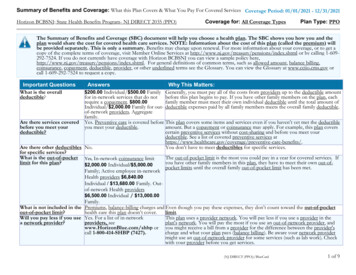
Alabama State BarAssociationPlatinum PlanGroup SupplementalHealth Insurance ProposalEffective Date:8/1/2021Lower Employee Deductibles * Reduce Out of Pocket Exposure * Save Premium Cost
Alabama State Bar Association - Platinum PlanAugust 1, 2021BCBSALMEDPLUSSingle 5000 / Family 10000BCBSAL 60% / Member 40%Single 8550 / Family 17100Single 500 / Family 1000Medplus 100% / Member 0%Single 500 / Family 1000BCBSAL covers 100%BCBSAL covers 100% 5000 CYD then 60% 5000 CYD then 60%MedPlus pays up to 8050MedPlus pays up to 8050Outpatient Facility & Ambulatory Centers 5000 CYD then 60% 5000 CYD then 60%MedPlus pays up to 8050MedPlus pays up to 8050Outpatient Physician (surgery and anesthesia) 5000 CYD then 60%MedPlus pays up to 8050Outpatient Diagnostic 5000 CYD then 60% 5000 CYD then 60% 5000 CYD then 60%MedPlus pays up to 8050MedPlus pays up to 8050MedPlus pays up to 8050BCBSAL covers at 100%Covered under BCBSAL 45 PCP/ 65 SpecialistBCBSAL Excludes 0 ded/ 15/ 60/ 100/ 50% up to 500Covered under BCBSALNo Copay - 24/7 AccessCovered under BCBSALCOMPOSITE SUMMARYDEDUCTIBLES & OUT OF POCKET MAXIMUMCalendar Year Deductible (CYD)Coinsurance after DeductibleOut of Pocket Maximum (OPM) *Cost after Deductible and OPM have been metINPATIENT HOSPITAL FACILITYInpatient HospitalInpatient Hospital Physician ServicesOUTPATIENT FACILITY AND PHYSICIAN CHARGESEmergency Room PhysicianAmbulanceOther Covered Services - PT, Chiro, DMEPHYSICIAN AND RX CO-PAYSPreventative/WellnessPrimary/Specialist Physician CopayTelemedicine: (24 hour Physician Access)Prescription Drug Benefits: Tier 1,2,3,4* The Out of Pocket with Medplus does NOT include Doctor Copays or Pharmacy deductibles or Copays
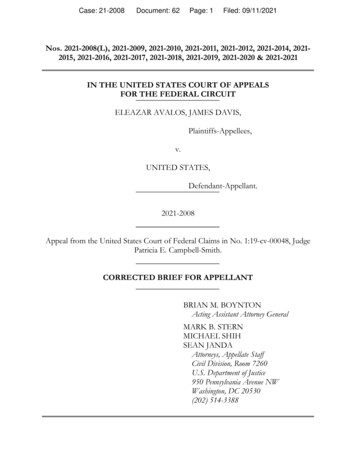
Alabama State BarAssociation - GoldPlanGroup SupplementalHealth InsuranceProposalEffective Date:8/1/2021Lower Employee Deductibles * Reduce Out of Pocket Exposure * Save Premium Cost
Alabama State Bar Association - Gold PlanAugust 1, 2021BCBSALMEDPLUSSingle 5000 / Family 10000BCBSAL 60% / Member 40%Single 8550 / Family 17100Single 2000 / Family 4000Medplus 100% / Member 0%Single 2000 / Family 4000BCBSAL covers 100%BCBSAL covers 100% 5000 CYD then 60% 5000 CYD then 60%MedPlus pays up to 6550MedPlus pays up to 6550Outpatient Facility & Ambulatory Centers 5000 CYD then 60% 5000 CYD then 60%MedPlus pays up to 6550MedPlus pays up to 6550Outpatient Physician (surgery and anesthesia) 5000 CYD then 60%MedPlus pays up to 6550Outpatient Diagnostic 5000 CYD then 60% 5000 CYD then 60% 5000 CYD then 60%MedPlus pays up to 6550MedPlus pays up to 6550MedPlus pays up to 6550BCBSAL covers at 100%Covered under BCBSAL 45 PCP/ 65 SpecialistBCBSAL Excludes 0 ded/ 15/ 60/ 100/ 50% up to 500Covered under BCBSALNo Copay - 24/7 AccessCovered under BCBSALCOMPOSITE SUMMARYDEDUCTIBLES & OUT OF POCKET MAXIMUMCalendar Year Deductible (CYD)Coinsurance after DeductibleOut of Pocket Maximum (OPM) *Cost after Deductible and OPM have been metINPATIENT HOSPITAL FACILITYInpatient HospitalInpatient Hospital Physician ServicesOUTPATIENT FACILITY AND PHYSICIAN CHARGESEmergency Room PhysicianAmbulanceOther Covered Services - PT, Chiro, DMEPHYSICIAN AND RX CO-PAYSPreventative/WellnessPrimary/Specialist Physician CopayTelemedicine: (24 hour Physician Access)Prescription Drug Benefits: Tier 1,2,3,4* The Out of Pocket with Medplus does NOT include Doctor Copays or Pharmacy deductibles or Copays
Alabama State BarAssociation - SilverPlanGroup SupplementalHealth InsuranceProposalEffective Date:8/1/2021Lower Employee Deductibles * Reduce Out of Pocket Exposure * Save Premium Cost
Alabama State Bar Association - Silver PlanAugust 1, 2021BCBSALMEDPLUSSingle 5000 / Family 10000BCBSAL 60% / Member 40%Single 8550 / Family 17100Single 4000 / Family 8000Medplus 100% / Member 0%Single 4000 / Family 8000BCBSAL covers 100%BCBSAL covers 100% 5000 CYD then 60% 5000 CYD then 60%MedPlus pays up to 4550MedPlus pays up to 4550Outpatient Facility & Ambulatory Centers 5000 CYD then 60% 5000 CYD then 60%MedPlus pays up to 4550MedPlus pays up to 4550Outpatient Physician (surgery and anesthesia) 5000 CYD then 60%MedPlus pays up to 4550Outpatient Diagnostic 5000 CYD then 60% 5000 CYD then 60% 5000 CYD then 60%MedPlus pays up to 4550MedPlus pays up to 4550MedPlus pays up to 4550BCBSAL covers at 100%Covered under BCBSAL 45 PCP/ 65 SpecialistBCBSAL Excludes 0 ded/ 15/ 60/ 100/ 50% up to 500Covered under BCBSALNo Copay - 24/7 AccessCovered under BCBSALCOMPOSITE SUMMARYDEDUCTIBLES & OUT OF POCKET MAXIMUMCalendar Year Deductible (CYD)Coinsurance after DeductibleOut of Pocket Maximum (OPM) *Cost after Deductible and OPM have been metINPATIENT HOSPITAL FACILITYInpatient HospitalInpatient Hospital Physician ServicesOUTPATIENT FACILITY AND PHYSICIAN CHARGESEmergency Room PhysicianAmbulanceOther Covered Services - PT, Chiro, DMEPHYSICIAN AND RX CO-PAYSPreventative/WellnessPrimary/Specialist Physician CopayTelemedicine: (24 hour Physician Access)Prescription Drug Benefits: Tier 1,2,3,4* The Out of Pocket with Medplus does NOT include Doctor Copays or Pharmacy deductibles or Copays
PPOPlan BenefitsBronzeBlueCard PPOEffective August 1, 2021Visit our website atAlabamaBlue.comAn Independent Licensee of the Blue Cross and Blue Shield Association
Prescription Drugs: ValueONE NetworkValueONE Network Facts: 41,000 major national and regional pharmacy chains, retailers and grocers, and independentpharmacies participate in the ValueONE Network. This includes many national pharmacies you mayalready be using. Pharmacies that participate in the ValueONE Network can fill up to a 90-day supply of certainmedications at the same location (prescription must be written for up to a 90-day supply). If you do not use a ValueONE Network pharmacy, you may be responsible for the full cost of yourprescription medication. Benefits may not be provided for out-of-network pharmacies. To maximize your pharmacy benefits, you will need to transfer all your prescriptions to a ValueONENetwork Pharmacy.Find a ValueONE Network PharmacyYou can locate all of the participating pharmacies in your area atAlabamaBlue.com/ValueONEPharmacyLocator. To search for pharmacies in your area, enter your ZIP codein the “Location” search field and then click “Search”.Group # 59617 B001
Alabama State Bar AssociationBlueCard PPO – BronzeAugust 1, 2021BENEFITIN-NETWORKOUT-OF-NETWORKBenefit payments are based on the amount of the provider’s charge that Blue Cross and/or Blue Shield plans recognize for payment ofbenefits. The allowed amount may vary depending upon the type provider and where services are received.Calendar Year DeductibleSUMMARY OF COST SHARING PROVISIONS(Includes Mental Health Disorders and Substance Abuse) 5,000 individual; 10,000 family 10,000 individual; 20,000 familyCalendar Year Out-of-Pocket Maximum 8,550 individual; 17,100 familyAll deductibles, copays and coinsurance for innetwork services and all deductibles, copaysand coinsurance for out-of-network mentalhealth disorders and substance abuseemergency services apply to the out-of-pocketmaximum.After you reach your Calendar Year Out-ofPocket Maximum, applicable expenses for youwill be covered at 100% of the allowed amountfor remainder of calendar yearThere is no out-of-pocket maximum forout-of-network services.The in-network and out-of-network calendaryear deductibles are separate and do not applyto each otherINPATIENT HOSPITAL AND PHYSICIAN BENEFITS(Includes Mental Health Disorders and Substance Abuse)Precertification is required for inpatient admissions (except medical emergency services and maternity); notification within 48 hours formedical emergencies. Generally, if precertification is not obtained, no benefits are available. Call 1-800-248-2342 (toll-free) forprecertification.Inpatient HospitalCovered at 60% of the allowed amount,subject to calendar year deductibleCovered at 50% of the allowed amount,subject to calendar year deductibleNote: In Alabama, available only for medicalemergency services and accidental injuryInpatient Physician Visits andConsultationsCovered at 60% of the allowed amount,subject to calendar year deductibleCovered at 50% of the allowed amount,subject to calendar year deductibleMental Health Disorders and SubstanceAbuse Services covered at 50% of theallowed amount, no copay or deductibleOUTPATIENT HOSPITAL BENEFITS(Includes Mental Health Disorders and Substance Abuse)Precertification is required for some outpatient hospital benefits. Precertification is also required for provider-administered drugs; icationDrugList.If precertification is not obtained, no benefits are available.Outpatient Surgery (IncludingAmbulatory Surgical Centers)Covered at 60% of the allowed amount,subject to calendar year deductibleCovered at 50% of the allowed amount,subject to calendar year deductibleIn Alabama, not coveredEmergency Room (Medical Emergency) Covered at 60% of the allowed amount,subject to calendar year deductibleCovered at 60% of the allowed amount,subject to calendar year deductibleMental Health Disorders and SubstanceAbuse Services covered at 60% of theallowed amount, subject to in-networkcalendar year deductibleGroup # 59617 B002
BENEFITIN-NETWORKEmergency Room (Accident)Note: If you have a medical emergency asdefined by the plan after 72 hours of anaccident, refer to Emergency Room (MedicalEmergency) above.Emergency Room (Physician)OUT-OF-NETWORKCovered at 60% of the allowed amount,subject to calendar year deductibleCovered at 60% of the allowed amount,and subject to calendar year deductible forservices rendered within 72 hours; 50% ofthe allowed amount subject to calendaryear deductible when services arerendered after 72 hours of the accidentand not a medical emergency as definedby the planCovered at 60% of the allowed amount,subject to calendar year deductibleCovered at 60% of the allowed amount,subject to calendar year deductibleMental Health Disorders and SubstanceAbuse Services covered at 60% of theallowed amount, subject to in-networkcalendar year deductibleChemotherapy, Dialysis, IV Therapy,Outpatient Diagnostic Lab, Pathology,Radiation Therapy & X-rayCovered at 60% of the allowed amount,subject to calendar year deductibleCovered at 50% of the allowed amount,subject to calendar year deductibleIn Alabama, not coveredIntensive Outpatient Services andCovered at 60% of the allowed amount,Partial Hospitalization for Mental Health subject to calendar year deductibleDisorders and Substance AbuseServicesCovered at 50% of the allowed amount,subject to calendar year deductibleIn Alabama, not coveredPHYSICIAN BENEFITS(Includes Mental Health Disorders and Substance Abuse)Precertification is required for some physician benefits. Precertification is also required for provider-administered drugs; icationDrugList.If precertification is not obtained, no benefits are available.Office Visits and Second SurgicalOpinionsCovered at 100% of the allowed amount,after 45.00 primary care physician copayor 65.00 specialist physician copayCovered at 50% of the allowed amount,subject to calendar year deductibleSurgery & AnesthesiaCovered at 60% of the allowed amount,subject to calendar year deductibleCovered at 50% of the allowed amount,subject to calendar year deductibleMaternity CareCovered at 60% of the allowed amount,subject to calendar year deductibleCovered at 50% of the allowed amount,subject to calendar year deductibleChemotherapy, Diagnostic Lab,Dialysis, IV Therapy, Pathology,Radiation Therapy & X-rayCovered at 60% of the allowed amount,subject to calendar year deductibleCovered at 50% of the allowed amount,subject to calendar year deductibleGroup # 59617 B003
BENEFITApplied Behavioral Analysis (ABA)TherapyIN-NETWORKCovered at 60% of the allowed amount,subject to calendar year deductibleOUT-OF-NETWORKCovered at 50% of the allowed amount,subject to calendar year deductibleLimited to ages 0-18 for autism spectrumdisordersRoutine Immunizations and PreventiveServices PREVENTIVE CARE BENEFITSCovered at 100% of the allowed amount,no copay or deductibleNot CoveredSee AlabamaBlue.com/PreventiveServices r a listing of the specific drugs,immunizations and preventiveservices or call our CustomerService Department for a printedcopyCertain immunizations may also beobtained through the PharmacyVaccine Network. SeeAlabamaBlue.com/VaccineNetworkDrugList for moreinformation.Note: In some cases, office visit copays or facility copays may apply. Blue Cross and Blue Shield of Alabama will process theseclaims as required by Section 1557 of the Affordable Care Act.PRESCRIPTION DRUG BENEFITS(Includes Mental Health Disorders and Substance Abuse)Precertification is required for some drugs; if precertification is not obtained, no benefits are available.Retail Prescription Prepaid BenefitsCovered at 100% of the allowed amount,Not CoveredThe retail pharmacy network for the plan isValueONE Retail Network Locate a ValueONE Retail Networkpharmacy at AlabamaBlue.com/ValueOnePharmacyLocatorMaintenance drugs - up to 90-day supply maybe purchased but copay applies for each 30day supplyPrescription drugs (other than maintenancedrugs) - up to a 30-day supply Some copays combined for diabeticsuppliesView the SourceRx 1.0 drug list that applyto the plan at AlabamaBlue.com/SourceRx1DrugList4Tsubject to the following copays for a 30day supply for each prescriptionTier 1 Drugs: 15 copay per prescriptionTier 2 Drugs: 60 copay per prescriptionTier 3 Drugs: 100 copay per prescriptionTier 4 (specialty) Drugs:50% of the allowed amount up to 500maximumThe only in-network pharmacy for some Tier 4(specialty) drugs is the Pharmacy SelectNetwork Tier 4 (specialty) drugs can be dispensedfor up to a 30-day supplyView the Specialty Drug List tGroup # 59617 B004
BENEFITIN-NETWORKMail Order Pharmacy Benefits Up to a 90-day supply with one copayMail Order Drugs are available throughHome Delivery Network (Enroll online atAlabamaBlue.com/HomeDeliveryNetwork or call 1-800391-1886)Only maintenance drugs can be purchasedthrough this mail order pharmacy service View the maintenance drug list thatapplies to the plan at AlabamaBlue.com/MaintenanceDrugListTier 1 Drugs: 37.50 copay per prescriptionOUT-OF-NETWORKNot CoveredTier 2 Drugs: 150 copay per prescriptionTier 3 Drugs: 250 copay per prescriptionTier 4 (specialty) Drugs:Not coveredView the SourceRx 1.0 drug list thatapplies to the plan at AlabamaBlue.com/SourceRx1DrugList4TBENEFITS FOR OTHER COVERED SERVICES(Includes Mental Health Disorders and Substance Abuse)Precertification is required for some other covered services; please see your benefit booklet. If precertification is not obtained, nobenefits are available.Allergy Testing & TreatmentCovered at 60% of the allowed amount,subject to calendar year deductibleCovered at 50% of the allowed amount,subject to calendar year deductibleAmbulance ServiceCovered at 60% of the allowed amount,subject to calendar year deductibleCovered at 50% of the allowed amount,subject to calendar year deductibleParticipating Chiropractic ServicesCovered at 60% of the allowed amount,subject to calendar year deductibleCovered at 50% of the allowed amount,subject to calendar year deductibleLimited to 15 visits per member per calendaryearIn Alabama, not coveredDurable Medical Equipment (DME)Covered at 60% of the allowed amount,subject to calendar year deductibleCovered at 50% of the allowed amount,subject to calendar year deductibleRehabilitative Occupational, Physicaland Speech TherapyCovered at 60% of the allowed amount,subject to calendar year deductibleCovered at 50% of the allowed amount,subject to calendar year deductibleCovered at 60% of the allowed amount,subject to calendar year deductibleCovered at 50% of the allowed amount,subject to calendar year deductibleOccupational, Physical and SpeechTherapy for Autism SpectrumDisorders ages 0-18Covered at 60% of the allowed amount,subject to calendar year deductibleCovered at 50% of the allowed amount,subject to calendar year deductibleHome Health and HospiceCovered at 60% of the allowed amount,subject to calendar year deductibleCovered at 50% of the allowed amount,subject to calendar year deductibleOccupational, physical and speech therapylimited to combined maximum of 30 visits permember per calendar yearHabilitative Occupational, Physical andSpeech TherapyOccupational, physical and speech therapylimited to combined maximum of 30 visits permember per calendar yearIn Alabama, not coveredGroup # 59617 B005
BENEFITIN-NETWORKOUT-OF-NETWORKHEALTH MANAGEMENT BENEFITS(Includes Mental Health Disorders and Substance Abuse)Individual Case ManagementChronic Condition ManagementBaby Yourself Contraceptive ManagementAir Medical TransportCoordinates care in event of catastrophic or lengthy illness or injury. For more information, pleasecall 1-800-821-7231.Coordinates care for chronic conditions such as asthma, diabetes, coronary artery disease,congestive heart failure, chronic obstructive pulmonary disease and other specialized conditions.A maternity program; For more information, please call 1-800-222-4379. You can also enrollonline at AlabamaBlue.com/BabyYourself.Covers prescription contraceptives, which include: birth control pills, injectables, diaphragms,IUDs and other non-experimental FDA approved contraceptives; subject to applicabledeductibles, copays and coinsuranceAir medical transportation to a network hospital near home if hospitalized while traveling morethan 150 miles from home; to arrange transportation, call AirMed at 1-877-872-8624.Useful Information to Maximize Benefits To maximize your benefits, always use in-network providers for services covered by your health benefit plan. To find in-network providers, check aprovider directory, provider finder website (AlabamaBlue.com) or call 1-800-810-BLUE (2583). In-network hospitals, physicians and other healthcare providers have a contract with a Blue Cross and/or Blue Shield Plan for furnishinghealthcare services at a reduced price (examples: BlueCard PPO, PMD). In-network pharmacies are pharmacies that participate with Blue Crossand Blue Shield of Alabama or its Pharmacy Benefit Manager(s). In Alabama, in-network services provided by mental health disorders andsubstance abuse professionals are available through the Blue Choice Behavioral Health Network. Sometimes an in-network provider may furnish aservice to you that is not covered under the contract between the provider and a Blue Cross and/or Blue Shield Plan. When this happens, benefitsmay be denied or reduced. Please refer to your benefit booklet for the type of provider network that we determine to be an in-network provider fora particular service or supply. Out-of-network providers generally do not contract with Blue Cross and/or Blue Shield Plans. If you use out-of-network providers, you may beresponsible for filing your own claims and paying the difference between the provider’s charge and the allowed amount. The allowed amount maybe based on the negotiated rate payable to in-network providers in the same area or the average charge for care in the area. Please be aware that providers/specialists may be listed in a PPO directory or provider finder website, but not covered under this benefit plan.Please check your benefit booklet for more detailed coverage information. Bariatric Surgery, Gastric Restrictive procedures and complications arising from these procedures are not covered under this plan. Please seeyour benefit booklet for more detail and for a complete listing of all plan exclusions. Please refer to your benefit book or contact Blue Cross directly about coverage for your hospital charges and other related medical services.Approval for air medical services does not mean that hospitalization and other medical expenses will be covered. All coverage determinations formedical benefits are subject to the terms, conditions, limitations and exclusions of the health plan. Air medical transport services are providedthrough a contract with AirMed International, LLC, an independent company that does not provide Blue Cross and Blue Shield of Alabamaproducts. Blue Cross is not responsible for any mistakes, errors or omissions that AirMed, its employees or staff members make. Air medicalservices terminate if coverage by your health plan ends.This is not a contract, benefit booklet or Summary Plan Description. Benefits are subject to the terms, limitations andconditions of the group contract (including your benefit booklet). Check your benefit booklet for more detailed coverageinformation. Please visit our website, AlabamaBlue.com.Group # 59617 B006
Effective August 1,2021
Dental Blue 1500BDental BenefitsGENERAL PROVISIONSCalendar Year DeductibleAnnual Maximum Benefitseach Calendar YearAnnual Maximum BenefitsRollover each Calendar YearRollover Account MaximumLimit 25 deductible per member per calendar year; 75 family maximum. 1,500 per member per calendar year.Plan will allow up to 500 of unused annual maximum dollars to carry over when a membercompletes their diagnostic and preventive service(s) within a calendar year.The rollover amount is 1,000.DIAGNOSTIC AND PREVENTIVE SERVICESCovered at 100%, with no deductible.Includes: Dental exams up to twice per calendar year. Full mouth x-rays, one set during any 36 consecutive months. Bitewing x-rays, up to twice per calendar year. Other dental x-rays, used to diagnose a specific condition. Routine cleanings, twice per calendar year. Tooth sealants on teeth numbers 3, 14, 19, and 30, limited to one application per tooth each 48 months. Benefits arelimited to a maximum payment of 20 per tooth. Limited to the first permanent molars of children through age 13. Fluoride treatment for children through age 18 twice per calendar year. Space maintainers (not made of precious metals) that replace prematurely lost teeth for children through age 18.BASIC RESTORATIVE SERVICESCovered at 100%, subject to deductible.Includes: Fillings made of silver amalgam and synthetic tooth color materials (tooth color materials include composite fillings on thefront upper and lower teeth numbers 5-12 and 21-28; payment allowance for composite fillings used on posterior teeth isreduced to the allowance given on amalgam fillings). Simple tooth extractions. Direct pulp capping, removal of pulp and root canal treatment. Repairs to crowns, inlays, onlays, veneers, fixed partial dentures and removable dentures. Emergency treatment for pain.BASIC SUPPLEMENTAL SERVICESCovered at 100%, subject to deductible.Includes: Oral surgery for tooth extractions and impacted teeth and to treat mouth cysts and abscesses of the intra-oral and extra-oralsoft tissue. General anesthesia given for oral or dental surgery. This means drugs injected or inhaled for relaxation or to lessen pain,or to make unconscious, but not analgesics, drugs given by local infiltration, or nitrous oxide. Treatment of the root tip of the tooth including its removal.MAJOR PROSTHETIC SERVICESCovered at 50%, subject to deductible.Includes: Full or partial dentures. Fixed or removable bridges. Inlays, onlays, veneers or crowns to restore diseased or accidentally broken teeth, if less expensive fillings will not restorethe teeth.Note: No benefits for late enrollee until the member has been covered for a continuous 365-daysMAJOR PERIODONTIC SERVICESCovered at 80%, subject to deductible.Includes: Periodontic exams twice each 12 months. Removal of diseased gum tissue and reconstructing gums. Removal of diseased bone. Reconstruction of gums and mucous membranes by surgery. Removing plaque and calculus below the gum line for periodontal disease.Note: No benefits for late enrollee until the member has been covered for a continuous 365-daysThis is not a contract. Benefits are subject to the terms, limitations and conditions of the group contract.
Dental Blue 1000BDental BenefitsGENERAL PROVISIONSCalendar Year DeductibleAnnual Maximum Benefitseach Calendar YearAnnual Maximum BenefitsRollover each Calendar YearRollover Account MaximumLimit 50 deductible per member per calendar year; 150 family maximum. 1,000 per member per calendar year.Plan will allow up to 500 of unused annual maximum dollars to carry over when a membercompletes their diagnostic and preventive service(s) within a calendar year.The rollover amount is 1,000.DIAGNOSTIC AND PREVENTIVE SERVICESCovered at 100%, with no deductible.Includes: Dental exams up to twice per calendar year. Full mouth x-rays, one set during any 36 consecutive months. Bitewing x-rays, up to twice per calendar year. Other dental x-rays, used to diagnose a specific condition. Routine cleanings, twice per calendar year. Tooth sealants on teeth numbers 3, 14, 19, and 30, limited to one application per tooth each 48 months. Benefits arelimited to a maximum payment of 20 per tooth. Limited to the first permanent molars of children through age 13. Fluoride treatment for children through age 18 twice per calendar year. Space maintainers (not made of precious metals) that replace prematurely lost teeth for children through age 18.BASIC RESTORATIVE SERVICESCovered at 100%, subject to deductible.Includes: Fillings made of silver amalgam and synthetic tooth color materials (tooth color materials include composite fillings on thefront upper and lower teeth numbers 5-12 and 21-28; payment allowance for composite fillings used on posterior teeth isreduced to the allowance given on amalgam fillings). Simple tooth extractions. Direct pulp capping, removal of pulp and root canal treatment. Repairs to crowns, inlays, onlays, veneers, fixed partial dentures and removable dentures. Emergency treatment for pain.BASIC SUPPLEMENTAL SERVICESCovered at 80%, subject to deductible.Includes: Oral surgery for tooth extractions and impacted teeth and to treat mouth cysts and abscesses of the intra-oral and extra-oralsoft tissue. General anesthesia given for oral or dental surgery. This means drugs injected or inhaled for relaxation or to lessen pain,or to make unconscious, but not analgesics, drugs given by local infiltration, or nitrous oxide. Treatment of the root tip of the tooth including its removal.MAJOR PERIODONTIC SERVICESCovered at 80%, subject to deductible.Includes: Periodontic exams twice each 12 months. Removal of diseased gum tissue and reconstructing gums. Removal of diseased bone. Reconstruction of gums and mucous membranes by surgery. Removing plaque and calculus below the gum line for periodontal disease.Note: No benefits for late enrollee until the member has been covered for a continuous 365-daysThis is not a contract. Benefits are subject to the terms, limitations and conditions of the group contract.
Our goal from the start wasto make our health plancompetitive with the smallgroup offerings currentlyavailable from BCBS whileadding stability and value toyour membership.We chose to offer Medical, Dental, and Vision plans from BlueCross BlueShieldof Alabama and VSP to accomplish this goal.Members should find comfort and familiarity in being insured by the largestHealthcare company in Alabama. BlueCross Blue Shield is a undisputed leaderwhile VSP provides the largest network of vision providers in the state.We will offer a multiple option medical strategy, allowing your employees to choosea medical plan that fits their needs and their budget.Dental willhavetwo options for members to choose from. You will find flexibility throughout the offering in order to make our plan your plan!
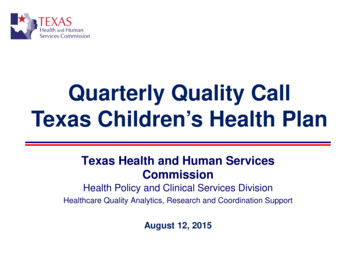
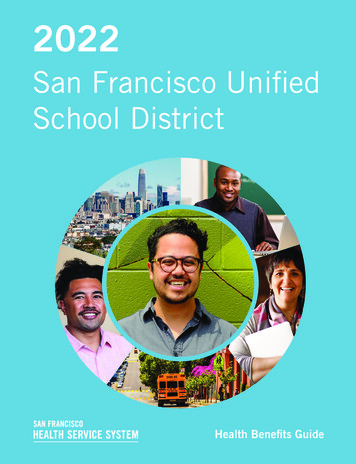
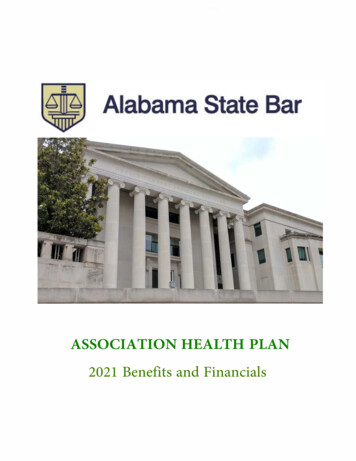
Why Everyone Needs Vision CareVision is more critical to a benefits package than you might think.Employees who have a vision benefit are nearly twice as satisfiedwith their benefits - and are more than twice as likely to saybenefits are a reason they stay with their employer.1Employees NeedVision Care3 in 4adults needvision correction.21 in 4childrenneed visioncorrection.2Powerful PreventiveHealthcare1 in 5OnlyAmericans get anannual medical exam –only half get the preventivescreenings you’d expect.46 in 10employees say visualdisturbances affect their3quality of work.VSP MEMBER PROMISESATISFACTIONGUARANTEEYour employeeswill be happy orwe’ll make it right.
Rate Summary for Bronze Plan BCBS-NO Secondary Insurance Rate Summary for Gold Plan BCBS Medplus Employee 560 Employee Spouse 1,120 Employee Children 1,016 . Rate Summary for Dental Value. Current Rates. Renewal Rates; 29. 23: 54. 43: 62. 49: Employee Employee Spouse Employee Children Family 92. 72. Rate Summary for .