Transcription
JIDAMeISSN 2582 - 0559“An Official Journal of IDA - Madras Branch” 2019.Available onlineORIGINAL ARTICLESINUS FLOOR AUGMENTATION BY SINUSLIFT BALLOON SYSTEM- A 1 YEAR FOLLOWUP STUDYDr. A. Archana MeenakshiDepartment of Periodontology and Implantology,Ragas Dental College and Hospital, Chennai, Tamilnadu, India.To access & cite this articleWebsite: jidam.idamadras.comAddress for correspondence:Dr. A. Archana Meenakshi, MDS.,Reader,Department of Periodontology andImplantology,Ragas Dental College and Hospital, Chennai,Tamilnadu, India.ReceivedAcceptedPublished125ABSTRACTA maxillary sinus floor augmentation procedure(also known as sinus lift / sinus procedure) isa surgical technique to augment bone mass inthe maxilla which increases the likelihood ofsuccessful placement of dental implants. Therevolutionary concept of osseointegration isconsidered highly predictable. Today the implantsupported oral restorations are among the mostupdated treatment options for treating edentulousor partially edentulous jaws opting for a fixedprosthesis. This study aimed to assess the safetyand efficacy of a minimally invasive techniquefor maxillary sinus elevation using the sinus liftballoon system (Zimmer Dental); followed byaugmentation of the sinus with cancellous boneallograft (RMTB) and to evaluate the clinical andradiological outcomes of sinus floor augmentationprocedure using OPG, over a one-year period.KEYWORDS : Osseointegration, Schneider’smembrane, pneumatization, osteotome, MIAMBE.: 26.7.2019: 12.9.2019: 27.12.2019JIDAM/Volume:6/Issue:4/Pages 125 - 130/October - December 2019
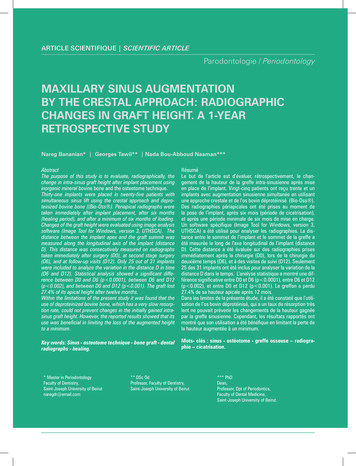
Archana: Sinus floor augmentation by sinus-lift balloon systemINTRODUCTION:Oral rehabilitation with implant supportedprosthesis is considered the therapeutic procedure ofchoice for partially or completely edentulous patients.Implant success and primary stability are greatlyaffected by localized bone density, with implantsplaced in areas of poorer bone quality associated withhigh failure rates1. The posterior region of edentulousmaxilla frequently presents insufficient bone forrehabilitation by means of endosseous implants. Thismight be because of alveolar bone resorption andpneumatization of the maxillary sinus2. One methodthat makes implant placement possible in suchdifficult situations is the augmentation of maxillarysinus using various graft materials. This procedureinvolves the detachment of Schneiderian membranefrom the maxillary sinus floor, creating a space filledwith grafting material, to promote vertical boneaugmentation into the maxillary sinus cavity.In 1994, Summers introduced osteotomesinus floor elevation,with different carrier materials. Irradiated allogeniccancellous bone and marrow particulate graftsrandomly sized between 2-3mm have also been usedas bone substitute for autogenous bone graft.AIM OF THE STUDY: 1. To assess the safety and efficacy of a minimallyinvasive technique for maxillary sinus elevationusing the Sinus lift Balloon system (ZimmerDental); followed by augmentation of the sinuswith Cancellous Bone Allograft (RMTB). 2. To evaluate the clinical and radiologicaloutcomes of sinus floor augmentation procedureusing OPG, over a one-year period.MATERIALS AND METHODS:The study included a total of 10 patients,7males and 3 females, aged between 25 to 60 yrs,for implant placement in the edentulous posteriormaxilla. Informed written consent to participatein this study was obtained from all patients, afterexplaining the objectives and protocol of the study,and possible side effects.INCLUSION CRITERIA:Patients were selected using the following criteria:Fig 1- Osteotome sinus floor elevation techniquewhich is a minimally invasive technique that allowsfor localized maxillary sinus elevation, in alveolarcrest with a residual bone height of 5 - 10 mm3. Aminimally invasive technique for sinus membraneelevation (MIAMBE) which is a modification ofosteotome technique using balloon inflator securedinto the osteotomy site was introduced by Kfir et al(2006) 4. In this technique, inflation of the balloonelevated the sinus membrane, which was followedby bone augmentation and implant placement.MIAMBE resulted in high procedural success,satisfactory bone augmentation, implant survivaland less complication rates. Because it is minimallyinvasive, this technique may be used as an alternativeto the existing sinus augmentation procedures. A widevariety of graft materials have been used to augmentbone volume within the sinus: demineralised freezedried bone allograft (DFDBA), hydroxyapatitepreparations, calcium phosphate preparations andxenografts as well as growth factors embedded126 With a unilateral or bilateral loss of teeth in themaxillary premolar or molar area. Crestal bone height greater than 5mm below thesinus floor as determined by an OPG. Patients with Class B, division–V (VerticalDefect) were included (ABC classification byHom-Lay Wang 2008)5. a) The bone crest is 6to 9mm from the sinus floor. b) The bone widthis 5mm or more. c) The bone crest is more than3mm from the adjacent CEJ. Patients with good oral hygiene and without anyactive periodontal disease were selected.EXCLUSION CRITERIA: Systemic conditions such as uncontrolleddiabetes mellitus, hypertension or any othercontraindicating systemic complications. Patients with immunosuppression and bleedingdisorders.JIDAM/Volume:6/Issue:4/Pages 125 - 130/October - December 2019
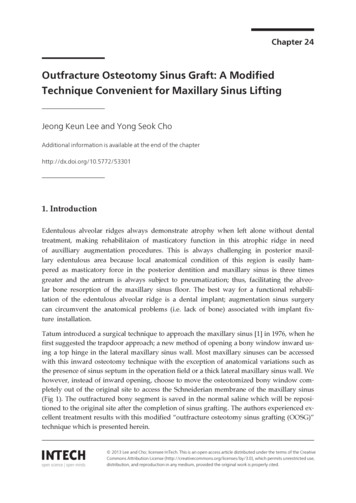
Archana: Sinus floor augmentation by sinus-lift balloon system Patients with orofacial cancer, chemotherapy orhead and neck radiotherapy twelve months priorto the surgery. Any pathological lesion in the sinus. Untreated active periodontitis in neighbouringteeth. Patients with long term steroid therapy orbisphosphonate medication. Patients who are not current smokers. Pregnant women and nursing mothers. Any previous history of sinus surgery. Patients with any drug abuse including alcohol.MATERIALS USED:SINUS-LIFT BALLOON SYSTEMFig 3a & 3b - Sinus lift balloon system The Sinus-lift balloon system (Zimmer Dental)was developed to gently elevate the Schneiderianmembrane with minimal trauma and without theuse of sharp instruments. The apparatus is a pneumatic device consisting ofa 5ml syringe, polyvinyl chloride (PVC) tubingand a metal shaft with the tip connected to alatex mini balloon with an inflation capacity ofapproximately 5cm3. The amount of saline placed in the syringe wasdetermined by the number of millimeters thesinus membrane would need to be elevated –1cc of saline solution corresponds to 6mm ( /0.5mm) of membrane elevation.RADIOGRAPHIC EXAMINATION:Preprocedural panoramic radiographs wereused to assess the vertical bone height (VBH) belowthe sinus lining.BONE GRAFTSFig 2 - Tracing of OPGDigital periapical radiographs were takenbefore the procedure was initiated. Evaluation ofVBH from the alveolar crest (arbitrary horizontalline joining the CEJ of the adjacent teeth) to the floorof the sinus, was done using OPG. The followingthree points were marked on the arbitrary horizontalline joining the CEJ. Point A- 2mm from the mesialtooth. Point B- Midpoint from the line joining pointA & C. Point C- 2mm from the distal tooth. Fromthese 3 points mentioned above, vertical arbitrarylines were drawn to the floor of the maxillary sinusand the values were recorded.127Fig 4 - Bone graftIrradiated allogenic cancellous bone andmarrow particulate bone graft (Rocky MountainTissue Bank, Denver, Co) randomly sized between 2to 3mm has been used as a bone substitute for sinusaugmentation in this study. It is a trabecular allograftobtained from the spinal column and treated with 2.5JIDAM/Volume:6/Issue:4/Pages 125 - 130/October - December 2019
Archana: Sinus floor augmentation by sinus-lift balloon systemslowly inflated with gentle inflating pressure withand 3.8 megarads of radiation.SURGICAL TECHNIQUE:Under local anesthesia, alveolar mid-crestalhorizontal incision wasFig 7a,7b & 7c - Balloon inflation of the surgicalsite doneFig 5 - Incision placedplaced in the edentulous site and connected withsulcular incision of adjacent teeth. Mucoperiosteal flapwas elevated exposing alveolar crest of the bone. Novertical releasing incision was used and the flap wasreflected not exceeding the alveolar ridge. Corticalperforation was done using a round bur, followedby pilot drill reaching about 1mm short of the sinusfloor (After radiographic verification of the sinusfloor with digital periapical radiographs). Sequentialexpansion of the osteotomy site was achievedFig 6a & 6b - Flap elevated and pilot drilling of thesurgical site doneusing a series of osteotomes (from 3.8mm to 5mm)in graduated diameters, to laterally condense the lowdensity maxillary bone. Care was taken to gentlypenetrate the sinus floor and slightly elevate theSchneiderian membrane to allow 3mm of access forthe deflated balloon. Valsalva maneuver is followed.The sinus lift balloon was anchored and securedinto the osteotomy site. Then the balloon was128normal saline (1cc of saline solution correspondsto 6mm of membrane elevation). Digital periapicalradiographs were taken to assess the balloon inflationand the extent of sinus floor elevation at the surgicalsite during the procedure. Once the desired elevation(usually greater than 10mm) was obtained, theballoon was deflated. A second test of membraneintegrity was done by Valsalva manoeuvre. Irradiatedallogenic cancellous bone and marrow (RMTB)was filled under the elevated sinus membraneusing bone condensers.Simple interruptedsutures were placed using 3-0 silk suture material.Fig 8 - Flap suturedPost-operative instructions and antibiotic coveragewere given. Patients were examined after a weekand suture removal was done. The grafted sinus wasallowed to heal for 6 months.POST-OPERATIVE RADIOGRAPHICEVALUATION:During the 3 months and 6 months follow-upJIDAM/Volume:6/Issue:4/Pages 125 - 130/October - December 2019
Archana: Sinus floor augmentation by sinus-lift balloon systemperiod, radiographic assessmentimplants.Fig 9 - post-operative IOPAof the vertical bone gain in the augmented sites wasdone using OPG at the three reference points (A, B,C).STATISTICAL ANALYSIS:The paired ‘t’ Test was adopted to evaluatethe significance of differences in the mean boneheight (MBH)RESULTS: Clinically, no complications were observedduring or after the surgical procedure. No signs and symptoms of maxillary sinuspathology There was a significant increase in the mean boneheight (MBH) post-operatively at the 3 monthsfollow-up period. Point A- 2.3mm, Point B -3.2mm, Point C- 1.8mm Which consistently increased during the 6 monthsfollow-up period (point A- 2.7mm, point B- 3.34mm, point C-2mm)DISCUSSION:First introduced by Dr. Hilt Tatum in 1974,sinus lining elevation was done using inflatablecatheters between 1975 – 1979. Boyne and James7authored the first publication on the technique in 1980- when they published case reports of autogenousgrafts placed into the sinus and allowed to heal for6 months, which was followed by the placement ofThe present study was undertaken to assessthe safety and efficacy of a minimally invasivetechnique (MIAMBE) for maxillary sinus elevationusing the sinus lift balloon system (Zimmer Dental);followed by augmentation of the sinus with irradiatedcancellous bone allograft (Rocky Mountain). Theimplant placement was planned after a six-monthfollow-up period. It is generally preferred to delayimplant placement by several months after thegrafting phase, to allow adequate graft maturation.In the present study, the radiographic assessmentwas based on panoramic radiographs. Although CTscan is considered to be the most accurate meansfor the diagnosis of sinus pathologies and for theevaluation of sinus membrane thickness, periapicaland panoramic radiographs were also frequentlyused to diagnose radiodensities and mucosal cysts(Casamassimo PS1980)8. OPG can only be usedfor the assessment of bone height because it offersonly a two-dimensional view, therefore volumemeasurement could not be assessed. There was asignificant increase in the mean bone height (MBH)post-operatively at the 3 months follow-up period,which consistently increased during the 6 monthsfollow-up period at the 3 reference points (A, B,C).This study utilized irradiated allogenic cancellousbone and marrow graft (RMTB) for augmentationof the sinus. It has been shown that among allavailable allografts, irradiated bone is most similar toautogenous bone, demonstrating rapid replacement& consistent establishment of a reasonable ratio ofnew bone6. NS Soltan et al (2005)9 reported antralmembrane balloon elevation via a lateral bonefenestration. The procedure was highly successfuland predictable. Xiulian Hu et al (2009)10 assessedthe efficacy and safety of MIAMBE followed bybone grafting and implant placement in 28 patients.MIAMBE can be used as a predictable alternative tothe invasive sinus augmentation procedures whichare currently in use.CONCLUSION:6129Within the limits of this study, the followingconclusions have been elucidated: MIAMBE is safe and effective for maxillary sinusaugmentation. The procedure yielded satisfactorybone augmentation results.JIDAM/Volume:6/Issue:4/Pages 125 - 130/October - December 2019
Archana: Sinus floor augmentation by sinus-lift balloon system This procedure eliminates the complications,discomfort and also shortens the surgical time. Particulate irradiated cancellous bone allograft(RMTB) augmentation was biocompatibleand seemed to improve new bone formationin sinus grafting. It can be used as a substitutefor autogenous grafts in sinus augmentationprocedures.Thus, it is appropriate to conclude that, sinusfloor elevation using “Sinus-lift Balloon System(Zimmer Dental)” has obvious advantages, pavingway for maximal augmentation of the sinus forsuccessful implant placement in future. Because it isminimally invasive, this technique may be used as analternative to the currently employed maxillary sinusaugmentation methods. However, further controlledclinical trials with large sample size, advancedradiographic and histomorphometric analysis shouldbe executed to evaluate the effectiveness and safety ofthis technique compared to other sinus augmentationprocedures.FINANCIAL SUPPORT ANDSPONSORSHIP:5. Hom-Lay Wang; Katranji, Amar. ABC al of Periodontics & Restorative Dentistry2008, Vol. 28 Issue 4, p382-389. 8p. 1 ColorPhotograph, 11 Diagrams, 1 Chart.6. Tatum H Jr (1986). “Maxillary and sinus implantreconstructions”. Dent Clin North Am. 30: 207–229.7. Boyne PJ, James RA. Grafting of the maxillarysinus floor with autogenous marrow and bone. JOral Surg. 1980 Aug;38(8):613-6.8. Casamassimo PS, Lilly GE. Mucosal cysts ofthe maxillary sinus; A clinical and radiographicstudy. Oral surg Oral Med Oral Pathol 1980;50:282-286.9. Soltan M, Dennis G. Smiler: Antral membraneballoon elevation: J Oral Implantol 2005:31:8590.10. Xiulian Hu; Ye Lin; Metzmacher, Arnulf-Reimar;Yu Zhang. Sinus Membrane Lift Using a WaterBalloon Followed by Bone Grafting and ImplantPlacement: A 28-Case Report. InternationalJournal of Prosthodontics . 2009, Vol. 22 Issue 3,p243-247. 5p. 7 Color Photographs, 4 Black andWhite Photographs.NilCONFLICTS OF INTEREST:There are no conflicts of interest.REFERENCES:1. Adell R, Eriksson B, Lekholm U, BranemarkPI, Jemt T: Long-term follow-up study ofosseointegrated implants in the treatment oftotally edentulous jaws: Int J Oral MaxillofacImplants. 1990; 5:347-59.2. Akesson L, Rohlin M, Hakansson J. Comparisonbetween panoramic and posterior bitewingradiography in the diagnosis of periodontal boneloss. J Dent 1989;17:266-271.3. Summers RB. A new concept in maxillary implantsurgery: The Osteotome technique. CompendContin Educ Dent 1994:15:152-162.4. Kfir E1, Kfir V, Mijiritsky E, Rafaeloff R, KaluskiE. Minimally invasive antral membraneballoon elevation followed by maxillary boneaugmentation and implant fixation.J OralImplantol. 2006;32(1):26-33.130JIDAM/Volume:6/Issue:4/Pages 125 - 130/October - December 2019
Implant success and primary stability are greatly affected by localized bone density, with implants placed in areas of poorer bone quality associated with . First introduced by Dr. Hilt Tatum in 1974,6 sinus lining elevation was done using inflatable catheters between 1975 - 1979. Boyne and James7