Transcription
TELEMETRYBASICS FORNURSINGSTUDENTS
““Accuracy of cardiacmonitoring is an importantcomponent of patient safetyin hospitalized patients whomeet the criteria fordysrhythmia monitoring.”(AACN, 2016, p. e26)2
OBJECTIVES Following review of the material, the studentnurse will be able to list the three criteria fora normal sinus rhythm. Following review of the material, the studentnurse will be able to list at least two nursinginterventions for abnormal rhythms. Following review of the material, the studentnurse will be able to list one indication forproper telemetry lead placement.Disclaimer: this presentation is not a complete guide to cardiacmonitoring and does not replace formal telemetry training.3
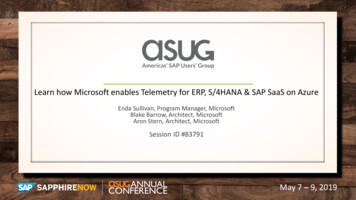
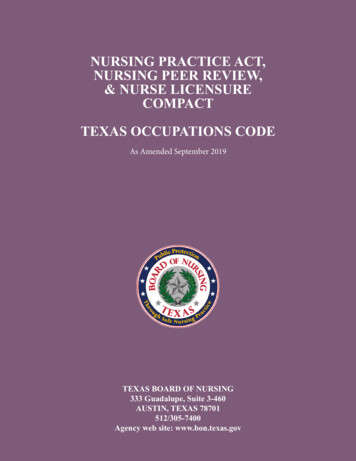
THE STRIPThe horizontal axis measures time(Lieberman, 2008) Little boxes 0.04 secondsBig boxes 0.2 secondsThe vertical axis represents electricalstrength 4This Photo by Unknown Author is licensed under CC BY-SALittle box 1 millivolt (mV), or 1millimeter (mm)
THE LEADS This Photo by Unknown Author is licensed under CC BY-SA5Think of the telemetry leads as acamera looking in through thewindows of the house at the heart Negative (downward) inflection current going away from lead(Lieberman, 2008) Positive (upward) inflection current going toward lead
UNDERSTANDINGLEADS Leads V1-V6 view the heart in thetransverse plane (Lieberman, 2008) called precordial leads Leads I, II, III, aVR, aVL, and aVF view theheart in the frontal plane Called limb leadsApplication: If a heart attack is suspected,knowing the anatomical place the lead is “looking”at can help determine which area is not receivingblood (ischemia).Ischemia presents as ST segment elevation ordepression. See here for tutorial.6This Photo by Unknown Author islicensed under CC BY-NC-SA
LEAD PLACEMENT Loose or incorrectly placed leads maycause false alarms or misdiagnosedrhythms (AACN, 2016). Use anatomical markers to applystickers correctly 7This Photo by Unknown Author is licensed underCC BY-NC-SALoose stickers contribute to alarmfatigueIncorrect lead placement changes themorphology (shape) of the waveform
LEAD PLACEMENTProper application of leads: Clean sticker sites with alcohol and/or preptape Clip hair if indicatedChange tele stickers daily with bathApplication: assess condition/location of leadsduring your morning assessment.8
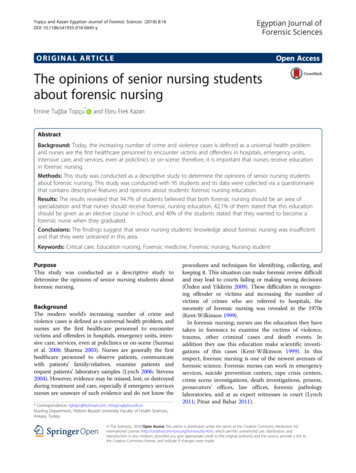
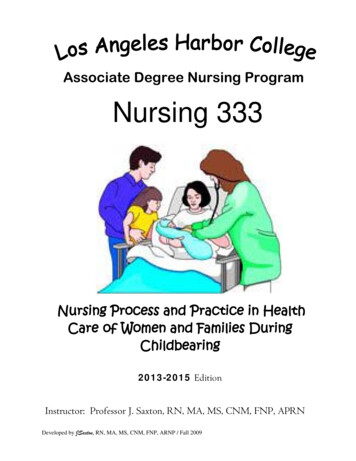
THE EKG TRACINGThis Photo by Unknown Author is licensedunder CC BY-SA9This Photo by Unknown Author is licensed under CC BY-SA P Sinus node firing, atrialdepolarization QRS Ventricular depolarizationT Ventricular repolarization atrial repolarization hidden inQRS
CONDUCTION DEFECTSAbnormal conduction from one part of theheart to another is called a blockSinus node to AV node conduction problem:10 1 : Delayed conduction: Seen as too long from P to QRS Normal PR Interval (PRI) 0.12-0.2 seconds 2 : Intermittent conduction (“dropped” QRS’s)3 : No conduction (patient probably unstable!)
CONDUCTION DEFECTSBundle branch conduction problem: Seen as widened QRSNormal QRS 0.08-0.12Can be right, left, or bifascicular blockApplication: limited clinical significance for beginnersunless new left bundle branch block (LBBB).11This Photo by Unknown Author is licensed under CC BY-SA
SINUS RHYTHMA sinus rhythm means the heart is following the “instructions” of thesinus nodeIndicators of Sinus Rhythm:1.2.3.12P before every QRSRegular rhythm (QRS complexes are equal distance apart)If heart rate (HR) 60-100, called normal sinus rhythm (NSR)This Photo by Unknown Author is licensed under CC BY-SA
HEART RATE (HR) Sinus Tach (ST) sinus rhythm with HR 100 Sinus Brady (SB) sinus rhythm with HR 60Application: 13If your patient has high heart rates, consider physiological factors likepain, bleeding, or missed home medication. If low, may be athletic ortoo high dose of medication.High HR (e.g. 130) may decrease blood pressure since the chamberscannot fill fast enoughCheck for as needed (PRN) medication orders that might help controlrate.
ATRIAL FIBRILATION (A-FIB)In A-fib, multiple areas of the atria are sending out impulses, causingirregular heart rate (hallmark of a-fib)Indicators of A-fib: 14Irregular spacing between QRS complexesNo distinct P-wave—often has many small impulses that look likeartifact
TREATMENT FOR TACHYCARDIAApplication (New-Onset):15 Usually drops blood pressure (BP) since the atria is not filling theventricles. Main treatment goal is to decrease HR which shouldimprove BP. Any new-onset tachycardia should have 12-lead EKG to determine ifa-fib Usually need meds for rate control and/or dysrhythmia, andanticoagulation (blood pools in atria) Note: this is a very common chronic rhythm in elderly. Treatment isvery similar as for new-onset a-fib.
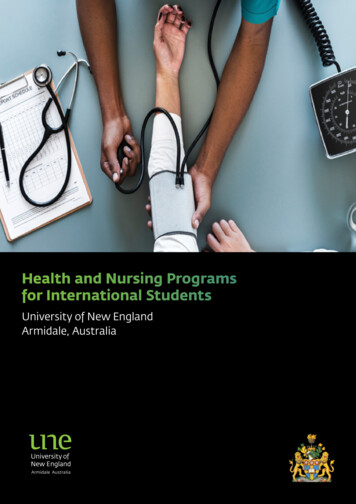
PREMATURE ATRIAL COMPLEX (PAC) 16A random, early QRSSame morphology (shape) asthe other QRS complexes(indicates impulse traveledthrough AV node, so camefrom atria)Application This Photo by Unknown Author is licensed under CC BY-NC-SAFrequent or runs of PAC’s may warn ofirritable heart Check potassium and magnesiumlevel Consider antidysrhythmic meds
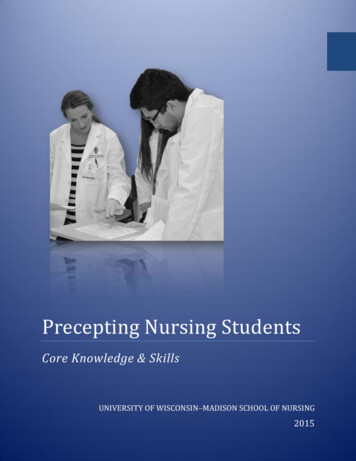
PREMATURE VENTRICULAR COMPLEX (PVC) 17A random, early QRSWidened QRS and differentmorphology (indicatesimpulse originated belowAV node)Application Frequent or runs of PVC’s may warn of irritableheartCheck potassium and magnesium levelConsider antidysrhythmic meds This Photo by Unknown Author is licensed under CC BY-SAMay devolve into ventricular tachycardia (vtach). Life threatening!
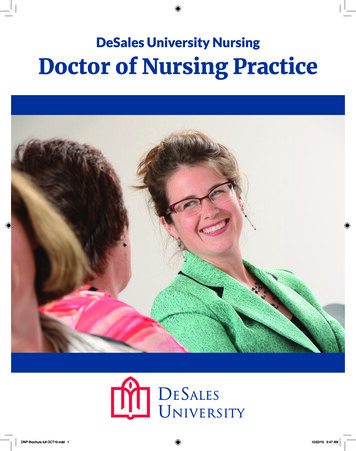
VENTRICULAR TACHYCARDIA (V-TACH)Life threatening!18 Call code blue and shock as soon as possible! Anyone with BLS may operate the AED If untreated, may devolve into ventricular fibrillation (v-fib) and then toasystole. Rapid movement (e.g. brushing teeth) may mimic v-tach, so check patientfirstThis Photo by Unknown Author is licensed under CC BY-NC
REVIEW
OBJECTIVESCan you answer these questions now?20 List the three criteria for a normal sinusrhythm. List at least two nursing interventions forabnormal rhythms. List one indication for proper telemetry leadplacement.
DISCUSSION QUESTIONS Are the leads on your patient in the proper location and sticking well? What questions do you have for your preceptor?What rhythm is your patient in?Did you notice any ectopy (early beats)?Does your patient have a heart block? (unusual)What medications are scheduled or PRN that might affect your patient’s rhythm?Based on your review of your patient’s telemetry/rhythm, what conditions orrhythm changes should you be prepared for?Application: you should be asking yourself these questions anytime you have amonitored patient.21
REFERENCESAmerican Association of Critical Care Nurses. (2016). Accurate dysrhythmiamonitoring in adults. Critical Care Nurse, 36(6), e28-e36.Lieberman, K. (2008). Interpreting 12-lead ECGs: a piece by piece analysis. TheNurse Practitioner, 33(10), 28-35.Both of these articles are highly recommended for the curious.22GL 12.6 (SMOG)
ABOUT MEI wrote this for a BSN teaching project, butreally, I love trying to make tough nursingtopics easier to understand and apply. Ihope this has been useful for you! 23My name is Mark NislyI work in the Critical Care Float Pool(Supplemental Staff) Credentials: RN, CCRN. Experience: 8 years RN, 3 years CNA
BASICS FOR NURSING STUDENTS . Regular rhythm (QRS complexes are equal distance apart) 3. If heart rate (HR) 60-100, called normal sinus rhythm (NSR) 12 This Photo by Unknown Author is licensed under CC BY-SA. HEART RATE (HR) Sinus Tach (ST) sinus rhythm with HR 100 Sinus Brady (SB) sinus rhythm with HR 60 Application: If your patient has high heart rates, consider physiological