Transcription
JOURNAL OF ORAL & MAXILLOFACIAL RESEARCHStarch-Jensen and JensenMaxillary Sinus Floor Augmentation: aTreatment ModalitiesReview of SelectedThomas Starch-Jensen1, Janek Dalsgaard Jensen1Department of Oral and Maxillofacial Surgery, Aalborg University Hospital, Aalborg, Denmark.1Corresponding Author:Thomas Starch-JensenDepartment of Oral and Maxillofacial SurgeryAalborg University Hospital18-22 Hobrovej, DK-9000 AalborgDenmarkPhone: 45 97 66 27 98Fax: 45 97 66 28 25E-mail: thomas.jensen@rn.dkABSTRACTObjectives: The objective of the present study is to present the current best evidence for enhancement of the vertical alveolarbone height and oral rehabilitation of the atrophic posterior maxilla with dental implants and propose some evidence-basedtreatment guidelines.Material and Methods: A comprehensive review of the English literature including MEDLINE (PubMed), Embase andCochrane Library search was conducted assessing the final implant treatment outcome after oral rehabilitation of theatrophic posterior maxilla with dental implants. No year of publication restriction was applied. The clinical, radiological andhistomorphometric outcome as well as complications are presented after maxillary sinus floor augmentation applying thelateral window technique with a graft material, maxillary sinus membrane elevation without a graft material and osteotomemediated sinus floor elevation with or without the use of a graft material.Results: High implant survival rate and new bone formation was reported with the three treatment modalities. Perforation ofthe Schneiderian membrane was the most common complication, but the final implant treatment outcome was not influencedby a Schneiderian membrane perforation.Conclusions: The different surgical techniques for enhancement of the vertical alveolar bone height in the posterior part of themaxilla revealed high implant survival with a low incidence of complications. However, the indication for the various surgicaltechniques is not strictly equivalent and the treatment choice should be based on a careful evaluation of the individual case.Moreover, further high evidence-based and well reported long-term studies are needed before one treatment modality mightbe considered superior to another.Keywords: alveolar ridge augmentation; dental implants; oral surgical procedures; review; sinus floor augmentation.Accepted for publication: 30 September 2017To cite this article:Starch-Jensen T, Jensen JD.Maxillary Sinus Floor Augmentation: a Review of Selected Treatment ModalitiesJ Oral Maxillofac Res 2017;8(3):e3URL: 3.pdfdoi: chives/2017/3/e3/v8n3e3ht.htmJ Oral Maxillofac Res 2017 (Jul-Sep) vol. 8 No 3 e3 p.1(page number not for citation purposes)
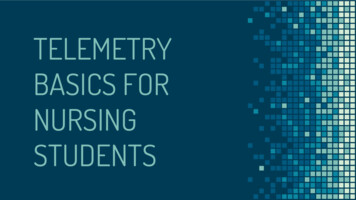
JOURNAL OF ORAL & MAXILLOFACIAL RESEARCHINTRODUCTIONPeriodontal disease and dental caries are the maincauses of tooth loss and the incidence of edentulouspatients varies worldwide between 7% and 69% [1].Complete or partial tooth loss is often associatedwith nutritional deficiencies, oral pain, and poorpsychosocial functioning. During the last 40 years,osseointegrated dental implants have become oneof the most used biomaterial to replace missing orlost teeth and the treatment has been characterisedby a highly successful outcome of complete, partialor single edentulism [2-5]. Oral rehabilitation withimplant-supported prosthesis have shown improvedmasticatory function and oral specific health-relatedquality of life compared to removable dentures [6,7].However, placement of implants in the posteriorpart of the maxilla is frequently compromised orimpossible due to atrophy of the alveolar process,poor bone quality and maxillary sinus pneumatization.Therefore, vertical alveolar ridge augmentationis often necessary before or in conjunction withinstallation of implants. Various surgical approachescomprising elevation of the Schneiderian membranehave been proposed in order to achieve the necessaryvertical height of the alveolar process for theinstallation of implants with a sufficient lengthincluding maxillary sinus floor augmentation with thelateral window technique, osteotome-mediated sinusfloor elevation and sinus membrane elevation withoutthe use of a graft material [8-10]. However, thetreatment of choice for the most appropriate surgicalintervention for oral rehabilitation of the atrophicposterior maxillary ridge with implants is influencedby the vertical height of the residual alveolar bone,local intrasinus anatomy and the number of teeth to bereplaced [10].Different types of biomaterials have been usedfor maxillary sinus floor augmentation includingautograft, allograft, xenograft, alloplast, and growthfactors, and the selection of the ideal graft materialhas been a subject of controversy over the years.Autogenous bone graft is considered the goldenstandard in augmentation procedures due to itsosteoinductive, osteogenic and osteoconductivecharacteristics [11]. However, the use of autogenousbone grafts is associated with risk of donor sitemorbidity and unpredictable graft resorption [1219]. Therefore, various bone substitutes of biologicor synthetic origin are used increasingly to simplifythe surgical procedure by diminishing the needfor bone harvesting. The treatment outcome afterenhancement of the vertical alveolar bone /v8n3e3ht.htmStarch-Jensen and Jensenin the posterior part of the maxilla with the differenttreatment modalities is well-documented and hasbeen reported in numerous systematic reviews andmeta-analysis [20-34]. Although, the conclusions areoften based on short-term non-comparative studies.Therefore, the objective of this comprehensive reviewis to present the current evidence for enhancementof the vertical alveolar bone height in the posteriorpart of the maxilla and propose some evidencebased treatment guidelines for oral rehabilitationof the atrophic posterior maxilla with dentalimplants.SURGICAL METHODS FOR ENHANCEMENTOF THE ALVEOLAR BONE HEIGHT IN THEPOSTERIOR MAXILLAMaxillary sinus floor augmentation applying thelateral window technique with a grafting materialand simultaneous or delayed implant installationMaxillary sinus floor augmentation using the lateralwindow technique was originally developed byTatum [35] in the mid-seventies and afterwardsdescribed by Boyne and James in 1980 [36]. Thissurgical intervention is still the most frequentlyused method to enhance the vertical alveolar boneheight of the posterior part of the maxilla beforeor in conjunction with installation of implants,and the treatment outcome has been reported inseveral systematic reviews and meta-analysis[20-25].Surgical techniqueMaxillary sinus floor augmentation applying thelateral window technique is usually performed underlocal anaesthesia and sedation. The maxillary sinusis exposed through the oral mucosa in the regionof the anterior and lateral maxillary sinus wall. Amidcrestal incision is made with posterior and anteriorvertical releasing incisions. A mucoperiosteal flapwith a trapezoid base is reflected exposing the lateralwall of the maxillary sinus. A trapdoor osteotomyis performed on the lateral wall of the maxillarysinus with burrs and a high-speed handpiece orpiezoelectric surgery advoiding laceration of theSchneiderian membrane (Figure 1A). The trapdooris infractured and the Schneiderian membrane iscarefully dissected and elevated from the maxillarysinus floor as well as the lateral and medial sinuswall and displaced dorsocranially with bluntdissector to create a compartment for placement ofthe graft material (Figure 1B). Implants are insertedJ Oral Maxillofac Res 2017 (Jul-Sep) vol. 8 No 3 e3 p.2(page number not for citation purposes)
JOURNAL OF ORAL & MAXILLOFACIAL RESEARCHStarch-Jensen and JensenABCDFigure 1. Maxillary sinus floor augmentation applying the lateral window technique with a grafting material. A a trapdoor osteotomy isperformed on the lateral wall of the maxillary sinus. B the trapdoor is infractured and the Schneiderian membrane is carefully dissectedand elevated from the maxillary sinus floor to create a compartment for placement of the graft material. C the implant is insertedsimultaneously with the augmentation procedure. D the graft material is densely packed around the exposed implant surface in the createdcompartment.simultaneously with the augmentation procedure,if the height of the residual alveolar bone providessufficient primary implant stability. An implant bed issuccessively prepared with burrs before the implantare inserted in the residual alveolar bone with theimplant tip exposed in the created compartment inthe maxillary sinus (Figure 1C). The graft materialis densely packed around the exposed implantsurface to facilitate de novo bone formation (Figure1D). The lateral window to the maxillary sinus isusually covered by a resorbable collagen e3/v8n3e3ht.htmto prevent ingrowth of fibrous tissue before themucoperiosteum is readapted and sutured. If primaryimplant stability is compromised, then the implantsare inserted 4 to 12 months after the augmentationprocedure. Final prosthetic solution is performed threeto six months after implant installation.Clinical outcomeRecent systematic reviews and meta-analysis haveassessed the implant survival after maxillary sinusJ Oral Maxillofac Res 2017 (Jul-Sep) vol. 8 No 3 e3 p.3(page number not for citation purposes)
JOURNAL OF ORAL & MAXILLOFACIAL RESEARCHfloor augmentation with various types of graftmaterials disclosing an overall implant survival ratewell-beyond 90% [20-25]. The implant survival ratewas equivalent regardless of the used graft materialand time of implant placement [24,25]. Moreover,a newly published systematic review and metaanalysis assessing the long-term implant treatmentoutcome concluded that maxillary sinus flooraugmentation with autogenous bone graft, mixture ofautogenous bone graft and bone substitutes or bonesubstitutes alone seem to be a highly predictableand successful surgical procedure to enhancethe vertical alveolar bone height of the posteriorpart of the maxilla before or in conjunction withimplant placement with a high implant survival rate[24].Radiological and histomorphometric outcomeRecent published systematic reviews assessinghistomorphometric variables after maxillary sinusfloor augmentation concluded that autogenous bonegraft resulted in the highest amount of newly formedbone in comparison to various bone substitutes,though allografts, alloplastic materials and xenograftsseemed to be a good alternative to autogenous bonegraft [23,37]. Moreover, a meta-analysis assessingthe total bone volume after maxillary sinus flooraugmentation based on histomorphometric analysisdemonstrated a significantly higher proportion ofmineralized bone during the early healing phase whenautogenous bone was used as graft as compared withvarious bone substitutes used alone or in combinationwith autogenous bone graft [38]. However, ahealing period of more than 9 months revealed nostatistically significant differences between thedifferent treatment modalities [37]. A newly publishedsystematic review and meta-analysis evaluated theeffect of a barrier membrane over the lateral windowdemonstrating similar amount of bone formationwith or without a barrier membrane [39]. Moreover,the type of grafting material and healing time didnot influence the histomorphometric outcome [39].The effect of autogenous platelet concentrates onthe clinical and histomorphometric outcome haspreviously been evaluated in a systematic reviewdisclosing no evidenced beneficial effect of plateletconcentrates due to large heterogeneity among theincluded studies [40]. The bone-to-implant contactand the volumetric stability of the graft materialafter maxillary sinus floor with autogenous bonegraft alone or in combination with different ratiosof deproteinized bovine bone mineral has beenevaluated in an experimental minipigs model e3/v8n3e3ht.htmStarch-Jensen and JensenIt was concluded that the bone-to-implant contactwas significantly higher when autogenous bone graftor deproteinized bovine bone mineral mixed withautogenous bone graft in different ratios were usedas compared to deproteinized bovine bone mineralalone, after 12 weeks [41]. In addition, fluorochromelabelling indicated that the early bone to implantcontact formation adjacent to the implant surfacewas more advanced with autogenous bone graftcompared to deproteinized bovine bone mineral [41].Computed tomography scans obtained preoperatively,immediately after surgery, and after 12 weeks showeda significant volumetric reduction of autogenousbone grafts from the iliac crest and the mandible[18]. Increased graft preservation occurred after theaddition of deproteinized bovine bone mineral andthe volumetric reduction was significantly influencedby the ratio of deproteinized bovine bone mineral andautogenous bone graft [18]. Volumetric dimensionalchanges of the graft material after maxillary sinusfloor augmentation has previously been assessed ina systematic review concluding that some loss ofthe augmentation volume always occurs, but bonesubstitutes or composite grafts display less volumereduction compared to autogenous bone graft[19].ComplicationsPerforation of the Schneiderian membrane is the mostcommon operative complication during maxillarysinus floor augmentation [42-45]. Presence of sinussepta and a residual bone height less than 3.5 mmincreases the risk for a sinus membrane perforation[46]. However, perforation of the Schneiderianmembrane seems not to influence the final treatmentoutcome [42-45], but a higher prevalence for sinusitisis reported in cases of membrane perforation [46].Other complications include bleeding, migration ofdental implants into the maxillary sinus, postoperativeinfection, sinusitis, exposure of the graft, graft loss,oedema, seroma formation, benign paroxysmalpositional vertigo and exposure of the collagenmembrane. Smokers generally exhibited greaterchances for complications and a newly publishedsystematic review concluded that smoking seems tobe associated with increased risk of wound dehiscenceand infection after maxillary sinus floor augmentation[46,47]. However, complications related to maxillarysinus floor augmentation applying the lateral windowtechnique with a grafting material are generally lowand not severe, as documented in systematic reviews[20,24].J Oral Maxillofac Res 2017 (Jul-Sep) vol. 8 No 3 e3 p.4(page number not for citation purposes)
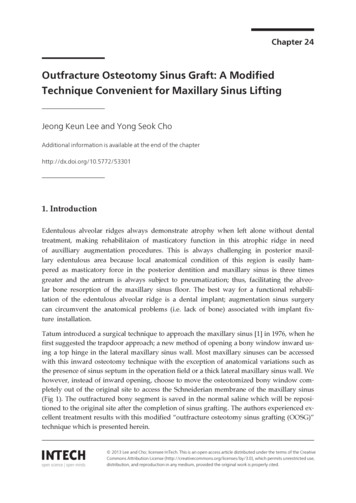
JOURNAL OF ORAL & MAXILLOFACIAL RESEARCHConclusion and clinical recommendationsMaxillary sinus floor augmentation applying thelateral window technique with a grafting materialis a safe and predictable surgical procedure withlow morbidity for oral rehabilitation of the severelyatrophic posterior maxilla with dental implants. Thissurgical intervention is recommended when theheight of the residual alveolar bone is less than 6 mm.Dental implants are inserted simultaneously with theaugmentation procedure, if the height of the residualalveolar bone provides sufficient primary implantstability. If not, then the implants are inserted 4 to 12months after the augmentation procedure, dependingof the used graft material.Maxillary sinus membrane elevation applying thelateral window technique without a graft materialand simultaneous implant installationMaxillary sinus membrane elevation using the lateralwindow technique without a graft material andsimultaneous installation of implants was introducedby Lundgren et al. in 2004 [48]. This surgicalintervention requires sufficient vertical height ofthe residual alveolar bone in the posterior part ofthe maxilla to achieve primary implant stability,since immediate implant installation is necessaryto preserve and support the elevated Schneiderianmembrane, allowing coagulum formation round theexposed implant surface in the sinus cavity. Thetreatment outcome has been reported in varioussystematic reviews and meta-analysis involvingpredominantly short-term non-comparative studies[26,27,29,30,34], but long-term studies are scarce.Surgical techniqueThe formation of the lateral window, elevation of theSchneiderian membrane and implant installation issimilar to the surgical technique described above formaxillary sinus floor augmentation with a graftingmaterial and simultaneous implant installation,although the implant bed is usually prepared with anundersized drilling protocol and the lateral corticalbony window is often dissected free and removed fromthe underlying Schneiderian membrane (Figure 2A). Ablood coagulum is formed around the exposed implanttip in the secluded compartment between the elevatedSchneiderian membrane and the original floor of themaxillary sinus (Figure 2B). The lateral window to themaxillary sinus is covered by a resorbable collagenmembrane or the dissected lateral cortical bonywindow. The mucoperiosteum is readapted and 3/v8n3e3ht.htmStarch-Jensen and Jensen(Figure 2C). Final prosthetic solution is usuallyperformed three to six months after maxillary sinusmembrane elevation and implant installation, when denovo bone is formed around the implant (Figure 2D).Clinical outcomeRecent systematic reviews and meta-analysis haveassessed the implant survival after maxillary sinusmembrane elevation using the lateral windowtechnique without a graft material and simultaneousinstallation of implants disclosing an implant survivalrate beyond 90% [26,27,29,30,34]. However, longterm studies are scarce. A 5-year implant survivalrate of 100% has been reported after maxillary sinusmembrane elevation without a graft material andsimultaneous installation of 80 implants in 44 patients[49]. Moreover, an implant survival of 99% has beendescribed in a 1 to 6-year follow-up study involving189 implants inserted in 84 patients [50]. However,only 14 implants inserted in 6 patients were followedfor 6 years [50].Radiological and histomorphometric outcomeAssessment of intra-sinus new bone formationand bone density after maxillary sinus membraneelevation using the lateral window technique withouta graft material has been compared with maxillarysinus floor augmentation applying the lateral windowtechnique with autogenous bone graft or allogenicmineralized bone graft [51,52]. The average verticalalveolar bone gain after 6 months was 7.9 mm withouta graft material and 8.3 mm when an autogenousbone graft was used [51]. There was no significantdifference in the vertical alveolar bone gain betweenthe two treatment modalities at any time-points[51]. Radiographic assessment showed that the bonedensity increased significantly during the observationperiod, but the bone density was significantly higherin sinuses augmented with a blood clot compared toan allogenic mineralized bone graft after 6 months[52]. A non-comparative study assessing maxillarysinus membrane elevation with the lateral windowtechnique without a graft material demonstrated anintra-sinus vertical alveolar bone gain of 7.4 mm after5 years, with no significant changes in the gainedbone height between 2 and 5 years [52]. Moreover,the gain in intra-sinus vertical alveolar bone heightwas increased significantly for implants protrudinglonger into the sinus cavity compared to implants withonly a minor part of the implant tip exposed [52,53].Histologic evaluation of biopsies retrieved aftermaxillary sinus membrane elevation with the lateralJ Oral Maxillofac Res 2017 (Jul-Sep) vol. 8 No 3 e3 p.5(page number not for citation purposes)
JOURNAL OF ORAL & MAXILLOFACIAL RESEARCHStarch-Jensen and JensenABCDFigure 2. Maxillary sinus membrane elevation applying the lateral window technique without a graft material and simultaneous implantinstallation. A the lateral cortical bony window is dissected free and removed from the underlying Schneiderian membrane, which iscarefully elevated from the maxillary sinus floor to create a compartment for placement of the graft material. B a blood coagulum isformed around the exposed implant tip in the secluded compartment between the elevated Schneiderian membrane and the original floor ofthe maxillary sinus. C the window to the maxillary sinus is covered by the dissected lateral cortical bony window. D new bone formationaround the implant tip in the previous created compartment.window technique without a graft material revealednew bone formation and a mean vital bone volumevarying between 39% and 60%, after 6 months[54-56].ComplicationsPerforation of the sinus membrane was the mostfrequent intraoperative complication, although veryrare [26,27,29,30]. A higher risk of sinus e3/v8n3e3ht.htmperforationhas been reported, when the lateral corticalbony window was dissected free and removed fromthe underlying Schneiderian membrane [29]. However,the treatment outcome seems not to be influencedby a sinus membrane perforation, although implantloss has been reported in a case with a perforation ofthe sinus membrane [29,50]. Other n,exposure of the covering membrane, swelling,mild postoperative oedema, pain, loosening ofJ Oral Maxillofac Res 2017 (Jul-Sep) vol. 8 No 3 e3 p.6(page number not for citation purposes)
JOURNAL OF ORAL & MAXILLOFACIAL RESEARCHStarch-Jensen and Jensenhealing abutments, and nose bleeding [29].Surgical techniqueConclusion and clinical recommendationsOsteotome-mediated sinus floor elevation andsimultaneous installation of implants with or withoutthe use of a graft material is performed under localanaesthesia and sedation. An intraoral midcrestalincision is made with or without a vertical releasingincision. Mucoperiosteum is reflected along theresidual alveolar ridge and the implant position ismarked on the alveolar crest with a small roundbur. The implant bed is prepared with a seriesof osteotomes with increasing diameter or incombination with burrs to a depth approximately 1 to2 mm away from the maxillary sinus floor boundary(Figure 3A). An up-fracture of the maxillary sinusfloor is made with a mallet under light tapping andthe Schneiderian membrane with the maxillary sinusfloor is carefully elevated using an osteotome or ablunt instrument (Figure 3B). The integrity of themembrane is controlled with Valsalva maneuver,before grafting material may be added to the liftedarea underneath the elevated Schneiderian membranewith the original maxillary sinus floor. The implantis inserted in the residual alveolar bone with theimplant tip exposed in the lifted area (Figure 3C).Mucoperiosteum is readapted and sutured. Finalprosthetic solution is performed three to six monthsafter osteotome-mediated sinus floor elevation withsimultaneously implant installation, when de novobone is formed around the implant (Figure 3D).Maxillary sinus membrane elevation applying thelateral window technique without a graft materialand simultaneous implant installation seems to bea safe and predictable surgical procedure with fewcomplications and a high short-term implant survivalrate. However, no consensus has yet been reachedon the amount of bone formation and predictabilityfor installation of numerous implants in the posteriorpart of the maxilla with this surgical intervention.Moreover, long-term clinical and radiographic studiesassessing the final implant treatment outcome arescarce. Thus, further long-term comparative studies areneeded before final conclusion can be provided aboutthis surgical intervention for oral rehabilitation of theatrophic posterior maxilla with dental implants. It isour opinion that maxillary sinus membrane elevationusing the lateral window technique without a graftmaterial and simultaneous implant installation shouldsolely be recommended for single implant installation,when a limited amount of bone regeneration is needed.Osteotome-mediated sinus floor elevation andsimultaneous installation of implants with or withoutthe use of a graft materialThe osteotome-mediated transcrestal sinus liftapproach was first proposed by Tatum in 1986 [35].In 1994, Summers [57] described a modificationof this technique using a set of tapered osteotomeswith increasing diameters intended to increase thedensity of the soft bone and create an up-fractureof the maxillary sinus floor. The Schneiderianmembrane and the maxillary sinus floor is elevatedfrom a transcrestal approach using osteotomescreating a compartment for graft placement and/or blood clot formation, without the preparation of alateral window. Implants are inserted immediately tosupport the elevated floor of the maxillary sinus withthe Schneiderian membrane. Osteotome-mediatedsinus floor elevation is most suitable for installationof a single implant but can be used for multipleimplants. The treatment outcome has been reportedin reviews, systematic reviews and meta-analysiscomprising predominantly short-term studies [3133,58-61]. Osteotome-mediated sinus floor elevationwith simultaneous installation of implants with orwithout the use of a grafting material are consideredless invasive and time-consuming than maxillarysinus floor augmentation applying the lateral /2017/3/e3/v8n3e3ht.htmClinical outcomeVarious systematic reviews and meta-analysis haveassessed the implant survival after osteotomemediated sinus floor elevation and simultaneousinstallation of implants with or without the use of agraft material revealing an overall implant survivalrate higher than 90% [31-33,58-61]. However, longterm studies are scarce. A newly published systematicreview and meta-analysis disclosed no statisticallysignificant difference in short-term implant survivalrate between osteotome-mediated sinus floor elevationand simultaneous installation of implants with orwithout the use of a graft material [61]. A 10-yearimplant survival rate of 100% has been reportedafter osteotome-mediated sinus floor elevation andsimultaneous installation of 23 implants in 15 patientswithout the use of a graft material [62]. The implantsurvival rate after osteotome-mediated sinus floorelevation and simultaneous installation of implants issignificantly higher when the residual vertical alveolarbone height is more than 5 mm, as documented ina systematic review [32]. Moreover, installationJ Oral Maxillofac Res 2017 (Jul-Sep) vol. 8 No 3 e3 p.7(page number not for citation purposes)
JOURNAL OF ORAL & MAXILLOFACIAL RESEARCHStarch-Jensen and JensenABCDFigure 3. Osteotome-mediated sinus floor elevation and simultaneous installation of implants with or without the use of a graft material.A the implant bed is prepared with a series of osteotomes with increasing diameter or in combination with burrs to a depth approximately1-2 mm away from the maxillary sinus floor boundary. B an up-fracture of the maxillary sinus floor is made with a mallet under lighttapping and the Schneiderian membrane with the maxillary sinus floor is carefully elevated with the osteotome or a blunt instrument. C theimplant is inserted in the residual alveolar bone with the implant tip exposed in the lifted area. D new bone formation around the implanttip in the previous created compartment.of short implants ( 6 mm) in conjunction withosteotome-mediated sinus floor elevation significantlydiminished the implant survival rate [58].Radiological and histomorphometric outcomeThe 3-year radiographic assessment of intra-sinus newbone formation after osteotome-mediated sinus floorelevation and simultaneous installation of implantsranged from 3.17 to 5.1 mm with a graft e3/v8n3e3ht.htmand from 1.7 to 4.1 mm without a graft material,as documented in a systematic review and metaanalysis [61]. Moreover, a prospective radiographicstudy assessing the intra-sinus vertical alveolar bonegain after osteotome-mediated sinus floor elevationand simultaneous installation of implants revealedsignificantly more bone gain with a grafting materialcompared to the use of no graft [62]. The 10-yearradiographic intra-sinus new bone formation was3 mm without the use of a graft material and boneJ Oral Maxillofac Res 2017 (Jul-Sep) vol. 8 No 3 e3 p.8(page number not for citation purposes)
JOURNAL OF ORAL & MAXILLOFACIAL RESEARCHformation was more pronounced during the firstyear and tends to increase for three years [63].Consequently, osteotome-mediated sinus floor elevationwith a graft material and simultaneous installationof implants seem to facilitate more vertical alveolarbone gain compared to the use of no graft material.ComplicationsStarch-Jensen and JensenHence, osteotome-mediated sinus membrane elevationis usually indicated when a residual vertical alveolarbone height of more than 6 mm is present. Autogenousbone graft or bone substitutes can be added, if moreintra-sinus bone gain is needed for installation ofimplants with a desirable length.CONCLUSIONSPerforation of the Schneiderian membrane is the mostcommon operative complication after osteotomemediated sinus floor elevation and simultaneousinstallation of implants with or without the use ofa graft material with a mean incidence of 3.8%(range 0 to 21.4) [64]. An oblique maxillary sinusfloor, sinus septa and root apices penetrating into themaxillary sinus increases the risk of Schneiderianmembrane perforation. However, perforation of sinusmembrane seems not to influence the implant survivalrate [64]. Other complications include postoperativeinfection, disorientated after surgery, nose bleeding,blocked nose, hematomas, benign paroxysmalpositional vertigo and postoperative bleeding [58].Conclusion and clinical recommendationsOsteotome-mediated sinus membrane elevation is apredictable and reli
and simultaneous or delayed implant installation Maxillary sinus floor augmentation using the lateral window technique was originally developed by Tatum [35] in the mid-seventies and afterwards described by Boyne and James in 1980 [36]. This surgical intervention is still the most frequently used method to enhance the vertical alveolar bone