Transcription
HEART ATTACKS - WHATS FOR YOU ANDWHATS FOR MEHarvey WhiteJohn Neutze ScholarGreen Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ
Disclosure Statement of Financial InterestWithin the past 12 months, I or my spouse/partner have had a financialinterest/arrangement or affiliation with the healthcare related companylisted belowFinancial Relationship CompanyResearch GrantsSanofi Aventis; Eli Lilly; NIH; MerckSharpe & Dohme; AstraZeneca;GSK; Daiichi Sankyo PharmaDevelopmentConsultingAstraZenecaGreen Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ
Checklist for Secondary Prevention Aspirin P2Y12 inhibitors (Ticagrerlor for 3 years) Beta-blockers Lipid management (statins, ezetimibe 10mg, aim for LDL 1.4mmol/L) Renin angiotensin aldosterone system modulation Blood pressure control Warfarin for apical thrombus Dabigatran or rivaroxiban for atrial fibrillation Diabetes management
Checklist for Secondary Prevention Implantable Cardioverter Defibrillator (ICD with EF 30% 3 monthsoptimal treatment) Cardiac rehabilitation program , with training in CPR, AEDs, andadherence (text messages) Lifestyle modification, nutrition, exercise, weight control Depression, anxiety, stress Influenza vaccination No smoking Exercise 30 min/day on most days
Optimal medical therapyGreen Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ
Guideline – recommended secondarypreventionThere is a 10% lower mortality for each 10% increase incomposite adherence to guideline-recommended therapiesin hospital and a 33% reduction in mortality overall withconsistent use of optimal medical therapy in secondarypreventionGreen Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ
Guidelines – recommended secondaryprevention SYNTAX TRIAL Just over 31.2% of CABG and approximately 50.2% ofPCI patients were discharged on optimal medicaltherapy, and only one third received optimal medicaltherapy (aspirin, antiplatelet, beta blocker, ACE inhibitor,statin) at 5 yearsGreen Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZIqbal. Circulation.2015;131:1269-77
Optimal Medical Therapy.Time from dischargeGreen Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZJavaid Iqbal et al. Circulation.2015;131:1269-1277
Evidence Based Medicine forACSAdherence is very importantGreen Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ
Evidence Based Medicine forACS: How well do we do? Statin use over 3 year follow-up assessed bypharmaceutical dispensing data83% had received a statinAdequate maintenance defined as a MedicationPossession Ratio (MPR) 80%69% first year, 67% second year, 66% third yearLess adherence in Maori or Pacific ethnicityand aged 35-45 yearsGrey et al Heart 2014Green Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ
ACS and Thrombus FormationTHROMBUSGreen Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ
Green Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ
Stenting in ACS what doesit do?Green Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ
Stable Ischemic Heart Disease(SIHD)What is the evidence that a routine strategy ofprompt revascularization after SIHD diagnosisimproves survival/ reduces clinical events?Green Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ
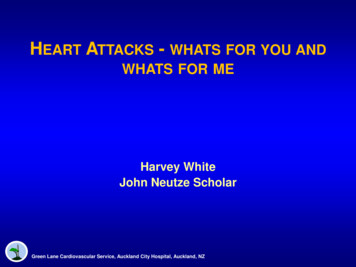
CABG vs no CABGCABG Surgery Trialists Collaboration; 10-year outcome0.500.40Cumulative mortality rate0.50VA studyEuropean study0.40P 0.12 5 yrsP 0.45 10 yrs0.30P 0.001 5 yrsP 0.02 10 yrs0.30n 3540.200.10n 3730.20n 332n 3940.100.0000.500.40Relevance todayis unclear.0.002 There4 6 8 was10 12 minimal0 2or4 no6 use8 10 12No CABGCABG0.50CASS studyAll studiesof effective medicaltherapy0.40(ASA, statins, 0.30beta-blockers,0.20ACE inhibitors).P 0.25 10 yrs0.30P 0.001 5 yrsP 0.03 10 yrsn 3900.200.10n 1,325n 1,3240.10n 3900.000.000246810 120246810 12Time (years)Green Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZYusuf et al. Lancet 1994;344:563-570.
Stable Ischemic Heart DiseasePCI vs. Medicine Pre-COURAGE and BARI 2DMeta-analysis of 11 randomized trials; N 2950Left Main disease excludedFavors PCIFavors Medical ManagementPDeath0.68Cardiac death or MI0.28Nonfatal MI0.12CABG0.82PCI0.3401Risk ratio (95% Cl)Green Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ2Katritsis DG et al. Circulation. 2005;111:2906-12.
Severe Obstruction (angina, no rupture) vs MildObstruction (no angina, likely to rupture)Severe fibrotic plaque Severe obstruction No lipid Fibrosis, Ca2 Exertional angina ( ) ETTRevascularizationAnti-anginal RxVulnerable plaque Minor obstruction Eccentric plaque Lipid pool Thin capCoronary Stenosis prior to MI 4 studies of angiogramsbeforeandPlaquerupture Acute MIafter MI Unstable angina 68% had 50% stenosis;18% 50 Sudden death70% stenosis preceeding MIFalk et al. Circulation. 1995;92:657-671Green Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZPharmacologic stabilizationEarly identification of high-risk?Courtesy of PH Stone, MD.
Optimal Medical Therapy in stable ischemicheart diseasePharmacologicLifestyle Smoking cessation Antiplatelet Aspirin Physical activity P2Y12 inhibitors Nutrition Weight control DietAnti-lipid Statin Other ACE Inhibitor/ARB Beta-blocker Calcium channel blocker Long-acting nitrate Ranolazine
Era of intensive medical therapyLandmark trials COURAGE BARI 2DGreen Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ
Stable Ischemic Heart DiseasePCI Did Not Reduce Death or MIOptimal Medical Therapy (OMT)1.018.5%0.90.8PCI OMT19.0%Hazard ratio: 1.0595% CI (0.87-1.27)P 0.620.70.60.50.001Number at RiskMedical 91017101395995283483333% PCI rate in OMT; 21% repeat PCI in PCI groupGreen Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZBoden et al NEJM 2007
Stable Ischemic Heart DiseaseSurvival was similar in the two groupsPCI OMT1.00.9OMT0.80.7Hazard ratio: 0.8795% CI (0.65-1.16)P 0.380.60.50.0Number at RiskMedical TherapyPCI01234567Years113811491073109410299171051 929717733Green Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ4684883023123844Boden et al NEJM 2007
Prompt revascularization did not improve survivalin diabetic patients with SIHDBARI 2DMed group –revasc 19% year 1, 42% by year 5Green Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZBARI 2D Study Group. N Engl J Med2009;360:2503-2512.
BARI 2D Survival Endpoint by Revascularization ModePCI vs. CABG NOT RandomizedBARI 2D Composite Secondary Endpoint (death/MI/CVA) in CABG Stratum; reducedBARI 2D Study Group,due to fewer MIs. No systematic assessment of peri CABG MINEJM 2009
New Zealand 2012 Guidelines for the Managementof Non ST-Elevation Acute Coronary SyndromesOxygen therapy Oxygen therapy is indicated for patients with hypoxia(oxygen saturation 93%) and those with evidence ofcardiogenic shock, to correct tissue hypoxia IIa In the absence of hypoxia, the benefit of oxygen therapy isuncertain, and in some cases oxygen therapy may beharmfulGreen Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ
New Zealand 2012 Guidelines for the Managementof Non ST-Elevation Acute Coronary SyndromesAspirin Aspirin 150-300mg, 1A Long-term, lower doses of enteric coated aspirin 75100mg should be given indefinitelyGreen Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ
The RISC trialLow dose aspirin 75 mg o.d. in non-STE ACS0.25Placeboof Death or MIProbability0.20Risk ratio 0.520.1595% CL 0.37-0.720.10Aspirin 75 mg0.050.00036MonthsGreen Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ912Wallentin L et al. Lancet 1990; JACC 1991;18:1587-93.
Effect of aspirin on cancer deaths in51 trials (77,549 participants)Number of deathsAspirinControlOdds Ratio(95% CI)0- 2.9 years2923250.90 (0.76 – 1.06)0.183.0 - 4.9 years1611730.93 (0.75 – 1.16)0.51 5 years921450.63 (0.49 – 0.82)0.0005Unknown1721--Total5626640.85 (0.76 – 0.96)0.008PCancer death only**Cancer death or non-vascular deaths if cancer data were unavailableRothwell P, et. al Lancet 2012: 379:1591
Effect of aspirin on risk of metastasisRothwell P, et. al Lancet 2012: 379:1591
Aspirin benefit vs harm Prevention of GIT cancers vastly outweighs risks ofmajor bleeds in those at low cardiovascular risk Aspirin could be started at a low dose of 75mg perhapsin the early 50’s to allow for both the early and delayedanticancer benefitFox, White, Gersh, Opie; Drugs for the Heart 2013
Should aspirin be dropped? Aspirin was shown in the AntithromboticTrialists’ Collaboration in patients with prior MIto reduce MI, stroke, or vascular death by 25%over two and a half years Increase in 1-3 per thousand in major bleeds,mostly gastrointestinal And may reduce cancer and cancermetastases by 15%Green Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZATTC (including White HD) Lancet.
What happens if aspirin is stopped? Potential consequences of unopposedthromboxane-dependent plateletactivation after stopping aspirin Discontinuation of low-dose aspirin insecondary prevention resulted in a 40%increase in MI and stroke as comparedwith continuationGreen Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZGarcia Rodriguez LA, et al. Neurology.2011;76:740-6;
Should aspirin be dropped? Aspirin is effective and cheap There is only one small trial and the WOESTauthors concluded: “we agree that furtherstudies are needed on this topic and this isat least hypothesis generating for the future” Further studies are needed before we canconclude that aspirin can be stopped inpatients who are taking anticoagulants for AFand who have been stented and are on a P2Y12inhibitorGreen Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ
Ticagrelor: does not require hepaticmetabolism for activationTicagrelor:Does NOT require metabolic activationto become active e iate metaboliteProdrugClopidogrel:A prodrug; requires metabolism tobecome active drugGreen Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZAdapted from Schomig A. N Engl J Med. 2009;361:1108–1111.
Cumulative incidence (%)PLATO: primary endpointK-M estimate of time to major CV event(composite of CV death, MI or lorNNT 54(HR, 0.84; 95% CI, 0.77-0.92; P 0.001)024681012Months after randomizationNo. at rel9291852183628124665050964047Green Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ.K-M , Kaplan-Meier
PLATO: hierarchical testing of majorefficacy endpointsTicagrelor(n 9333)Clopidogrel(n 9291)HR for ticagrelor(95% CI)P value†CV death MI stroke864 (9.8)1014 (11.7)0.84 (0.77-0.92) 0.001Secondary endpoints, n (%/yr)Total death MI stroke901 (10.2)1065 (12.3)0.84 (0.77-0.92) 0.0011290 (14.6)1456 (16.7)0.88 (0.81-0.95) 0.001MI504 (5.8)593 (6.9)0.84 (0.75-0-95)0.005CV death353 (4.0)442 (5.1)0.79 (0.69-0.91)0.001Stroke125 (1.5)106 (1.3)1.17 (0.91-1.52)0.22Death from any cause399 (4.5)506 (5.9)0.78 (0.69-0.89) 0.001All Patients*Primary endpoint, n (%/year)CV death MI stroke severe recurrent ischemia recurrent ischemia TIA arterial thrombus*The percentages are K-M estimates of the rate of the endpoint at 12 months. Patients could have had more than one type of endpoint. Death from CVcauses and fatal bleeding, as only traumatic fatal bleeds were excluded from the CV death category. Death from any cause was tested after stroke, whichwas nonsignificant, so the results should be considered nominally significant; †By Cox regression analysis using treatment as factor.Green Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZWallentin L, et al. N Engl J Med. 2009;361:1045-1057.
PLATO Unexplained findingsMortality Play of chance? Less bleeding translates into reduced mortality? Modest reduction in MI compared to reduction in mortalityNon-CABG bleeding is increased with ticagrelor in PLATOAdenosine-like effect? Mechanism for benefit of adenosine-like effect on mortality isunclear Related to infarct size? (prevention of MI is modest)Reduction in heart failure? (data lacking on size of MI, or incidence of, ormortality from heart failure)Arrhythmic death? (incidence of sudden death not reported)Higher Inhibition of platelet aggregation?Green Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ
PLATOCABG and Non CABG Major Bleeding*NSNSK-M estimated rate (% per year)13121110911.64.511.611.23.8NonCABGP 0.006NonproceduralP 0.037.982.8763.1NS11.22.37.72.2NonCABGP 0.03P NSP NS547.47.9CABGP grelPLATO Major BleedingTicagrelor/clopidogrelTIMI Major BleedingTicagrelor/clopidogrelPLATO Major Bleeding*Both groups included aspirin; Patients may be counted in more than 1 bleeding event category. The graded areas in the middle of the columnsrepresent patients with both a CABG bleed and a non-CABG bleed, or both a procedural bleed and a nonprocedural bleed; NS, not significant;CABG, coronary artery bypass graft; K-M, Kaplan MeierGreen Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ
DyspnoeaDyspnoea was reported more frequently by patients onticagrelor than clopidogrel (13.8% vs 7.8%; P 0.001)Most episodes lasted less than a weekTicagrelor-associated dyspnoea was mostly mild tomoderate and did not affect efficacy1 in 90 patients discontinued study drug because ofdyspnoea (0.9% vs 0.1%, P 0.001)The higher frequency of dyspnoea with ticagrelor was notassociated with any detectable detrimental effect onpulmonary or cardiac function (compared withclopidogrelGreen Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZWallentin L, et al. N Engl J Med. 2009;361:1045-1057;Storey R, et al. JACC. 2010;55(Suppl 1):A108.E1007.
How do you transition fromclopidogrel to ticagrelorBegin ticagrelor without aloading dose 90mg bid onthe next dayGreen Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ
Impact for patientsBased on 1,000 patients admitted to hospital for ACS,using ticagrelor instead of clopidogrel for 12 monthsresulted in 14 fewer deaths11 fewer myocardial infarctions6–8 fewer cases with stent thrombosis6 more major non-CABG bleeds but no increase in fatal orlife threatening bleeds9 patients may switch to thienopyridine treatment becauseof reversible symptoms of dyspnoeaTreating 54 patients with ticagrelor instead of withclopidogrel for one year will prevent one event of CVdeath, MI or stroke and treating 71 will reduce one deathGreen Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ
New Zealand 2013 Guidelines for the Managementof ST-Elevation Acute Coronary SyndromesP2Y12 Inhibitors Ticagrelor is the preferred P2Y12 inhibitor and should begiven at presentation in all patients with ST-elevation MIundergoing primary PCI, with a 180mg loading dose, evenin patients who have already received clopidogrel, andthen 90mg bid for a year. Class 1;Level of evidence B Administration of Ticagrelor should be started 24 hoursafter beginning fibrinolysis with a loading dose of 180 mgand continued 90mg bid for a year. Class IIa; Level ofEvidence CST-Elevation myocardial infarction Guidelines Group and the Cardiac Society of NZNZMJ 2013 ;126:127-64Green Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ
Outcomes over 1 Year for 10,000 Patientswith Prior MIIrreversible DamageTicagrelor 90 mg bidTicagrelor 60 mg bidP value Ticagrelor 90 mgTicagrelor 60 mg0.0080.0040.150.07An Academic Research Organization ofBrigham and Women’s Hospital and Harvard Medical School0.010.030.140.030.430.47 0.001 0.001Events extrapolated from 3-yr KM rates from ITT populationP values based on Cox regression
Lower LDL is Better Pravastatin or Atorvastatin Evaluation and Infection Therapy–Thrombolysis in Myocardial Infarction 22 (PROVE IT-TIMI 22)Cannon et al N Engl J Med 2004;350:1495-504Green Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ
New Zealand 2012 Guidelines for the Managementof Non ST-Elevation Acute Coronary SyndromesLipid modifying therapy Initiation of high dose statin therapy (e.g.:atorvastatin 80mg) should be commenced onadmission in all ACS patients in order to enhanceadherence and to reduce events Class 1; Level ofEvidence B Administration of a high dose statin is reasonablebefore PCI to reduce the risk of periprocedural MIClass II; Level of Evidence ANon-ST-Elevation myocardial infarctionGuidelines Group and the Cardiac Society of NZNZMJ 2013 ;125: 1-26Green Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ
Study DesignPatients stabilized post ACS 10 daysLDL 125*mg/dL (or 100**mg/dL if prior lipid-lowering Rx)Double-blindASA Standard Medical TherapySimvastatin 40 mgN up to 18,000Eze/Simva 10/40 mgFollow-Up Visit Day 30, Every 4 Months*3.2mM**2.6mMDuration: Minimum 2 1/2 year follow-up (5250 events)Primary Endpoint: CV Death, MI, Hospital Admission for UA,revascularization ( 30 days after randomization), or StrokeGreen Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ
Ezetimibe: background Ezetimibe inhibits Niemann-Pick C1-like 1 (NPC1L1)protein located primarily on the epithelial brush borderof the GI tract resulting in reduced cholesterol absorption When added to statin, produces 20% furtherreduction in LDL-C Two recent human genetic analyses have correlatedpolymorphisms in NPC1L1 with lower levels of LDL-Cand lower risk of CV events**MI Genetics Consortium Investigators NEJMGreen Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ2014; online Nov 12; Ference BA et al AHA2014
Patient populationInclusion Criteria: Hospitalization for STEMI, NSTEMI/UA 10 days Age 50 years, and 1 high-risk feature: New ST chg, troponin, DM, prior MI, PAD, stroke,prior CABG 3 years, multivessel CAD LDL-C 50-125 mg/dL(1.4-3.5 mmol/L), (50–100 mg/dL if prior lipidlowering Rx)Major Exclusion Criteria: CABG for treatment of qualifying ACS Current statin Rx more potent than simva 40mg Creat Cl 30mL/min, active liver diseaseGreen Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ
LDL-C and lipid changes1 Yr Simva53.2125.8120.448.73.3Δ in mg/dL-16.7-19.3-16.7 0.6-0.5Median Time avg69.5 vs. 53.7 mg/dL
Primary endpoint — ITTCardiovascular death, MI, documented unstable angina requiringrehospitalization, coronary revascularization ( 30 days), or strokeHR 0.936 CI (0.887, 0.988)p 0.016Simva — 34.7%2742 eventsNNT 50EZ/Simva — 32.7%2572 events7-year event rates
Individual cardiovascularendpoints and CVD/MI/StrokeAll-cause .8714.813.10.002Stroke0.864.84.20.052Ischemic stroke0.794.13.40.008Cor revasc vaBetterSimva* EZ/Simva* p-value15.315.40.782*7-yearevent rates (%)
ACS: 2014 Conclusions Incidence of STEMI is falling and non STEMI isincreasing; as troponins become more sensitiveunstable angina is disappearingACS patients still have a significant incidence ofcomplications including death, recurrent myocardialinfarction and strokeManagement can be improved substantially byusing evidence based treatments in secondarypreventionGreen Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ
“Science tells us what we can do;Guidelines what we should do;Registries what we are actually doing.”Green Lane Cardiovascular Service, Auckland City Hospital, Auckland, NZ
VA study CASS study European study All studies P 0.12 5 yrs P 0.45 10 yrs P 0.001 5 yrs P 0.02 10 yrs P 0.25 10 yrs P 0.001 5 yrs P 0.03 10 yrs n 354 n 332 n 373 n 394 n 390 n 390 n 1,325 n 1,324 No CABG CABG Yusuf et al. Lancet 1994;344:563-570. Relevance today is unclear. There was minimal or no use of effective medical therapy (ASA, statins .