Transcription
Basic ECG & ArrhythmiasDamrongg Sukitpunyaroj,p y j, MD
ECG 12 lead ECG ECG strip(Rhythm strip)
ECG 12 leadl d ECG– Completeinformation Rate, rhythm, axis,hhypertrophy,t hischemia,miscellaneous– Takes more time– May not obtainedfrom telemetrymonitor ECG stripti– Limited information RRate,t rhythm,h th Ischemia– Easy to get Monitor : Telemetry,Defibrillator– Longer strip givemore informationabout rhythm rhythm strip
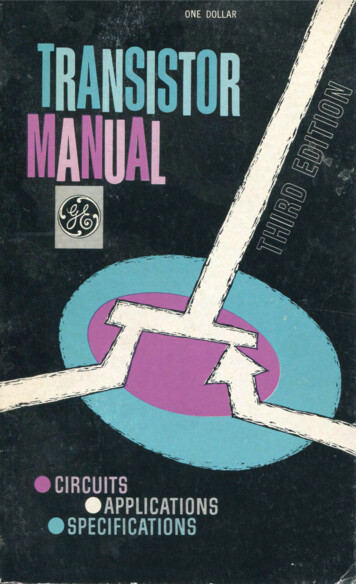
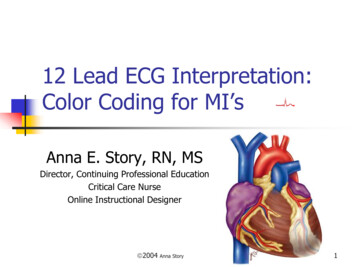
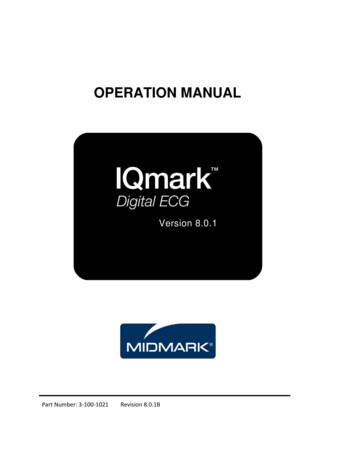
Cardiac CycleRPPRQSSSTTQT intervalP wave: Atrial contraction ( 2.5 small box)PR interval: AV conduction time ( 1 large box)QRS complex: Ventricular depolarization( 3 small box )Twave: Ventricular repolarization
Five Aspects for ECG Reading Rate RhythmA iAxisHypertrophyInfarction
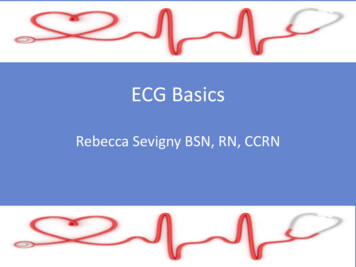
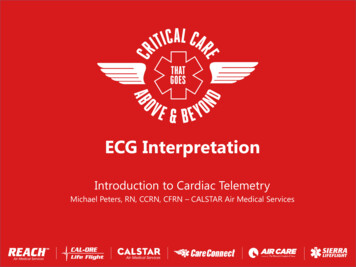
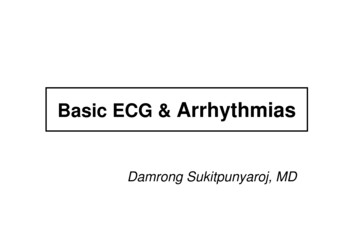
ECG Paper5 big box 1 sec0.1 mV ECG paper runs by a machine with therate of 25 mm/sec Standardization 10 mm 1 mVolt
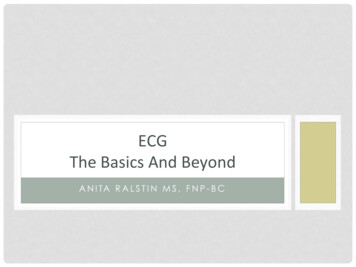
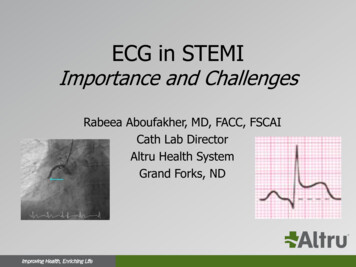
Rate 300/N 1500/nR 0 R1300 150 100 75 60 50 43กระดาษวิ่งด วยความเร็ว 25 mm ใน 1วินาที””1 ”1/ 25 0.04 ”5 ”0.04 x 5 0.20.00.”””จาก R0 ถึง R1 : 0.2 sec ได 1 cardiac cycle60 sec 60/ 0.2 300/ 1
Quick rate determination
Rate ?
Marked Bradycardiayor Total Irregularg Rhythmy3 second marks6 second stripRate Cardiac cycle in 6 second strip x 10
Rate ?
Rate ?
Five Aspects for ECGReading RateR t RhythmRh th Axis Hypertrophy Infarction
Rhythm(Arrhythmia)y(y)“ AlwaysAlMeasureMPP-RR IIntervaltl andd QRS ComplexCl ”Varying Rhythm : sinus arrhythmia, Wanderingpacemaker AFpacemaker,Extra Beats and Skips : premature beats, escapebeats, sinus arrestRapid Rhythm : PSVT, AFl, AF, VT, VFl, VFHeart Blocks : SA blockk, AV block, BBB
การอ านจังหวะการเต �การเตนหวใจ ต องมองหา P waves และ QRS complexes– Rate– Regular or Irregular– MorphologyM h l �นธ ระหว าง P waves และ QRScomplexes - PR interval
1 มองหา QRS complex1. ไม ไ เห็น็ QRS complexl– Asystole– Ventricular fibrillation(VF)– Connector problem เห็น็ QRS complex– Rate 60 Bradycardia 60-100 normal 100 tachycardia– Regularity Totally irregular Æ likelyAF– Narrow or Wide Wide QRS– Ventricular rhythm e.gVT– Pacemaker rhythm– Pre-existing BBB– Aberrant conduction– WPW
Quick Approach to Rhythm LookL k ffor QRS– No QRS identified : Asystole, VF, connector problems– QRS identifiedid tifi d Æ IdentifyId tif hheartt ratet Normal resting heart rate: 60 – 100 bpm Tachycardia: 100100 bpm Bradycardia: 60 bpm– Regular or irregular Totally irregular Æ likely AF– Wide or narrow QRS complex Wide QRS complex : Ventricular rhythm ee.g.g VT; prepre-existingexistingBBB or aberrant conduction; pre-excitation (WPW),pacemaker rhythm
Quick Approach to Rhythm Look for P wave and association of P wave to QRS (PRinterval)– P wave : not identified P wave hidden in T wave, QRS complex, small P wave No P wave with flat line : sinus arrest, sinus block No P wave with fibrillation/flutter wave: AF, A flutter– P wave: ididentifiedtifi d Is it sinus P wave? – P wave in II, III, aVF– Not sinus P wave : ectopic atrial rhythm (bradycadia or normal HR),atrial tachycardia (tachycardia) Retrograde P wave?– Junctional rhythm, SVT, VT Association of P wave to QRS -- PR interval is consistent?– No association : AV Block Vs AV dissocitation– Some associtation but not consistent : 2nd degree AVB– Consistent association but long PR: 1st degree AVB
Mechanism of CardiacArrhythmias Abnormal Impulse Formation– Increase Automaticity– Triggered Activity–Reentry Abnormal Impulsep Conduction Combination
Classification of Cardiac arrhythmiaySupraventricularin OriginSA node, Atrium,AV node, etc.VVentricularti lin Origin
Normal Sinus RhythmECGCriteria60-100 beats / minregularlupright in I, II and aVF and uniform0 12-0 20 sec and constant from beat to0.12-0.20beat5. QRS duration 0.10 sec or less1. Rate2.2 RhythmRh th3. P waves4.4 PR interval
Normal Sinus Rhythm1. ทุทกก P wavesมี QRS complexes ตามมา2. QRS แคบเป นปกติคอื ไม เกิน 0.12 วินาที3 ยะระหว างแต ละ complexes สมาเสมอสม่ําเสมอ4. P wave หวตงในหัวตัง้ ใน lead 2,3, aVF5. อัตราการเต น 60-100 ครัง้ /นาที
Sinus BradycardiaECGcriteria1. Same NSR2.2 RateR t 60 BPM
Sinus Bradycardia อาจพบในคนปกตได ใ ป ิไ โดยเฉพาะถ โ าเต นไไมช า มาก และไมมีไ อี าการใดๆใ– High vagal tone เช น นักกีฬา– Nocturnal bradycardia กรณีที่ชีพจรช ามาก เช น น อยกว า 40 ครั้งต อนาที และมีอาการจําเป นต องได �ดยเฉพาะหากเป น unstable bradycardiay– Vagovagal reflex Æ cardioinhibitory– Sinus node disease– Drug effects B-blocker, Ca blocker, antiarrhythmic ( Amiodarone, digoxin,etc)– Electrolyte imbalance, acid-base abnomality– Acute coronary syndrome– Etc.Etc
Sinus TachycardiaECGCriteria1. Same NSR2.2 Rate: greater than 100 bpm
Sinus tachycardia ��ปกตั ป สสี ป ิ �พาะไ ํ ป ัํแต ควรไปแก สาเหตุที่กระตุน หัวใจจึงจะเต นช าลงจนเป นปกติเอง เว นเสียแต ��โดยไม เหมาะสมแก ภาวะ Sinus tachycardiaสาเหตุ อาจรักษาโดยใช ยา Beta blocker ได สาเหตุที่พบบ อย Æ มีตัวกระตุ นต อ sinus node––––––– ไไข �เหนื่อยจากโรคปอด น้ําท วมปอด �รยดธัยรอยด เป ��โบลิค �ตาโบลคเช น �า ฯลฯSinus node reentry, Inappropriate sinus tachycardia Æ พบได ไม บ อย
Sinus ArrhythmiaECGCriteria11. Rate2. Rhythm3.3 Otherusually 6060-100100irregular, phasic withrespiration (increaseduring inspiration)same NSR
Sinus arrhythmia ภาวะทีคี่ ลืนื่ หัวั ใใจเหมืือน normall sinusiแต มีอัตราการเต นไม สม่ําเสมอ คือเร็วและช าโดยสัมพันธ กับการหายใจ เมือื่ ตรวจดู P wave แล ว ��ลอด พบได ในคนปกติทอี่ ายุน อย ไม จําเป นต องให การรักษา
PrematureContractionA. PACB. PJCC. PVC
Supraventricular Tachycardia(SVT) From SA node (sinus node)– Sinoatrial node reentry tachycardia (SNRT)– Inappropriate sinus tachycardia Atrial source––––Ectopic atrial tachycardia (EAT)Multifocal atrial tachycardia (MAT)Atrial fibrillation with rapid ventricular responseAtrial flutter with rapid ventricular response(Without rapid ventricular response, fibrillation and flutter are usually notclassified as SVT) Atrioventricular source (AV node)AV nodal reentry tachycardia (AVNRT)AV reciprogatingp gg tachycardiay((AVRT))Junctional ectopic tachycardia (JET)
Supraventricular Tachycardia
Nonsinus Atrial Rhythm (CS)ECGCi iCriteria11. QRS2. Rhythm3.3 P waves4. RateNormal-lookingregularnegative in II, IIII, aVFnormal, tachycardia
Nonsinus Atrial Rhythm(Atrial ectopic rhythm) จุกกําเนิดไฟฟ าเกิดจากตําแหน งอื่นใน atrium นอกSA node ECG – P wave ไมเปนบวกในไม เป นบวกใน II,III,aVF พบได ในคนอายุน อย โดยทัว่ ไปไม อนั ตรายและไม จําเป นต องรักษา
Wandering PacemakerECGCriteria1. Normal-looking QRS2. Rhythm:irregular3.3 P waves:more ththan 3 contourst
Wandering pacemaker Atrial arrhythmia ทีเี่ กดจากจุิดกําํ เนดของไฟฟ ิไฟฟ �งั ใ ั ไป sinoatrial node (SA node), atrium, and/or theatrioventricular node (AV node) ECG– �งรูปร างของ P wave (upright, flattened, notched, biphasic)มักเห็นชัดใน lead II– Ventricular conduction ปกติ ÆQRS รูปร างปกติ �แปลงขึน้ ลงของ vagal tone ( varying vagal tone)– เมืเมอ่อ vagal tone สูสงง SA node �ล อยไฟฟ าช าลง �าจากจุาให มีการปล อยไฟฟ �าาเนิดไฟฟ าสํารองจากตําแหน งอื่นในหัวใจห องบน– เมื่อ vagal tone ลดลง SA node � พบได พบไดในเดกในเด็ก คนชรา นกกฬานักกีฬา มักไม ทําให เกิดอาการและไม จําเป นต องรักษา
Multifocal Atrial Tachycardia (MAT)Common inCOPDECG CCriteriait i1. Same wandering pacemaker2. Rate 100 bpm
Multifocal atrial tachycardia ECG– P wave มีลักษณธแตกต างกันตั้งแต 3 แบบขึ้นไป– PR intervals แตกตางกนแตกต างกัน– ชีพจรเร็วมากกว า 100 ครั้ง/okmu สาเหตุุ– พบบ อยในผู ป วยสูงอายุที่มโี รคปอด เช น COPD ภาวะ hypoxemia– อาจพบในภาวะ digitalis toxicity, AMI, hypokalemia,hhypomagnesemiai การรักษา– �เหต การใหการให Oxygen �ช วยในบางราย– ถ าหัวใจเต �าให ยากลุ ม Ca blocker เช น Verapamil,etc
Atrial FlutterECGCriteriaRateatrium 250-400, ventricular varyusually 150yatrial regularg , vent mayy regg or irreggRhythmdepending on AV conductionP wave saw-toothed or “flutter” wavesPR interval not measurableQRSnormal or BBB
Atrial flutter ECG : ลกษณะลักษณ P wave คลายฟนเลอยคล ายฟ นเลื่อยหัวใจห องบนเต นผิดจังหวะ เกิจจากmacroreentry ในหัวใจห องบนขวาหรือซ ายมักพบในผูู ปว ยโรคหัวใจ แต �มหี ัวใจปกติได บ อยครั้งที่จะ degenerate เป ร atrialfibrillationอาการมักั ขึนึ้ กับั อััตราการเต นของหััวใใจห องล าง(ventricular response)– Flutter rate 300 ms 2:1 AVB Æ V rate 150 bpmp 3:1 AVB Æ V rate 100 bpm การรักษา– Rate control– Rhythm control : cardio versionversion,drug, RF ablation– Embolic prevention เหมือนAF
Atrial Fibrillation
Atrial Fibrillation เปนป arrhythmia �ูี่ โสงอายุ อาจพบรวมกบ ั sick sinus syndrom (SSS)มีส วนน อยที่ พบในคนปกติ (lone AF)ECG : ไม เห็น P wave (อาจเห็นป น fibrillatory activity) ; QRS ไม สม่ําเสมอ– VentricularV t i l ratet อาจเร็ว็ หรือื ช า ขึ้ึนกับ ventriculart i l conductiond tiAF ร วมกับ WPW syndrome Æ atrial activation ผ านสู ventricle ผ านทางbypass tract แทน AVN อาจมี ventricular rate เร็วมาก จนเกิด VF ได AF โดยทัโ ่วไปไม ไปไ ท ําให ใ ผ ปู วยเสีียชีีวิต ยกเว น AF withith WPW แต ใ นกรณีีที่ ventriculart i l ratet เร็็วมากๆ อาจทําให �่นที่เป �หัวใจล มเหลว ความดันต่ํา กระตุ นให เกิด acutecoronary syndrome เป นต นCo morbidity �ของ AF คอคือ thromboembolism (Strokes; acuteembolism)AF management– Rhythm control : CardioversionCardioversion, antiarrhythmic drugsdrugs, RFablation– Rate control– Embolic prevention
Sick sinus syndrome (SSS) SinusSiarrest– // escape junctional rhythm (slowjunctional rhythm) Sinus pause Sinus exit block Extreme sinus bradycardia– / / chronotropic incompetence Tachy-bradyarrhythmiayyy
Sinus Arrest
Sinus pause/Sinus arrest ECG– P wave หายไป 2 วินาที (10 ช องใหญ ) ทําให QRS หายไป หรือมี QRS �นิดไฟฟ าสํารอง (escape rhythm) Atrailil escape: rateAtt 60-8060 80 BPMJunctional escape : rate 40-60 BPMVentricular escape; rate 20-40No escape rhythm: asystoleเกิดจาก Sinus node (Sinoatrial node) หยุดปล อยกระแสไฟฟ � สาเหตุ – Sick sinus syndrome Fibrosis,, infiltrative disease,, ischemia– Drugs, toxicity– Electrolyte imbalances– High vagal tone – carotid massagemassage, vagal maneuvermaneuver, vagovagal/vasovagal reflex (cardioinhibitory type)
Escapep Beat
Junctional Rhythm
Junctional Bradycardia
Sinus exit block
Sinus Exit Block ECG–PP wave หายไปไป Æ QRS หายไปไป–แยกจาก sinus ppause โดยสังเกตจากุ ppauseinterval จะเป นจํานวนเท า (2x, 3x,4x, ) ของPP interval ก อ นหน า �น Sinus pause/arrestp
Tachy-bradycardia Syndrome
AV conduction abnormality FirstFi degreedAV blblockk Second degree AV block– Mobitz I– Mobitz II– 2:1 AV block (high grade AV block) ThirdThi d ddegree AV blblockk (C(Completel t AVpheart block))block, complete
Types of AV block
First Degree AV BlockCriteria Prolong PR interval 0.20 sec
First degree AV block ECG : PR interval 0.20 2 sec (200 msec) Common causes––––––Normal variant ((incidence 0.6 -1.1% in normal ppopulation)p)Enhanced vagal tone Ie.g. atheletes)MedicationElectrolyte imbalanceAV conduction diseaseMyocarditis, AMI etc. Management– Identifying and correcting electrolyte imbalande– Witholding the offending medication Prognosis– Isolated first degree AV block – no direct clinical consequences
Second Degree AV Block, Mobitz I
Second degree AV block, Mobitz I(Wenckebach) ECG : PR interval ต อยๆยาวขึ้จนเกิด droppedQRS complex �ังจากนัน้ ก็จะมีการ reset ของPR interval กลับมาสั้นล วค อยๆยาวขึ้นอีกเป นวงจร(Wenckebach cycle) ส วนใหญ เกือบทั้งหมดเป น benign condition และไม ต อ งการ specificifi ttreatmenttt
Second Degree AV Block, Mobitz II
Second degree AV blockblock, Mobitz II ECG : Dropped QRS (blocked P wave)a e) เป ป นช วงๆ โดยที่ P wav มาสม่ําเมอดี และไม มีการยาวขึ้นของ PRintervals กอนทก อนที่ QRS complexes หายไป เกือบทัง้ �ปกติของ AV conduction ส วนปลาย (infrahisian block) ความสําคัญ:– มีโี อกาส progress เป ป น completel t AV blockbl k ได ไ ใ นระยะเวลาอันสั้น Æ syncope, cardiac arrest หรือsudden cardiac death– เป นข องบ งชี้ในการใส Pacemaker
Rate, rhythm, axis, hth Rate, rhythm, Ischemia – Easy to get h yper trop h y, ischemia, miscellaneous Easy to get Monitor : Telemetry, Defibrillator – Takes more time – May not obtained – Longer strip give more information May not obtained about rhythm from telemetry monitor about rhythm rhythm strip