Transcription
5/1/22Innovations inGlaucomaNext Generation Technology,Medications, and DeliveryJustin Schweitzer, OD, FAAOVance Thompson Vision, Sioux Falls, South DakotaOptometric Externship DirectorAssociate Director Residency Program1Financial Disclosure – Justin Schweitzer, OD, FAAO Aerie – C/LAlcon – C/LAllergan – C/LBausch Lomb – C/LOcular Therapeutix - CEyePoint - CDompe – CZeiss – C/L Sun – C/LEquinox - IReichert - CJ&J – C/LGlaukos – C/LHorizon – CQuidel – CSight Sciences – C/LLKC - C Co-Chief Medical Editor: Modern Optometry3Today’s Optometrists“To be on the cutting edge ofoptometry, you need to be on thecutting edge of science andtechnology.”41
5/1/22CornealThicknessSLTCornealHysteresisGlaucoma MedicationsMIGSONH AppearanceGlaucomaIOPOCTFiltration SurgeryFamily HistoryVisual FieldDrug Delivery Devices5Case 71-year-old AfricanAmerican male Medical History: HTN Family History: HTN,DM BCVA: 20/20 1 OU IOP(CATS): 29 mm Hg OD; 26 mm Hg OS IOP (IOPcc): 28.7 mm Hg OD; 27 mm Hg OS IOP (g): 23 mm Hg OD; 22 mm Hg OS C/D: 0.80/0.80 OD 0.65/0.65 OS Pachymetry: 510 OD; 514 OS Corneal hysteresis: 8 OD 8.9 OS Gonioscopy: Open to CB OU w/ tracepigment in TM SLE: Unremarkable VF’s – See next slide OCT’s – See next slide6OCT’s72
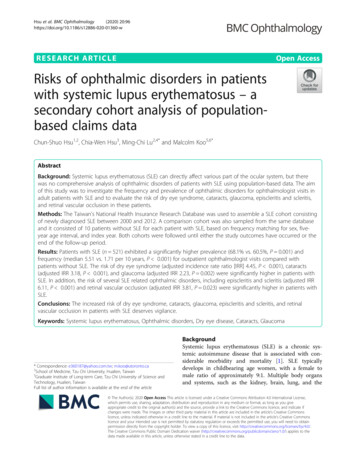
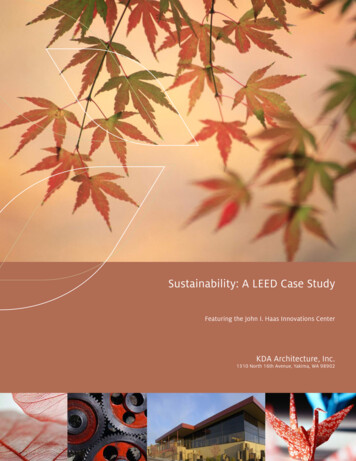
5/1/22Visual Field’s8Case Conclusion Start a Prostaglandin OU IOP 17 OD; 16 OS @ 6 weeks Monitoring the patient every 4 months initially Recent visit – stable VFT, OCT, and IOP (schedule q 6 mos)10IOP Matters30Baltimore Eye StudyPrevalence (%)Of POAG2502001501005000 15016-18019-21022-240IOP25-29030-340 350Sommer et al. Arch Ophthalmol. 1991.113
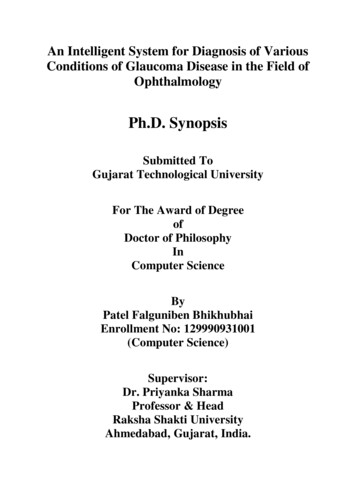
5/1/22The Correcting Applanation Tonometer Surface (CATS)12The Correcting Applanation Tonometer Surface (CATS)13IOP “corneal-compensated” (IOPcc)213 Eyes of 125 glaucomatous patients followed for 2.4 yearsGATORA11.1% (.11)24.5% (.24)RBT5.8%% (.05)Susanna BN, Ogata, NG, Daga FB et al. Association between Rates of Visual Field Progression and IntraocularPressure Measurements Obtained by Different Tonometer's. Ophthalmology. 2019 Jan;126(1): 49-54.144
5/1/22Case84-year-old, Caucasian femaleOcular HistoryDiagnosed with POAG – 2012-2014OD – latanoprostene bunod 0.024% qd, brimonidine tartrate/timololmaleate 0.2%/0.5% bid, brinzolamide bidOS – history of tube shunt, no current medicationsCataract extraction: 2009 OUFamily History: POAG - Father15Ocular Exam:VAcc: OD – 20/20 OS – 20/40Tmax IOP: OD – 24 mmHg OS – 28 mm HgSLEX: Tube shunt OS, otherwise unremarkableONH: OD – 0.80/0.80 OS – 0.95/0.9516Ocular Exam:Pachymetry: 510 OUGonioscopy: Open to CBIOP History:OD – consistently 10-12 mm HG (on medications)OS – consistently – 10-11 mm HG (tube shunt)175
5/1/221819Home IOP MonitoringA device is intended as anadjunct for monitoring IOP ofadult patients (self-use). TheHOME tonometer is designedfor use at home or on the go.206
5/1/22Case Summary:Subconjunctival Stent21Continuous IOP Sensors22Implandata Eyemate Sulcus based IOP sensor8 pressure-sensitive capacitorsDiameter: 11.2 mmThickness: 0.9 mm237
5/1/22ARGOS-02 Trial: 1 year results 22 Patients Major Design Changes:– 0.9 to 0.5mm thickness with 0.1mmrounded tapering– 4 haptics to prevent cilliary sulcus rotation IOP Concordance:– D30: Eyemate: 22.2 9.2 mmHg GAT: 19.5 6.8 mmHg– D360: Eyemate: 15.7 3.8 mmHg GAT: 14.1 2.2 mmHgAmerican Journal of Ophthalmology DOI: (10.1016/j.ajo.2019.09.011)24Sensors on the horizon LaunchPoint Technologies (Goleta, CA)– Sensor attached to IOL or injected into vitreousIntraocular Pressure Sensor. Launchpoint Technologies. Available at: aocular-pressuresensor . Accessed 10-23-201825Sensors on the horizon AcuMEMS (Menlo Park, CA) iSense System: implantable sensor Glaukos (San Clemente, CA) DOSE Medical IOP Sensor Implandata Ophthalmic Products GmbH Suprachoroidal IOP sensor Injectsense Inc (Emeryville, CA) Configurable on-demand sensor LaunchPoint Technologies (Goleta, CA) Sensor attached to IOL or injected into vitreous Solx (Waltham, MA) wireless intraocular sensor268
5/1/22Corneal Hysteresis, IOP, CCT27Corneal HysteresisCorneal Hysteresis reflects the ability of the corneal tissue to dissipateenergy 1Function of viscoelastic damping2Two predictive functions1. Which glaucomatous eyes are most susceptible to visual field lossprogression and risk of rate of progression?2. Which eyes are susceptible to glaucoma?1. Luce DA. J Cataract Refract Surg.2005;31:156-162.2. Dupps WJ Jr. J Cataract RefractSurg. 2007;33:1499-1501 .28Average CH in Normal SubjectsNCHBrazil10510.1 /- 1.8UK27210.2 /- 1.2China12510.9 /- 1.5Japan20410.2 /- 1.3Spain8810.8 /- 1.5USA4410.5 /- 1.2299
5/1/22CH as a Predictor of ProgressionMedeiros FA et al. Ophthalmology.2013;120:1533-1540.30460 eyes of 334 glaucoma patientsFollow-up – 4.3 yearsWell controlled if IOP 18 mm HG179 eyes well controlled42 (23.5%) of those eyes had VF progressionCH (8.6 vs 9.4)CCT (515 vs 531)68% higherrisk of progression31OCTPay attention to TSNIT curve.Pay attention to the actual numbersin the segmentation plotPay attention to the numbers betweeneyes in the segmentation plot3410
5/1/22Intereye (OD/OS) macular thicknessasymmetry 5 micronsIntraeye (sup/inf of same eye)macular thickness 9 micronsIntereye (OD/OS) average RNFLthickness 9 micronsTotal RNFL thickness 78 micronsor less35OCT Technology – Matching Structure and Function36The Role of Ganglion Cell ImagingSpectralis - maculaOptovueCirrus OCT3711
5/1/2238Resulting SITA Faster 24-2C Pattern on HFA3Large Gray24-2 patternLight Blue DotsTen additional24-2C pointsSmall W hite10-2 pattern3930.4% shorter than SITA Fast53.5% shorter than SITA Standard4012
5/1/22Objective Visual Field TestingFDA 510(K) ClearedTests OU simultaneously in 7 minutesMeasures the response of the pupils to a stimulusobjectiveFIELD41The Future of Visual Field Testing?42OCT Angiography: the Next Chapter? Images retinal microvasculature without dye injection Displays structure and function from a single imaging system2014: OCTA2006: Spectral DomainOCT2002: Time Domain OCT4313
5/1/22Trend AnalysisImage courtesy of Eric D. Nudleman, MD and Michael H. Goldbaum, MD of Shiley Eye Institute, University of California at San Diego, La Jolla, CA44Evaluation of an AI system for the automateddetection of glaucoma from stereoscopicoptic disc photographs: the EuropeanOptic Disc Assessment Study Objectives - To evaluate the performance of a deep learning based ArtificialIntelligence (AI) software for detection of glaucoma from stereoscopic optic discphotographs, and to compare this performance to the performance of a large cohortof ophthalmologists and optometrists. Results– Pegasus was able to detect glaucomatous optic neuropathy with an accuracy of 83.4%(95% CI: 77.5–89.2)– This is comparable to an average ophthalmologist / optometrist accuracy of 80.5% / 80%respectively (95% CI: 67.2–93.8) / (95% CI: 67–88) on the same images.– There was no statistically significant difference between the performance of the deeplearning system and ophthalmologists or optometrists.Rogers, TW, Jaccard, N., Carbonara, F. et al. Eye 2019. DOI:10.1038/s41433-019095190345Genetics of GlaucomaKey Points Ultimately, it allows for a more personalizedpatient management treatment algorithm Understanding the genetic basis of various forms of POAG glaucoma provides anopportunity for targeting specific genes or biological pathways for disease. By genetic testing it may be possible in the future to provide personalizedtherapeutic plans for a given patient based on knowledge of their specific genemutations and the molecular pathways they impact Patients with gene variants in mitochondrial genes may benefit from antioxidanttherapies, whereas patients with mutations in lipid metabolism genes maybenefit from cholesterol lowering medications. JAMA Ophthalmol.2019;137(7):756-765. doi:10.1001/jamaophthalmol.2019.0900Avellino’s test will haveMonogenic & PolygenicPOAG formsEarly Onset monogenic forms: Juvenile open-angleglaucoma Congenital glaucoma Anterior segmentdevelopmental syndromeAdult Onset polygenic forms: Primary open-angleglaucoma(POAG) Angle-closure glaucoma(ACG) Low tension glaucoma(LTG) Exfoliation glaucoma4614
5/1/22Treatment47Delivering Treatment48latanoprostene bunod 0.024% (Vyzulta)4915
5/1/22Nitric OxideEndogenous in the humanbodyCauses alterations inthe cytoskeletal networkReduced NO in TM,Schlemm’s canal, andciliary muscleNathanson JA et al. Alterations of ocular nitric oxidesynthase in human glaucoma. Invest Ophthalmol Vis Sci. 199550VOYAGER Studylatanoprostene bunod 0.024% (Vyzulta)JUPITER Studylatanoprostene bunod 0.024% (Vyzulta)51 63,893 women from Nurses’ Health Study 41,094 men from Health ProfessionalsFollow-Up StudyFindings: Compared with the lowest quintile ofdietary nitrate intake (appx 80mg/day), thehighest quintile (appx 240mg/day) wasassociated with: 21% lower risk of all POAG 44% lower risk of POAG with earlyparacentral visual field loss5216
5/1/22Neurotoxicity of BAK Exposure to BAK (0.01% or 0.1%) QD x 7 days: Decrease NFD (p 0.02 & 0.001) Decrease aqueous production (phenol red)Invest Ophthalmol Vis Sci. 2012 Apr; 53(4): 1792–1802.53BAK-Free Latanoprost Preservative-FreeFollowing instillation, micellesmix with the tear filmAs the micelles migrate toward theocular surface, they break apart, releasinglatanoprost5454netarsudil 0.02% (Rhopressa)MOAsROCKinhibitorsaqueous humor productionCorneaTrabecularmeshworktrabecular outflowepiscleral venous pressureSchlemm’s canalEpiscleral veinsUveoscleral outflowProstaglandin analogsAlpha agonistsLensBeta blockersAlpha agonistsCAIsCiliary processesPUB-01215517
5/1/22netarsudil 0.02% (Rhopressa)56netarsudil 0.02% (Rhopressa)Conjunctival Hyperem ia50 .0%45 .0% 15-20% Hyperemiaat baseline40 .0%35 .0%30 .0%25 .0%6% dropout rate forhyperemia20 .0%15 .0%10 .0%5.0 %0.0 %Mi l dMo d erate o r Sev ereMi l dMo d erate o r Sev ereNon eNon eSerle et al. Am J Ophthalmol. 2018; 186;116-12757netarsudil 0.02% latanoprost 0.005% (Rocklatan)8775PATIENTS, % RHO protein kinase(destabilizes actin in TM) Rock inhibitor(lowers EVP) Latanoprost(uveoscleral outflow) Net Inhibition75565362433733312414 20% 25% 30% 35%1769 40%IOP REDUCTION FROM BASELINE, %Netarsudil 0.02% latanoprost 0.05%Netarsudil 0.02%Latanoprost 0.05%Pooled Mercury 1 and Mercury 2 DataMean IOP reduction at 3 months5818
5/1/22netarsudil 0.02% latanoprost 0.005% (Rocklatan)Conjunctival Hyperemia60 .0% 15-20% Hyperemiaat baseline50 .0%40 .0%30 .0%15% Corneal Verticillata20 .0%10 .0%10.6% Conjunctival Heme0.0 %Mi l dMi l dMo d erate o r Sev ereMo d erate o r Sev ereNon eNon e59Omidenepag Isopropyl (OMDI)Selective, non-prostaglandin, prostanoid EP2 receptor agonistMechanism of Action: Increase outflow via both conventional and uveoscleralPhase 3 AYAME StudyOMDI 0.002% vs latanoprost 0.005%qd dosing x 4 weeksBaseline IOP 24 mm HgOMDI 25.1% reduction (17.81 mm Hg)Conjunctival hyperemia 24.5%60Innovations in Glaucoma Drug DeliveryWhat the Future Holds6119
5/1/22More than 90% of patients arenonadherent to their ocular medicationdosing regimens, and nearly 50%discontinue taking their medications before6 months1Nordstrom BL. Persistence and adherence with topical glaucoma therapy. Am J Ophthalmol.2005;140:598-59663Dennis, P. (2011, October 10). Adverse Effects, Adherence and Cost–Benefits in Glaucoma Treatment. European Ophthalmic Review.64Iridocorneal Angle1. Travoprost IntraocularImplant (Glaukos)Ocular Surface Devices1. Contact Lenses2. Microdose latanoprost (EyeNovia)3. IontophoresisInjectable Systems1. Bimatoprost SR (Allergan)2. Travoprost IntracameralImplant (OTX)3. Travoprost ExtendedRelease Implant (Aerie)Conjunctival Cul-de-Sac/Fornix1. Bimatoprost Ring (Allergan)Punctal Plug Devices1. Travoprost Intracanalicular Insert (OTX)2. Latanoprost and Travoprostpunctal plug delivery system (Mati)6520
5/1/22Patients Attitudes Towards Drug DeliveryTriple Combination Eye Drop – 85%Microdose Eye Spray – 54%Drug-eluting Contact Lens – 31%Drug-eluting Periocular Ring Insert – 43%Injectable Subconjunctival Drug Insert- 32%Injectable Anterior Chamber Implant – 30%Wang BB., Lin MM., Nguyen, T., et al. Patient attitudes towards novelglaucoma drug delivery approaches. Digit J Ophthalmol. 2018; 24(3): 16-2366Microdose latanoprost(EyeNovia)Delivers microdoses of latanoprost with Optejet deliveryAdvantages: 75% less drug and preservative88% of the time got to targetAchieved 29% IOP lowering from baselinein Phase 2 studyPasquale, LR, Shan L, Weinreb RN, et al. Latanoprost with high precision,Piezo-print microdose delivery for IOP lowering: clinical results of thePG21 study of 0.4 micrograms daily microdose.67Drug-Eluting Contact LensAttractive option secondary tolarge residence time in the eyeand upward of 50% bioavailabilityin comparison with eye dropformulations.Li, CC, Chauhan, A. Modeling ophthalmic drug delivery bysoaked contact lenses. Ind Eng Chem Res 2006; 45: 3718–3734.Peng, C-C, Kim, J, Chauhan, A. Extended delivery of hydrophilicdrugs from silicone-hydrogel contact lenses containing Vitamin Ediffusion barriers. Biomaterials 2010; 31: 4032–4047.6821
5/1/22Punctal Plug Delivery System(Mati Therapeutics)Latanoprost and Travoprost designsU.S. Phase II Multi-center Trials (Lower Puncta)Glau 12 (n 92) – 96% retention rateGlau 13 (n 87) – 92% retention ratePhase II Clinical StudyL-Evolute - 5.5 mmHg IOP lowering over 12 weeks studyDrug CorePolymer SleeveCyanoacrylate Film71Travoprost Intracanalicular Insert(Ocular Therapeutix)Bioresorbable sustained-release intracanalicular insertDesigned for continuous steady release of travoprost tothe ocular surface for up to 90 daysPreservative freeAllows visualizationLow Ocular Adverse Events:Dacryocanaliculitis – 8.3%Lacrimal structure disorder – 6.6%72Travoprost Intracanalicular Insert(Ocular Therapeutix)Phase III randomized, double-blind, placebo-controlled clinical trialReduction in IOP2 WeekDiurnal Time Points8:00 AM10:00 AM4:00 PMn 334 OTX-TP6 Week12 Weekmm 3.23-3.14-3.91-3.34-3.27-3.52-2.63-2.60n 211 Vehicle7322
5/1/2274Bimatoprost SR (Allergan)(10-microgram bimatoprost sustained-release implant) Biodegradable bimatoprost sustained-release implant FDA-approved and indicated to reduce IOP in patientswith open angle glaucoma or OHT Single intracameral administration Phase I/II/III Studies75Bimatoprost SR (Allergan)(10-microgram bimatoprost sustained-release implant)7623
5/1/227724 Month Phase I/II Clinical Trialbimatoprost pellet(6, 10, 15, or 20 micrograms)75 subjectstopical bimatoprost 0.03%Craven ER, Walters T, Christie WC, Day DG, et al. 24-Month Phase I/II Clinical Trial of Bimatoprost Sustained-Release Implant(Bimatoprost SR) in Glaucoma Patients.Drugs. 2020 Feb;80(2): 167-179.7824 Month Phase I/II Clinical Trialbimatoprost pellettopical bimatoprost 0.03%(6, 10, 15, or 20 micrograms)24 months – IOP reduction7.5, 7.3, 7.3, 8.9 mm Hg24 months – IOP reductionof 8.2 mm HgNo Rescue or Retreatment68% - 6 mos.40% - 12 mos.28% - 24 mos.Craven ER, Walters T, Christie WC, Day DG, et al.24-Month Phase I/II Clinical Trial of BimatoprostSustained-Release Implant (Bimatoprost SR) inGlaucoma Patients. Drugs. 2020 Feb;80(2): 167-179.7924
5/1/22Phase III (ARTEMIS)27% -conjunctival hyperemia10% - post administration 2 days5.4% - endothelial cell loss over 20 months5% - iritis80Travoprost Intracameral Implant(Ocular Therapeutix)Bioresorbable sustained-release implant injected into the ACGoal: Steady release of travoprost with target duration from 4 to 6 monthsPreclinical Models (beagle dogs)Steady state releasethrough 4 monthsIOP lowering of 25-30%through 4 months81Travoprost Intracameral Implant(Ocular Therapeutix)Phase 1, prospective, multi-center, open labelCohort 1 n 5(15 micrograms)Day 28 -9.1 mm Hg (n 5)Mo. 4 -7.6 mm Hg (n 4)Mo. 6 –7.5 mm Hg (n 3)*Mo. 21 - -9.3 (n 1)Cohort 2 n 4(26 micrograms)Day 28 -6.0 mm Hg (n 4)Mo. 4 -6.8 mm Hg (n 4)Mo. 6 –6.1 mm Hg (n 3)*Mo. 9 - -5.9 (n 2)Cohort 3 n 4(15 microgramsFast Degrading)Day 28 -11.5 mm Hg (n 3)Mo. 4 -13.8 mm Hg (n 2)*Mo. 6 -12.5 (n 1)8225
5/1/22Travoprost intraocular implant(Glaukos)Resides in AC angle, anchored behind TM Length:Diameter:TitaniumNon-ferrous1.8 mm0.5 mm83Travoprost intraocular implant(Glaukos)8424- Month UpdateAverage IOP reductions from baseline 7.9 mm Hg and 7.4 mm Hg in the fast and slow release arms.Average IOP reductions from baseline 29% and 28% in the fast and slow release arms.Favorable safety profile with no ECC loss, no corneal adverse events, no adverse events of conjunctival hyperemia8526
5/1/2236 Month Update1. 70% and 68% of subjects in fast and slow-release were well-controlled on feweror same medications as baseline.2. Average IOP reductions were 8.3 mmHg and 8.5mmHg in the fast and slow-release arms.86Case32 year old maleCC: LASIK evalROS: “blurred vision and haloafter working out”BCVA: 20/20 OD20/20 OSMRx: -3.25 Sph OUNo MedsIOP: 42 OD; 38 OSPachymetry: 550 OD550 OSONH Eval: 0.40 v OU929327
5/1/2294Slit Lamp Exam959628
5/1/22PRE LPIPOST LPI97Selective Laser TrabeculoplastySelectively targets and laserburns pigmented TM cells99SLT StudiesSLT vs. Prostaglandins SLT Med Study (2012) Dr. Katz @ Wills Eye in Philadelphia J Glaucoma 2012;21:460-468 SLT (100 applications over 360 degrees of TM) vs. prostaglandin analog Primary outcome - IOP Secondary outcome - # of treatment steps10029
5/1/22SLT Med Study Treatment Arms101SLT vs. Prostaglandins SLT Med Study (2012)Results:1. IOP reduction: SLT – 25.7% IOP reduction Prostaglandin – 28.3% IOP reduction 2.IOP reduced from 24.5 to 18.2 (6.3 mmHg reduction)IOP reduced from 24.7 to 17.7 (7.0 mmHg reduction)# of treatment steps: SLT group - 11% of eyes required additional SLTProstaglandin group - 27% of eyes required additional medication102Primary Outcome - Quality of Life at 3 yearsSecondary Outome – Cost, cost-effectiveness, clinical effectiveness, and safetyConclusions:No significant difference in QOL97% probability of SLT as 1st treatment being more cost-effectiveSLT at target IOP 93% of visits vs 91.3% at target for meds78.2% of SLT Drop Free @ 3 Years10330
5/1/22Steroid After Laser Trabeculoplasty (SALT)SteroidNSAID IOP Pre-Op: 23.3 mm Hg IOP Pre-Op: 23.3 mm Hg 12 week IOP check 12 week IOP check IOP lowering of 5.2 2.7 mmHg IOP lowering of 6.2 3.1 mmHgSaline Tears IOP lowering of 3 4.3 mmHg Steady state IOP 6 weeks (new baseline)Groth et al. Steroids After Laser Trabeculoplasty (SALT) Trial: Impact of Short-term Anti-Inflammatory Treatment on SLT Efficacy. Ophthalmology June 5 2019104Case Conclusion S/P laser peripheral iridotomy and SLT OU IOP 18 OD; 16 OS Stop topical medications Return for LASIK eval105Technology is nothing.What’s important is that youhave a faith in people, that they’rebasically good and smart, and if yougive them tools, they’ll dowonderful things with 1
Monitoring the patient every 4 months initially Recent visit -stable VFT, OCT, and IOP (schedule q 6 mos) 10 IOP) G 00 50 100 150 200 250 30 150 16-180 19-210 22-240 2529 30- 34 350 IOP Matters BaltimoreEyeStudy Sommeret al. Arch Ophthalmol. 1991. 11