Transcription
ObjectivesOHSUReview the impact of preventableunanticipated medical outcomesIdentify commonly used rational whichlimit actual disclosure of unanticipatedmedical outcomesDiscuss practical strategies to facilitatedisclosure and apology
My Mom’s storyOHSU“It may seem a strange principle toenunciate as the very first requirementin a hospital that it should do the sickno harm. It is quite necessary,nevertheless, to lay down such aprinciple.”Florence Nightingale, 1863
Background: Harvard MedicalPractice Study 1990OHSUAssess adverse events of hospitalizedpatients in New York, 1984Overall 3.7% of 2.7 million pts (98,609)experienced medical error 57% minimal or transient harm 17% moderate impairment 7% permanent impairment 14% deathBrennan N Eng J Med 1991
BackgroundOHSUIn 1999, the Institute of Medicine releasedthe report “To Err is Human: Building aSafer Health System”Since this report, the magnitude andimpact of medical errors have becomemore apparentTo Err Is Human: Building a Safer Health System Institute of Medicine2000.
BackgroundOHSU Preventable medical errors in the US 250,000 to 440,000 deaths a year 3rd leading cause of death after heartdisease and cancer Estimated 17 billion in direct medicalcosts; 735 billion - 980 billion ineconomic impactVan Den Bos Health Affaris 2011; Makary BMJ 2016
OHSU
Expectations of Patients andFamiliesOHSUPatients conceive of errors broadlyDesire full disclosure of harmful errors Worry that health care workers mighthide errorsGallagher JAMA, 2003Hobgood Pediatrics, 2005Matlow Arch Dis Child 2009
Expectations of Patients andFamiliesOHSUInformation patients want disclosed Explicit statement that error occurred What happened, implications for theirhealth Why it happened How will recurrences be preventedImportance of an apology
Expectations of PhysiciansOHSUPhysicians theoretically support physiciandisclosure of adverse events Patient and family trust Ethical imperative Patient safety Health provider mental healthGallagher, Arch Intern Med, 2006Stokes Emerg Med Clin North Am 2006Waite Health Law J 2005
Expectations of PhysiciansOHSUMost clinicians indicated that they woulddisclose an error to patientsBut qualitative analysis revealed thatclinicians held a nuanced definition of“disclosure” that most often did notcontain the elements desired by patientsFein J Gen Intern Med 2007
Barriers to DisclosureOHSUFear of failure in the eyes of their peersConcern that disclosure might harmpatientsFear of malpractice liabilityLack of confidence in disclosure skillsGallagher JAMA, 2009Gallagher Arch Intern Med, 2006Berlinger J Med Ethics, 2005McDonnell Ann Intern Med, 2008
Closing the Gap: Fear of FailureOHSUPhysician burnout, fatigue, and work unit safetygrades are independently associated with majormedical errors16% of surgeons who had made a “majormedical error” contemplated suicideNurse Practitioners experience “second victim”phenomenaShanafelt Arch Surg. 2011 Tawfik et al. Mayo Clinic Proceedings 2018Hay-David, Br J Oral Maxillofac Surg 2020
Closing the Gap: Fear of FailureOHSUThere are two kinds of physicians those who have been involved in a seriousincident those who will be involved in one at somepoint in the future, sometimes as a result oftheir own error, and sometimes due to thecircumstances under which they must carry outtheir workChange in Focus to Patient Safety
Closing the Gap: EthicalConcernsOHSUEthical complexities to disclosureShould I disclose: Errors with minor/transient harm? Fatal errors? Harmful errors in patients who arehopelessly ill? Other health care providers’ errors?
Closing the Gap: EthicalConcernsOHSUTrust is at the core of the patient-doctor relationshipHiding from, obscuring, or omitting facts inconversations in the face of a medical error, erodesthat trustPatient race/ethnicity, age, gender and education arenot related to preference for, or response to, disclosureFull disclosure, whether it increases malpracticeliability or not, is the appropriate ethical pathAMA Journal of Ethics 2008Hobgood Qual Saf Health Care 2008Berlinger J Med Ethics 2005
Closing the Gap: LegalConcernsOHSURisk managers in the US, Canada, the UK andEurope: up to 80% of malpractice claims areattributed to failures in communication and/or alack of interpersonal skillsPatients who have sued often cite perceptionthat truth was hidden from them as an importantmotivatorsHuntington Proc (Bayl Univ Med Cent) 2003Joint Commission 2006Helmchen 2010
Closing the Gap: LegalConcernsOHSUThough only 49% of physicians stronglyagreed that serious errors should bedisclosed, 70% of risk managers stronglyagreedLoren Jt Comm J Qual Patient Saf. 2010
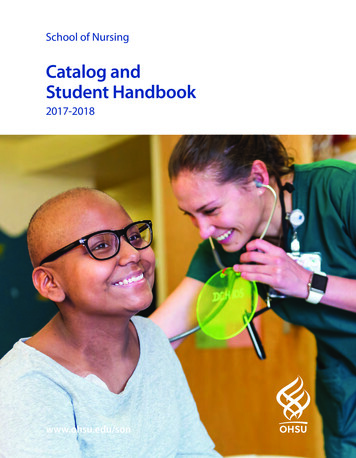
Closing the Gap: LegalConcernsOHSUSome lawmakers have attempted toencourage physician disclosure andapology through legislative effortsMany states have moved forward withdisclosure mandates and laws that protectapologies from being consideredexpressions of legal liabilityClinton N Engl J Med 2006McDonnell Ann Intern Med 2008
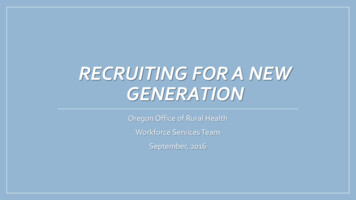
OHSUReproduced with permission from: McDonnell WM, Guenther E. Narrative Review: Do State Laws Make It Easier to Say “I’mSorry?” Ann Intern Med. 2008;149:811-815.
ORS 677.082¹Expression of regret or apologyOHSUFor the purposes of any civil action against a person licensed by theOregon Medical Board or a health care institution, health care facility orother entity that employs the person or grants the person privileges, anyexpression of regret or apology made by or on behalf of the person,the institution, the facility or other entity, including an expression ofregret or apology that is made in writing, orally or by conduct, doesnot constitute an admission of liability.(2)A person who is licensed by the Oregon Medical Board, or any otherperson who makes an expression of regret or apology on behalf of aperson who is licensed by the Oregon Medical Board, may not beexamined by deposition or otherwise in any civil or administrativeproceeding, including any arbitration or mediation proceeding, withrespect to an expression of regret or apology made by or on behalf ofthe person, including expressions of regret or apology that are made inwriting, orally or by conduct. [2003 c.384 §1; 2011 c.30 §5]
Oregon Patient SafetyCommission 2013OHSULaw designed to improve mediation andencourage transparencyA clinician or patient can file with OPSC to bringthe parties together, help them find a mediator,and help resolve the claim so it doesn't have toturn into a lawsuitSettlements reached through this process arenot reported to the NPDBBerthold Internal Med 2014
Closing the Gap: LegalConcernsOHSUIt seems that if disclosure of medical erroris made with compassion, in a timelymanner, and with good communicationskills both during and after the disclosureprocess, patients and their families are atleast no more likely to seek legal actionand some lawsuits may actually beavoided.Straumanis Pediatr Crit Care Med 2007
Closing the Gap: DevelopingSkillsOHSUFew feel prepared for theseconversations Only 9% of physicians report having hadtraining 87% indicated a desire for such trainingGallagher et al. Arch Intern Med 2006
OHSU
Closing the Gap: DevelopingSkillsOHSUResearch suggests training helpsTargeted-skills training can producesustained changes in physicians’communication behaviorsAn education program for disclosingmedical errors was helpful in improvingconfidence in medical error disclosureKim BMJ 2017Gardner J Grad Med Ed 2018Levinson Patient Ed and Counseling 2013Fallowfield Lancet 2002
The link between disclosure andpatient safetyOHSUReducingerrorsDisclosurePatient safety“Open disclosure is the most effective way to reduce errors because it begins theprocess of learning” -- Nikki Centomani, R.N., Director, Department of Safety andRisk Management at the University of Illinois Medical Center
Closing the Gap: Patient SafetyOHSU Talking about mistakes has a stronglearning effect"There is much to learn from the ability ofthe system to detect and recover fromfailures and close calls."Vincent et al. Implementation Science 2017
Closing the Gap: Patient SafetyOHSU An organizational culture of safetyBlame-free environment withpunishment-free reporting Expectation of collaboration acrossranks to seek solutions Willingness to direct resources toaddress safety concernsBoysen Ochsner J 2013
The Process of DisclosureOHSUA continuum of encounters between thepatient, the patient’s family and membersof the health care institution at which theincident occurredThe first priority must be the patient andthe family of the patientAll communications must be culturally andlinguistically appropriate.
The Disclosure ProcessOHSUProcess, not an event Initial Conversation Root Cause Analysis Follow-up Conversation Plan for on-going conversations withthe family over what occurred ifdesired
Disclosure 101OHSUPatients need Truthful, accurate information Emotional support, including apology Follow-up, potentially compensationHealthcare workers need Disclosure coaching Emotional support
Disclosure 101OHSUCertain principles are essential toeffective disclosure conversationsBut content is not enough – genuineempathy, caring, and concern areessential and patients can tell if you’re faking it!
PreparationOHSUStay attentive to the medical needs of thepatientInitial discussion within a few hours of theeventWho will be in the room? Clinicians with prior relationship Make sure everyone is emotionally capable Careful planning around rolesAttending physician usually leads theconversation
What should be told?OHSUFacts should always be disclosed, andgenerally the sooner the better BUTThe first story is usually incomplete andsometimes totally wrongAvoid natural desire to “put it alltogether” by connecting a few dots tomake a whole picture
Possible “agenda” forconversationOHSUReview of the facts (no speculation!)Clear, honest communication of regretSteps to care for the patientSteps to investigate event, prevent recurrenceWho will speak to the family next, and whenOffer of support services to patient / familyClose with sincere expressions of support,sympathy, concernAmerican Society for Healthcare Risk Management
“I’m sorry” “Apology”OHSU“I’m sorry for what has happened to you”is always appropriateBe careful of apologies that include “buts” “I’m sorry but if the nurse had only calledme ”Do not blame “the system” or colleagues. “The lab always does this ”
Additional “tips”OHSUBe yourself – it is possible to be “too careful” in choosingyour wordsFamilies need to hear a story that “makes sense” and is“plausible,” even when the facts are incompleteAnticipate potential reactions: quiet or loud anger,sarcasmBe prepared not to be “forgiven”Anticipate possible questions: “I want a different doctor / nurse” “Who’s going to pay for this additional treatment?”
Financial CompensationOHSU
Process After the InitialDisclosureOHSURoot cause analysisFollow-up meeting Begin by stating there has been an error; Describe the course of events State the nature of the mistake, consequences, andcorrective action Express personal regret and apologize Elicit questions or concerns and address them Plan the next step and next contact with the patientBerthold Internal Med 2014
Reflection After DisclosureOHSUHas there been appropriatecommunication and disclosure to thepatient and family, most often by a team?Has the organization made a statement ofempathy and issued an apology in caseswhere there is fault?Is the organization positioned to never losesight of the patient and family?
Assessment of the ProcessOHSUElicit feedback from the patients,families, and health care providers onthe disclosure processReview the lessons learned and makeappropriate systems changesProvide on-going support services toaffected health care personnel
SummaryOHSUThere is good information regarding the artand the science of disclosureThere remains much to be learnedOne thing we do know is that the art ofmessage delivery is as important as thecontent“I've learned that people will forget what you said, people will forget what youdid, but people will never forget how you made them feel.” --Maya Angelou
ResourcesOHSU AHRQ Toolkit 2016: provides a structuredprocess for ongoing communication with andcare for the affected patient and family, supportfor healthcare providers involved in the event,and a focus on system-based learning to preventrecurrence Oregon Patient Safety p/PSRP 2019 Annual Report.pdf
AcknowledgementsOHSUMy MomDr. Thomas GallagherDr. Edward Clark
To Err Is Human: Building a Safer Health System Institute of Medicine 2000. OHSU. Background Preventable medical errors in the US 250,000 to 440,000 deaths a year 3rd leading cause of death after heart disease and cancer Estimated 17 billion in direct medical