Transcription
Mini ReviewModifying an Implant: A Mini-reviewof Dental Implant BiomaterialsOliver K. Semisch-Dieter1, Andy H. Choi1 and Martin P. Stewart1,*1SchoolAbstractDental implants have been used as far back as 2000BC, and since then have developed into highly sophisticated solutions for tooth replacement. It is becoming increasingly important for the materials used in dentalimplants to exhibit and maintain favorable long-term mechanical, biological and more recently, aestheticproperties. This review aims to assess the biomaterials used in modern dental implants, introducing theirproperties, and concentrating on modifications to improve these biomaterials. Focus is drawn to the prominent biomaterials, titanium (Ti) and zirconia due to their prevalence in implant dentistry. Additionally, novelcoatings and materials with potential use as viable improvements or alternatives are reviewed. An effectivedental biomaterial should osseointegrate, maintain structural integrity, resist corrosion and infection, and notcause systemic toxicity or cytotoxicity. Current materials such as bioactive glass offer protection against biofilm formation, and when combined with a titanium–zirconium (TiZr) alloy, provide a reliable combinationof properties to represent a competitive alternative. Further long-term clinical studies are needed to informthe development of next-generation materials.KeywordsBiocompatibility, biomaterials, dental implant, titanium, zirconia.Significance StatementBiomaterials have become essential for modern implants. A suitable implant biomaterial integrates into thebody to perform a key function, whilst minimizing negative immune response. Focusing on dentistry, the useof dental implants for tooth replacement requires a balance between bodily response, mechanical structureand performance, and aesthetics. This mini-review addresses the use of biomaterials in dental implants withsignificant comparisons drawn between Ti and zirconia. Attention is drawn to optimizing surface modification processes and the additional use of coatings. Alternatives and novel developments are addressed, providing potential implications of combining biomaterials to form novel composites that combine andsynergize the benefits of each material.IntroductionBiomaterials are crucial for modern medical applications, and in the last severaldecades, these materials have been refinedand improved for applications seen indentistry, orthopedics, drug delivery, andcardiology. Candidate materials includepolymers, metals (and their alloys), ceramics, composites (e.g. carbon fiber), andglass. For clinical use, the material mustnot cause any adverse or damaging effectsto the patient [1]. This concept is knownas biocompatibility and was described byWilliams as, “the ability of a biomaterialto perform its desired function with respectto a medical therapy, without eliciting anyundesirable local or systemic effects in therecipient or beneficiary of that therapy, butgenerating the most appropriate beneficialcellular or tissue response to that specific12 of Life Sciences,Faculty of Science, Universityof Technology Sydney, Ultimo,NSW, Australia*Correspondence to:Martin P. StewartE-mail: martin.stewart@uts.edu.auReceived: September 7 2020Revised: December 7 2020Accepted: January 4 2021Published Online: March 192021Available at:https://bio-integration.org/situation, and optimizing the clinically relevant performance of that therapy” [2].The application of biomaterials as adental implant is shown in Figure 1A; anendosseous fixture is used to replace theroot and support a dental prosthesis. Dentalimplants have become an evidence-basedtreatment for the replacement of missingteeth. Selecting a biomaterial for a dental implant requires additional considerations for biological, mechanical, and aesthetic properties. Modern dental implantsneed to feature effective osseointegrationand maintain long-term stability of theirfavorable properties to maintain both theimplant’s structure and the integrity of surrounding hard and soft tissue [3, 4].This review aims to assess the currentstate of biomaterials (Ti, zirconia, andnovel materials) used in dental implants.Materials are assessed on their attributes,BIOI 2021, Vol 2, No. 1, 12–21https://bio-integration.org doi: 10.15212/bioi-2020-0034 2021 The Authors. Creative Commons Attribution 4.0 International License
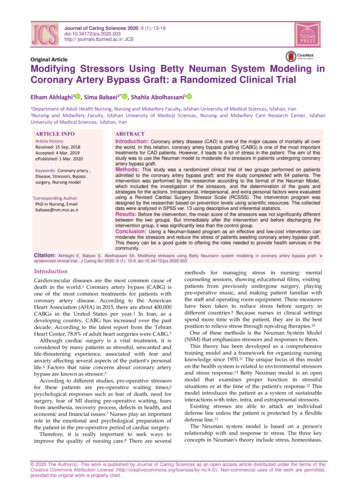
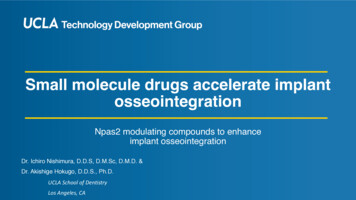
Mini ReviewBIOI 2021ABFigure 1 (A) Illustrates a cross-sectional view of a dental implant and the surrounding oral tissue. (B) Selecting the appropriate material touse for the implant requires considerations of implant durability, cell adhesion, and physiological implications for implant biocompatibility, andaesthetic concerns for patient satisfaction.characteristics, comparison of strengths and weaknesses,biocompatibility, and new advancements in addressing anyissues or concerns.deterring biofilm formation. Current surface topographiesinclude anodization, sandblasting, and polishing, however,conclusive evidence on which specific surface topographiesare optimal and why remains undetermined [9].TitaniumAlternative alloysTi is widely used for medical applications and is currentlythe most commonly used material for dental implants. Thepopularity is in part due to the combination of its tensilestrength, biocompatibility, ability to osseointegrate, density,corrosion resistance, and inert properties. Pure Ti, whilebeing safe for most clinical use, has been observed to forman accumulation of Ti ions around the implant site. Whileno material is entirely bioinert, such ions released from animplant that fails to osseointegrate may induce proinflammatory responses from sensitization. Such failure occurswhen there is a lack of biomechanical stability due to inadequate osseointegration. Stability can be promoted by modifying the implant’s physiochemical properties and surfacetopography. Observations from failed Ti implants show anincreased lymph node Ti ion concentration by 7.4–9 timesand lung Ti ion concentration by 2.2–3.8 times when compared to a successfully integrated implant [5, 6] (Table 1).Ti dental implants have been occasionally observed to resultin an allergic reaction. However, the exact mechanism for Tiion release and systemic effects remains unclear [7].Surface modifications of Ti implants are performed toimprove osseointegration and modulate cell adhesion. Thelargest post-operative issue with such implants is biofilm-induced mucositis, inflammation of mucous membranes,which can further develop into peri-implantitis, the inflammation of the gum and the surrounding bone structure. Thefirst generation of surface modification was developed inthe 1960s, where machined Ti (smooth surface) was usedto promote osseointegration by leaving a small degree ofroughness. Second generation surface modifications havebeen widely available since the 1990s and improve on thefirst generation by creating a microscopically rough surfacetopography. Finally, the current third generation (also knownas bioactive surfaces) maintains similar roughness to the second generation and are modified chemically or topographically to promote osseointegration [8]. Most surface topographies minimize vertical deviation to 1 μm or less, effectivelyIt is known that Ti can form alloys to solve reactivity concerns[1]. Vanadium (V) and aluminum (Al) are common alloyingelements for Ti (seen in Ti6Al4V alloy). Individually eachelement has shown potential adverse effects in high concentrations, causing carcinogenicity and neurotoxicity [10–12].However, reports on V also demonstrate antidiabetic effectsand resulted in reduced weight gain and gastrointestinal discomfort [1, 13]. Attempts are being made to replace thesealloying elements with less toxic elements such as niobium(Nb), tantalum (Ta), and palladium (Pd), to improve biocompatibility; however, Ti6Al4V remains a common choice [14].When comparing a Ti alloy to surgical stainless steel andcobalt alloys, the superior quality of Ti is its corrosion resistance. The ability for Ti alloys to withstand corrosive environments and develop an oxide layer with a shorter repassivation time compared to other metal alloys, aids in preventinga release of ions which can potentially be toxic (cobalt) orcause allergic reactions (nickel, found in stainless steel) [15].A unique alloy, TiZr has shown clinical success in the pastdecade. Under the trade name Roxolid, Institut StraumannAG, Basel, Switzerland (a 15% Zr, 85% Ti composition), theTiZr alloy was designed for dental implants, becoming a viable alternative to zirconia and other Ti-based implants [16].TiZr offers enhanced osseointegration compared to Ti6Al4Vand pure Ti and avoids the use of toxic alloying elements.Additionally, corrosion resistance can potentially reduceproblems associated with peripheral Ti ion concentrations[17–19]. A recent study observed that TiZr retains the abilityfor surface enhancement without compromising the mechanical strength of the implant [20]. While TiZr dental implantsdo not offer the aesthetic qualities of zirconia, they demon strate highly preferable qualities among clinically availableTi alloy options.TiNb is another alloy with favorable properties andprovides a low elastic modulus similar to human corticalbone. It is clinically significant as it reduces the issue ofstress concentration between the implant and bone, thusOliver K. Semisch-Dieter et al.: Modifying an Implant in Dental Implant Biomaterials 13
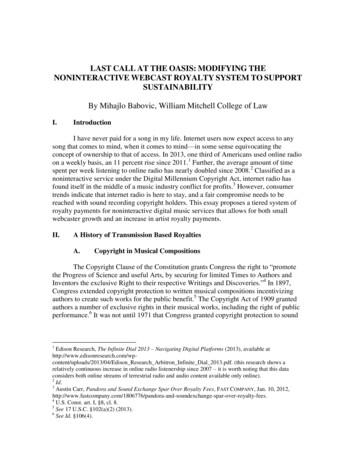
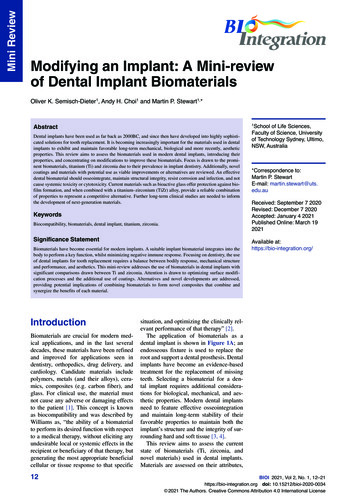
14 In vivoIn vivoIn vivo: pigmodelZeller et al. (2020)[80]Herrmann et al.(2020) [81]Kubasiewicz-Rosset al. (2018) [82]Studying the osseointegration of commercially availableTi and zirconia implantsExamining early and mature biofilms on Ti and zirconiaimplants at different roughness.Investigation of biofilm formation on gold and silver metalalloys, PEEK, zirconia, and TiZr alloy implants.Investigating the blood interaction, and resultingosseointegration, at the bone-implant interface ofmicrostructure Ti and zirconia implants.In vitroIn vitroIn vitroAssessing the effect of Ti and zirconia particles onosteoblast and fibroblast activity, and cytokine expressionAssessing biofilm formation on hydroxyapatite, Ti andzirconia implant surfacesInvestigating fracture resistance and implant failureIn vitroSchwarz et al.(2019) [58]Sánchez et al.(2014) [77]Rosentritt et al.(2014) [78]Rottmar et al.(2019) [79]Comparing the osseointegration of modified Ti andzirconia implant surfacesIn vivo: sheepmodelAssessing the effect of bacterial and mechanical fatigueon zirconia implantsIn vitroLanghoff et al.(2008) [47]Evaluating in vitro and in vivo performance of functionallygraded (FG) biomaterials of calcium phosphate/Ti alloysComparing biofilm formation on zirconia and Ti implantsIn vitro and invivoIn vitroEl-Hadad et al.(2018) [24]Roehling et al.(2017) [45]Siddiqui et al.(2019) [46]DescriptionInvestigating macrophage and fibroblasts behavior at thebone–implant interface of commercial implantsStudy typeIn vitroConclusionSurface composition (Ti vs ZLA vs Ti-Zi) had little effect on macrophage orfibroblast behavior, while hydrophilicity promoted lower inflammation andbetter soft tissue integrationFG Ti implants (Ti6Al4V) demonstrated the best in vitro cytocompatibility andin vivo systemic toxicity and osseointegration resultsZirconia presented a significant reduction in biofilm and plaque formationcompared to Ti implant surfacesMechanical loading and colonizing bacteria did not induce significantdegradation or damage. The authors consider zirconia a suitable alternativeto Ti implantsAll implants achieved successful osseointegration, with zirconia reachingslightly higher initial bone-implant contact (BIC). Overall, there were nosignificant differences in BICBoth Ti and zirconia particles reduced osteoblast and fibroblast cell viability,with no proinflammatory effect. The findings do require in vivo validationBiofilm formed irrespective of implant material, while only the morphologyand structure of the biofilms were differentBonded/screwed zirconia implants displayed lower fracture resistancecompared to two-piece Ti and one-piece zirconia implantsThrombogenicity was the highest on zirconia surfaces compared to Ti. Itwas suggested that a higher thrombogenicity promotes osseointegration,however, similarly micro-structured Ti maintained good osseointegrationpotentialPEEK, Zirconia and TiZr materials demonstrated similar biofilm formationon commercially available implants. Only gold and silver-based materialsshowed reduced biofilm growthZirconia showed significantly higher total bacterial cell counts, but could bedue to surface roughness. Biofilm formation and total bacterial cell countscould be assumed to be caused by surface roughnessOverall zirconia displayed similar levels of osseointegration, measuredthrough BIC. Differences between implant material yielded no statisticallyimportant differencesSummary of in vivo and in vitro studies assessing clinically relevant factors of Ti and zirconia dental implantsAuthorsWang et al. (2019)[5]Table 1Mini ReviewBIOI 2021Oliver K. Semisch-Dieter et al.: Modifying an Implant in Dental Implant Biomaterials
promoting osseointegration. This alloy improves on otherfunctional aspects compared to pure Ti, possessing highertoughness, hardness, and corrosion resistance. TiNb hasbeen proposed as a suitable alternative for replacing failedhard tissue [21, 22].Recent trendsRecent trends in the field point toward the utility of novelideas such as: (1) the development of implant coatings, and(2) the incorporation of alternative elements (e.g. iodine (I)and strontium (Sr)) to support Ti implants. The next generation of therapeutic implants may incorporate nano-engineered surface topographies. The use of anodized titania(titanium dioxide, TiO2) nanotubes (TNT) on the surfaceof Ti implants shows promising results. These NTs offeradvantages in topography, mechano-transduction, drugrelease, and mediating toxicity. The TNTs mimic the topographical scale of surrounding native tissues to significantlyupregulate protein absorption. The bone remodeling causedby mechanical strain stimulates cells at the bone–implantinterface to promote initial attachment and continued adhesion. TNTs that are capable of local drug release potentiallyallow for direct targeting of the implant site and a reductionin toxicity compared to systemic administration. Togetherthese factors contribute to influence cellular functions andimmunomodulatory responses towards dental implants [23,24]. Compared to conventional Ti implants, TNTs have beenobserved to orchestrate osteogenesis [25].A recent development in surface modifications is plasmaimmersion ion implantation which provides a uniform application over complex surface geometries, while reducingoverall cost and processing time. The in vitro testing of anoxygen plasma immersion ion implantation (OPIII) to a Tiimplant identified improvements in protein expression andcorrosion resistance [26]. The use of OPIII is capable ofproducing a bioactive oxide film which was determined toimprove in vitro cell differentiation and in vivo osseointegration. It is undetermined to what degree the process optimizesthe implant’s surface properties (topography, wettability, androughness), however, the most current research has observedno significant alteration [27]. In its current state, OPIII hasa good potential to become a viable surface modificationthrough further research.Additionally, an in vivo study demonstrated the ability touse macrophage polarization via NTs to augment osseointegration [28]. The property of local drug release is anothersignificant advantage of this technology. While someattempts have been made to incorporate antibiotics into NTs,these traditional or organic antibiotics pose the risk of resistance and are limited by selective toxicity. This has resultedin attention towards inorganic antibacterial agents, such assilver. Using silver as a coating has shown strong antimicrobial effects, however, it poses biocompatibility issues.Studies are testing the effect of loading silver nanoparticlesonto TNTs. These TNTs use a reducing agent to disperse silver nanoparticles from the coating and can aid in patient careduring the initial postoperative risk of infection. Clinicalsafety and molecular mechanism still require further studies[29]. Long-term studies are required to translate this technology for clinical application, and cost will also need to beconsidered for commercial implementation.Continued research in coatings has led to novel improvements on hydroxyapatite (HAp) for Ti6Al4V implants. Insitu synthesis of HAp-based nanocomposites including chitosan and polycaprolactone/fluoride (PCL/F) substitutionaim to utilize the advantages of HAp with promoting theformation of bone-like apatite at the bone–implant interface,while minimizing the brittleness of HAp. A sol–gel methodand alkali-treated Ti is used to provide a homogenous, crackfree coating that does not suffer from any delamination. Bothnanocomposites required a minimum 10 wt.% of HAp toprovide the desired results with the respective composite [30,31]. Research for chitosan/HAp identified improved cellularresponse at lower HAp content (10 wt.%), with higher content (50 and 60 wt.%) providing improved surface adhesionstrength, roughness, and hydrophilicity [30]. It was notedwith PCL/F that HAp content up to 30 wt.% improved similar surface properties, and higher corrosion resistance [31].Both coatings meet the required performance of bioactivecoatings and show potential for future clinical application.An alternative material to Ti is Ta. Ta is a useful biomaterial due to being highly bioactive and holds similarproperties to Ti regarding corrosion resistance and biocompatibility. The improvement over Ti is the optimization ofthe osseointegration process. However, it is a high-densitymaterial which is expensive to manufacture. Therefore, combining the properties of Ti and Ta, research has focused ondeveloping Ta oxide films. Preliminary research observedpromising results, improving wear resistance to microbialand chemical degradation. Improved osseointegration wasalso observed with increased osteoblastic activity and morphology. Finally, the study did not indicate any increasedbacterial cell adhesion when compared to conventional Tiimplants [32].Adding alternative elements is not a new concept, andcontinuing with the idea of surface treatment, the additionof Sr is a possibility. Historically Sr is biologically knownfor promoting osteoblast activity and inhibiting osteoclast activity. Oral administration of Sr may cause adverseeffects; therefore, surface incorporation (on Ti implants) hasbeen preliminarily observed to increase early bone osseointegration [33]. Another potential element is I, an essentialelement with antiseptic properties and may be a useful biomaterial for dental implants. A previous study indicated thatI-supported Ti implants in orthopedic applications substantially reduced the incidence of inflammation. The enhancedimplants exhibited cytocompatibility and increased antimicrobial activity [34].Another approach to modification is altering the implantdesign; the use of porous Ti has been researched to improveintegration into hard tissue. The sponge-like framework alsoallows for antibacterial agents to be directly incorporatedinto the implant surface or via degradable drug carriers [35].Currently challenges around optimization of the structureand high manufacturing cost are a barrier to implementationof this technology in the clinic [36].A recent study has improved on the capability of porousTi through using micropore channels in Ti implants toOliver K. Semisch-Dieter et al.: Modifying an Implant in Dental Implant Biomaterials 15Mini ReviewBIOI 2021
Mini ReviewBIOI 2021preserve alveolar height without additional growth factors.The canine in vivo model provides evidence in minimizingalveolar bone loss, while promoting cell viability, proliferation,
of dental implants for tooth replacement requires a balance between bodily response, mechanical structure and performance, and aesthetics. This mini-review addresses the use of biomaterials in dental implants with . AB Figure 1 (A) Illustrates a cross-sectional view of a dental implant and the surrounding oral tissue. (B) Selecting the .