Transcription
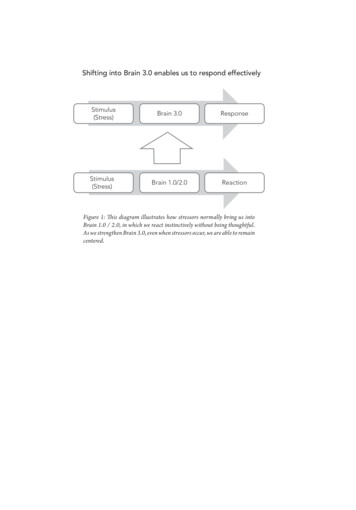
Brain Stimulation as a Viable Treatment for Antisocial Spectrum DisordersStevie Kloepfer 1*B.A. Candidate, Department of Psychology, California State University Stanislaus, 1 University Circle, Turlock, CA 95382Received 9 May, 2020; accepted 15 May, 2020AbstractIndividuals with Antisocial Personality Disorder (ASPD) and psychopathy are characterized by a failure to conform tosocial norms, reckless disregard for their own safety and that of others and a lack of empathy and remorse. In interpersonalrelationships, the defining features of these disorders include deceitfulness, consistent irresponsibility, impulsivity, irritability andaggressiveness. Although symptoms manifest behaviorally, the source of the disordered behavior may be organic, as brain regionssuch as the ventromedial prefrontal cortex, the anterior cingulate cortex, and the amygdala, are thought to contribute to the severityof the disorders. Despite this knowledge, viable treatment options for ASPD and psychopathy have not been established due to thecomplexity and range of traits exhibited. ASPD and Psychopathy, although distinct, are similar in that they typically negativelyimpact society both through acts of manipulation and acts of crime. Because standard psychiatric treatments such as talk therapy,medication, and electroconvulsive therapy (ECT) have been ineffective, I explored the potential viability of the experimentalneuromodulatory procedures of Deep Brain Stimulation and Transcranial Magnetic Stimulation in the reduction of maladaptivetraits exhibited by individuals with ASPD and Psychopathy. If these procedures demonstrate potential, they should be implementedinto medical practice as viable treatment options.Keywords: Neuromodulation, Deep Brain Stimulation, Transcranial Magnetic StimulationIntroductionThe etymology of the terms “antisocial” and“psychopath” can hold many negative connotations andare therefore commonly misused. The Diagnostic andStatistical Manual of Mental Disorders (DSM5)recognizes Antisocial Personality Disorder (ASPD) andpsychopathy as a singular disorder. However,psychopaths are thought to have been born with thegenetic predisposition for disordered behavior whereasindividuals with ASPD are thought to have been madeby being exposed to a damaging environment (Koenigs,2012). Despite this difference in how the disorders arethought to have originated, they often share strikinglysimilar characteristics. ASPD and psychopathy aredisorders characterized by behavior such as a failure toconform to social norms, reckless disregard for theirown safety and that of others, and a lack of empathy andremorse. These characteristics can be exhibited in avariety of ways, but the most common outwardexpressions of these traits are observable in the form ofdeceitfulness, consistent irresponsibility, impulsivity,irritability and aggressiveness (American PsychiatricAssociation, 2013). Because of the dysfunctional natureof the attributes exhibited by individuals with ASPDand psychopathy, they often clash with the normsimposed upon them by society which can result introuble ininterpersonal relationships, workenvironments, and with the law.1*Corresponding author. Email: skloepfer@csustan.eduA subset of individuals with ASPD andpsychopathy negatively impact society throughpersistent and violent criminal actions. An estimated 1%of males meet the criteria for psychopathy, whichroughly equals 1,150,000 adult psychopathic males inthe United States. A vast majority of this population,almost 93%, are in prison, jail or on probation. Thisleaves 7% of the psychopathic population that haven’tcommitted crimes or haven’t yet been caught (Kiehl etal., 2012; Koenigs, 2012). Although these individualsmay not engage in violent crime, their interpersonalrelationships and mental health may suffer greatly fromtheir disorder. It is suggested that the ventromedialprefrontal cortex (processing risk, fear), the anteriorcingulate cortex (empathy, impulse control, emotion,decision-making), the amygdala (anger, fear,aggression control), and the density of grey matter(sensory perception, decision making, self-control,emotion regulation) in the brain are involved in theseverity of the disorders (Figure 1) (Koenigs, 2012). Itis also important to note that even though the brain isaffected, it does not mean individuals with ASPD andpsychopathy are destined to be criminals as they arefully capable of making their own decisions. Unlikeother disorders, such as bipolar disorder and obsessivecompulsive disorder, ASPD and psychopathy cannotcurrently be treated with medication due to how little is
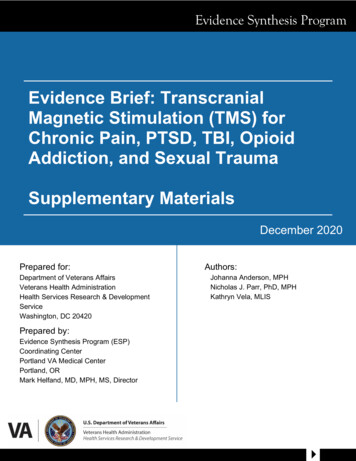
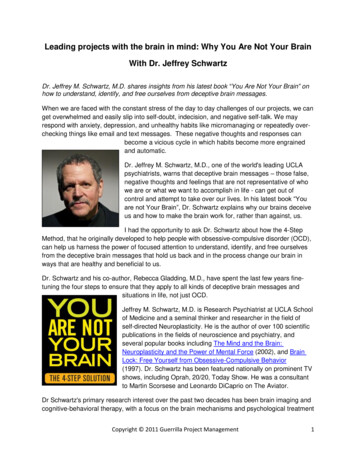
known about the disorders’ underlying mechanisms(Koenigs, 2012). However, a lack of viable treatmentoptions is not indicative of a failure to search for one. Inthe past, treatments used with the intent to curepsychopaths of their disorder were psychoanalysis,group-therapy, client-centered therapy, psychosurgery,and electroshock and drug therapies. Regardless of pastefforts, therapies proved to be ineffective and those whounderwent treatment were often more aggressive andshowed higher rates of recidivism following theirincarceration (Hare, 1970). This exemplifies the needfor continued research, and I believe that localizing theneural areas that contribute to ASPD and psychopathycould potentially lead to an effective treatment withinDeep Brain Stimulation (DBS) and TranscranialMagnetic Stimulation (TMS) procedures.Figure 1:Pet Scan of a Normal BrainPet Scan of a Psychopathic Brainstimulation is a procedure facilitated by a system withfour different components: the DBS electrode(s), theextension wire, the implantable pulse generator (IPG),and the external programming device. In contrast to theelectrode with a single contact at the tip that waspreviously used for DBS before technologicaladvancements were made, the most current systemconfiguration is the “quadripolar DBS electrode”. Thequadripolar DBS electrode is flexible and equipped withfour separate contacts constructed of a platinum-iridiumalloy and located near the tip of the rod. This allows forspecificity in adjustments to the electric field andprovides more accurate therapeutic results. Lastly, theIPG is composed of a titanium frame and lithiumbatteries. ICP devices range from constant-voltagecontrolled, to constant-current controlled, and ss (Vitek, p. 10-14).Figure -brain-stimulation/Note: CT image of Deep Brain -psychopath-brain-looks-like-2015-7Credit: James FallonNote: The top pet scan is characteristic of a normal male brain,whereas the bottom scan is characteristic of a psychopath’s brain. Thephotos above show a heat map of human brain function, warmercolors more activity, cool colors less activity. Note that the in theACC, vPC, and Amygdala show much less activity in the bottom photo.DBS is a neurosurgical procedure currentlyused to treat disorders such as epilepsy, Parkinson’sDisease, and dystonia by altering the neural activitywith electricity (Vitek, 2014) One of the mostcompelling aspects of DBS is that the procedure iscompletely reversible and poses a minimal risk ofimplantation complications due to infection. Deep brainSimilarly, Transcranial Magnetic Stimulation(TMS) is a procedure commonly used as a treatmentmethod for refractory disorders, and most notably,depression (Bermudes, 2018). In contrast to DBS, TMSuses magnetism and electricity to create a movingelectrical current using the brain as a conductor, byrapidly alternating the flow of electricity. All TMSmachines are comprised of the same components: acapacitor which is used to contain the electricity, thecoils used to induce an electrical field, and a thyristorswitch which controls how quickly the electricity flows.In the past, one small circular coil was used but thatmethod soon became outdated due to the limited rangecreated by the coil. Today, the most common TMSmethod requires two round “butterfly”, or “figure-eight”coils which allows for a more a more focused electricalfield. The strength of the magnetic field created isdependent on the distance the focal area is from themagnet, as a greater distance from the desired regionresults in a weaker magnetic field (Bermudes, 2018, p.24).
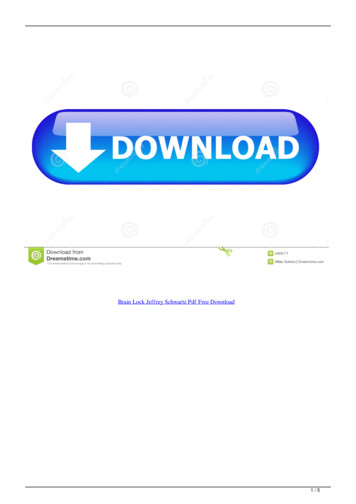
Figure 3.Organizing Results: I organized my results into the formof a table in order to consolidate the data in a way thatis visually org/wiki/Transcranial magnetic stimulationNote: TMS Schematic DiagramMethodsSources: I used primary sources where original researchwas conducted, and secondary sources that pertain todisorders that have been evidenced to benefit from brainstimulation. This includes, but is not limited to:Obsessive-Compulsive Disorder, Parkinson’s Disease,epilepsy, and the act of self-injurious behavior. Inaddition to this, I conducted structured interviews asprimary sources with experts in Antisocial PersonalityDisorder, Deep Brain Stimulation, and TranscranialMagnetic Stimulation.Procedures: I examined research articles where DBSwas an effective treatment, and how the affected neuralareas correspond to those which are believed toinfluence ASPD and psychopathy. Before conductingthe interview, I first obtained IRB Approval. I acquiredinformed consent by emailing the consent form to eachparticipant once they agreed to participate in theinterview process. By consenting, the interviewee gaveme permission to record our conversation, and to sharetheir name, profession, responses, and opinions in myfinal project. Each interview took place via telephonecall.Measures: The questions asked pertained to theinterviewee’s profession, the duration of interest in thesubject, and their expertise regarding whether brainstimulation could be used as a treatment forpsychopathy and antisocial spectrum disorders.Data Analysis: I examined the qualitative data obtainedfrom these studies and I found a correlation betweenbrain stimulation procedures and the alteration ofactivity in the prefrontal cortex, the anterior cingulatecortex, the subthalamic nucleus and the amygdala.DBS is a procedure that has been evidenced toprovide relief for movement disorders (Parkinson’sDisease (PD), epilepsy) and neurological disorders(OCD). However, the impact the procedure has on themood, impulsivity, and emotion of the patients treated,raises the question of whether DBS could be used toalter the functioning of dysfunctional regions in thehuman brain. There is an increased effort to understandhow the subthalamic nucleus (STN), a neural structurecommonly associated with movement, can affectemotional responses. This can be exemplified by a studyof seven DBS patients with PD who underwentsubthalamic nucleus DBS while watching 1.6-4.7minute emotion evoking and neutral video clips. (Bick,et. al., 2017) Four negative valance and four positivevalance emotional video clips were chosen from adatabase specifically for their emotion inductionproperties and were shown at random intervals. Duringthe emotional induction task, infrared spectroscopy wasused to monitor oxyhemoglobin concentration duringthe emotional video clips. This measures the levels ofoxygen in the prefrontal cortex and is associated withpleasure. The researchers found that STN DBS altersprefrontal activity during emotion induction byaffecting momentary action selection and long-term finetuning of behavioral repertoire. (Bick, 2017)(Table 1)This study shows that DBS of the STN changed howparticipants perceived the emotion-invoking videos, andthat in turn, their impulsivity and behavior changed as aresult, which could be helpful for people with ASPD.Additionally, twelve anterior thalamic nucleus(ANT) and Anterior Cingulate Cortex (ACC) DBSpatients with treatment refractory epilepsy were askedto complete a computer task that tested executivereaction time to go/no-go prompts with added stressorsand emotional distractor (Hartikainen et. al., 2014). Thetest was administered on a computer program thatintroduced the visual stimuli and subsequently collectedthe data while each patient was connected to anelectroencephalograph (EEG monitor). The testrequired that the patients discriminate from trianglespointing up or down while a symbol resembling a trafficlight signaled for the patient to respond or withhold theirresponse. The distractors included a line drawing of aspider, and a line drawing of a flower that appeared inthe center of the go/no-go symbol. The patients were torespond as quickly as possible while following thedirections from the symbol. The test was performed insixteen blocks, with six-to-eight minutes of bipolar DBSstimulation and a consecutive six-to-eight minutes
without stimulation with an alternation of status at eachblock. Researchers found that ANT and ACCstimulation increased attention-allocation to threat,compromised response inhibition, and impairedcognitive control (Hartikainen, 2014). (Table 1) Thisstudy shows that ANT and ACC DBS resulted in anincrease of attention placed on threatening stimuli,which is a behavior that most people with ASPD andPsychopathy lack. Additionally, this study showed thatstimulation of this region increased the impulsivity ofparticipants, which would be detrimental to someonewho already has a decreased sense of self-control.However, this raises the question about whether thestimulation parameters could be adjusted to achieve theopposite result.Another study that emphasizes how DBS canalter brain functioning was basolateral amygdala DBS,performed on a fourteen-year-old boy diagnosed withsevere Kanner’s autism, mental retardation, andcerebral palsy, in an attempt to decrease the severity ofthe child’s aggressive behavior (Sturm, et. al., 2012).The patient’s disorders were marked by an inability tocommunicate verbally, frequent anxiety attacks,tantrums, impaired self-regulatory processes inresponse to auditory and visual stimuli, impaired affectmodulation, emotional disturbances, and lifethreatening self-injurious behavior (SIB) that requiredconstant restraint. When the patient reached the age often he was treated for self-injurious behavior with adaily dosage of 2mg of Risperidone. This resulted in adrastic decrease of SIB until the patient entered pubertyand SIB started up again with increased frequency andaggression. The patient was subsequently treated withvarious other mood stabilizing medications, all of whichfailed to improve his symptoms. The patient’s legalguardians provided consent for the patient to be treatedwith the DBS of the amygdaloid complex and the supraamygdaloid projection system which controls fear,anxiety, and emotion. Two quadripolar DBS electrodeswere implanted through burr holes in the patient’s skull,and stimulation was activated several days after theinitial surgery. Twenty-six months after the DBStreatment was implemented, the patient’s SIB andaggression steadily improved, and the positive resultsshowed significant signs of continued improvement(Sturm, 2012). (Table 1) This study emphasized theefficacy of DBS in treating aggressive behavior,impairments in self-regulation, and decreased activity inthe amygdala, all of which are the prominent features ofASPD and psychopathy.Table 1. Table of Neural Areas Affected by DBS and SubsequentResults*1*2*3Note: location abbreviations; Subthalamic Nucleus (SubTNu),Anterior Thalamic Nucleus (ATN), Anterior Cingulate Cortex (ACC),Amygdaloid Complex (Amy Co).A similar study that examined how stimulationcan decrease aggression, was the examination of directtranscranial magnetic stimulation of the dorsolateralprefrontal cortex (dPFC). This study included thirtynine participants in the TMS group and forty-twoparticipants in the sham group (Choy, et. al., 2018).During stimulation, all participants performed aPsychomotor Vigilance Task, and the Iowa Gamblingtask which are two experimental procedures known tostimulate the Dorsolateral Prefrontal Cortex.Participants then assessed two hypothetical vignettesused to gauge perceptions of moral wrongness whichdepicted two scenarios; physical and sexual assault.Participants were then asked to gauge the likeliness theywould participate in those aggressive acts from 0 (not atall likely) to 10 (extremely likely). Participants werealso assessed in aggressiveness by interacting with asimulated voodoo doll on a computer screen. Users weretold that the voodoo doll represented someone close tothem, and were subsequently allowed to insert as manypins into the doll as they desired. The more pins thatwere used indicated higher aggression levels. This studyfound that the individuals who received anodalstimulation of the dPF resulted in the decreased intent tocommit aggressive acts one day after stimulation (Choy,et. al., 2018). (Table 2) This study shows the potentialof TMS to decrease aggressive and violent behavior,which is one of the defining features of antisocialbehavior.The final study that I examined, was the DirectCurrent Transcranial Magnetic Stimulation performedon the medial prefrontal cortex of a group of 40 healthy
subjects (Liao et. al., 2018). A total of twenty subjectseach, consisting of ten men and ten women wereassigned to anodal, cathodal, and placebo groups. Theparticipants were led to believe that in each trial, theywould have the option to help another subject (paintaker) that would ultimately either be electricallyshocked or spared based on the decisions they chose tomake, although no one was actually going to be harmed.In each trial, the participants were produced with a costanalysis of how much it would cost to help the paintaker and how likely it was that that they would besuccessful in helping the other person. Forty of theparticipants that were not included in the sham/placebogroup received a constant electrical current from atranscranial stimulator. The results of this studyindicated that those receiving both anodal and cathodalstimulation had an increased propensity for helpingbehavior when the probability of helping was high butdiminished when the probability of helping behaviorwas lower. The purpose of this study was to encouragethe participants to empathize with those whom theybelieved they were inflicting pain upon. This studyfound that anodal stimulation increased the propensityfor helping behavior, whereas cathodal stimulationdecreased the propensity for helping behavior (Liao,2018). (Table 2) This final study shows thatanodal/cathodal stimulation may have the potential tocause opposite effects. In addition to this, anodalstimulation was found to increase the empatheticreasoning of participants, resulting in prosocialbehavior, something most, if not all, psychopaths lack.Table 2. Table of Neural Areas Effected by TMS and subsequentresults.*4*5Note: Location abbreviations; Medial Prefrontal Cortex (mPC),Prefrontal Cortex (PC). Sample Size; In the first and second samplesonly half of the participants (matched for age/gender) receivedstimulation.Although the studies examined showedpromise, I had the pleasure of interviewing an expert togain critical insights. I spoke with Dr. Fallon, aneuroscientist with a background in psychology whostudied the brains of psychopaths for over ten years,ultimately discovering that psychopathy could bediagnosed by comparing similarities in the brainstructure of psychopaths. In an interview with Dr.Fallon, he mentioned that stimulating the inactive brainregions associated with ASPD and Psychopathy couldbe a potential treatment option for psychopaths; but thatmost areas of interest in psychiatry, not in neurology,such as dysregulated emotions and a sense of moralityare not very amenable to outside access as the center ofthose connectomes are at the base of the brain, unlessyou go in with an electrode. Dr. Fallon exemplifies thefact that although he was born with decreased neuralactivity, it does not predetermine criminality. Althoughthe studies examined have shown that maladaptive traitscould be altered and even improved by DBS or TMS, itis essential for proper studies to be executed beforeadopting either of these procedures as clinical treatmentoptions for ASPD and psychopathy. Some drawbacks tothis review were that the DBS sample sizes were highlylimited. The most critical aspect of this review toconsider, is that the studies I examined were not directlyrelated to either ASPD or psychopathy, outside of anoverlap in brain regions, so there could be a lack ofinformation regarding how affected individuals mightrespond to these treatments. This includes somepotential disadvantages to stimulation, such as thepossibility of aggravating other existing symptoms, andputting potentially unstable and socially problematicindividuals through trials. Taking into consideration thatthese studies potentially show promise, exacerbated bythe lack of treatment options makes brain stimulation anecessity in exploring future therapies.DiscussionI examined studies that involved disorderssuch as epilepsy, Parkinson’s disease, and autism. Thepurpose of this research was to examine the neuralregions receiving stimulation in neurological conditionsand how the resulting behaviors of these individualswere altered. Additionally, I included studies performedon individuals without neurological disorders as theyhighlighted the neural regions I am interested in andhelped in assessing the functionality of usingstimulation to alter the behavior of individuals who lackthe necessary qualifications for DBS. Although thestudies I examined showed promise for bothdysregulated and normal samples, the questionremaining is whether psychopaths themselves couldbenefit from treatment, and how the treatment of thoseindividuals would be initiated. Transcranial stimulation,being a non-invasive treatment might be the moredesirable treatment option. Deep brain stimulation,however, seems the most practical of the two treatmentoptions, as the implanted probes allow for deeper, morespecified access to hard-to-reach regions. However, the
invasive nature of the procedure makes the voluntarytreatment of psychopaths questionable, as psychopathsgenerally do not believe that there is anything wrongwith them. If DBS and TMS prove to be efficient inimproving maladaptive traits expressed by psychopathicand ASPD individuals, a viable step after determiningtheir efficacy may be to provide the treatment option toincarcerated individuals who are willing to receivetherapy. As of now, ASPD and psychopathy are elusive,destructive disorders that pose a substantial publicsafety risk, and the continual research of these disordersis necessary for the well-being of psychopaths, theirfamilies, and society.AcknowledgementsI thank the California State University, StanislausHonors Program for support throughout this research. Iwould like to especially thank Dr. Jamila Newton forher mentorship and continuous support.ReferencesBick, S. K, Folley, B. S., Mayer, J. S., Park, S., Charles,P. D., Camalier, C. R., Neimat, J. S. (2017).Subthalamic Nucleus Deep Brain StimulationAlters Prefrontal Correlates of EmotionInduction. Neuromodulation, u/10.1111/ner.125371*Bermudes, R., Lanocha, K., & Janicak, P.(2018). Transcranial magnetic tice (First ed.). Arlington, VA: AmericanPsychiatric Association Publishing.Choy, O., Raine, A., & Hamilton, R. (2018).Stimulation of the Prefrontal Cortex ReducesIntentions to Commit Aggression: ied,Parallel-GroupTrial. The Journal of Neuroscience : TheOfficial Journal of the Society forNeuroscience, 38(29), 6505-6512.4*Diagnostic and statistical manual of mental disorders(5th ed.). American Psychiatric Association.(2013). Washington, DC: Author.Fallon, James. Personal communication, April 15, 2020Hamani, C., Diwan, M., Macedo, C., Brandão, M.,(2010). Antidepressant-like effects of medialprefrontal cortex deep brain stimulation in rats.Biological Psychiatry, 10 (2) 15. 117-124 doi:10.1016/j.biopsych.2009.08.025Hare, Robert D. Psychopathy: Theory and Research.New York: John Wiley & Sons, 1970. Print.Approaches to Behavior Pathology Ser.Hartikainen, K. M., Sun, L., Polvivaara, M., Brause, M.,Lehtimäki, K., Haapasalo, J., Peltola, J. (2014).Immediate effects of deep brain stimulation ofanterior thalamic nuclei on executive . Journal of Clinical and ExperimentalNeuropsychology, u/10.1080/13803395.2014.9135542*Kiehl, Kent A, and Morris B Hoffman. “The criminalpsychopath: history, neuroscience, treatment,and economics.” Jurimetrics vol. 51 (2011):355-397.Koenigs M. (2012). The role of prefrontal cortex inpsychopathy. Reviewsintheneurosciencences, , C., Wu, S., Luo, Y., Guan, Q., & Cui, F. (2018).Transcranial direct current stimulation of themedialprefrontal cortex modulates the propensity to help incostlyhelpingbehavior. NeuroscienceLetters, 674, 54-59.5*Sieger, T., Serranová, T., Růžička, F., Vostatek, P.,Wild, J., štastná, D., Jech, R. (2015).Distinct populations of neurons respond toemotional valence and arousal in the humansubthalamic nucleus. PNAS Proceedings of theNational Academy of Sciences of the UnitedStates of America, 112(10), .1073/pnas.1410709112Sturm, V., Fricke, O., Bührle, C. P., Lenartz, D.,Maarouf, M., Treuer, H., Lehmkuhl, G.(2012). DBS in the basolateral amygdalaimproves symptoms of autism and related selfinjurious behavior: A case report andhypothesis on the pathogenesis of thedisorder. Frontiers in Human Neuroscience, 3*Vachon, D. D., & Lynam, D. R. (2016). Fixing theproblem with empathy: Development andvalidation of the affective and cognitivemeasure of empathy. Assessment, 23(2), 135–149. https://doi.org/10.1177/1073191114567941Vitek, J. L. (Ed.). (2014). Deep brain stimulation :Technology and applications (volume erner, K. B., Few, L. R., & Bucholz, K. K. (2015).Epidemiology, comorbidity, and behavioralgenetics of antisocial personality disorder andpsychopathy. Psychiatric annals, 45(4), 195–199. doi:10.3928/00485713-201504
The etymology of the terms “antisocial” and “psychopath” can hold many negative connotations and are therefore commonly misused. The Diagnostic and Statistical Manual of Mental Disorders (DSM5) recognizes Antisocial Personality Disorder (ASPD) and psychopathy as a singular disorder