Transcription
How to Write5-MINUTE TREATMENT PLANSWithBarbara Griswold,LMFTAuthor, Navigating theInsurance Maze: TheTherapist’s CompleteGuide to Working withInsurance – AndWhether You Shouldtheinsurancemaze.comHandouts and CEs:theinsurancemaze.com/plansABOUT MEBarbara Griswold, LMFT 30 years in private practice Private practice consultant Author, Navigating the InsuranceMaze: The Therapist’s CompleteGuide to Working with Insurance -And Whether You Should, 8th ed. Taught hundreds of trainings oninsurance/documentation My mission: Help therapistsnationwide to feel as good aboutthe business side of their practiceas they do about their therapytheinsurancemaze.com2
AGENDA What is a Treatment Plan?Why We Don’t Do Treatment Plans -- And Why We ShouldWhat Should be in Your Treatment PlansQuestionsSample Treatment PlansHow to Update Your Treatment PlansQuestionsWe’ll go quickly! Get slide handout and if have questionsleft, contact me: ST, A CONFESSION.I lied.theinsurancemaze.com4
WHAT IS ATREATMENT PLAN? Treatment plans Notes “Roadmap” you write at startof treatment “.describes the patient'scondition and procedures thatwill be needed, detailing thetreatment to be provided andexpected outcome and expected duration of the treatment.”* Deluxe treatment plan vs. “treatment plan light”theinsurancemaze.com*--- www.lawinsider.com5RESULTS OF MY SURVEYOF 500 THERAPISTS“Do you routinely write treatment plans forclients?” 37% Yes, for all clients 23% Only for some clients 40% No“How confident are you in your plans?” Only 18% said they felt confidentabout their planstheinsurancemaze.com6
SURVEY: WHY AREN’T WE WRITING THEM?“I don’t see them as helpful” (50%) “They aren’t able to reflect the fluidity of therapy” “Goals feel confining” “I just include goals in progress notes”“I don’t have time” (25%) Keeping up with notes is hard; treatment plans are lower priority “I write them, but don’t have time to update them”“I don’t know how to write them” (25%)Other common responses: “I write them because they are required” “I only write them for insurance clients” “I only write one when facing an insurance plan review or audit”theinsurancemaze.com7SO, WHY SHOULD WE DO TREATMENT PLANS? Required by health plans Documentation reviews or pre- or post payment reviews Health plans may refuse to pay or ask for money back if you don’thave good documentation -- even out-of-network providers Required by many state laws and licensing boards Some ethics codes require (APA / AAMFT/ NASW codes don’t mention)ACA Code of Ethics 1.c “Counselors and their clients work jointly indevising counseling plans that offer reasonable promise of success andare consistent with the abilities, temperament, developmental level, andcircumstances of clients. Counselors and clients regularly review andrevise counseling plans to assess their continued viability andeffectiveness, respecting clients’ freedom of choice.”*CAMFT members: See Ethics Codes 1.10 and 2.7* – American Counseling Association, 2014 Code of Ethics8
BENEFITS FOR CLIENTS AND THERAPISTSTreatment plans can help clients: avoid feeling overwhelmed, by setting goals stay motivated, achieve more, boost self confidence feel more satisfied with treatment research suggests providing focus and structure leads tomore positive therapy outcomesPlans can help therapists: monitor progress, and demonstrate it to client demonstrate progress and need for treatment to insurance make treatment adjustments, when necessary build rapport, as client/therapist collaborate on visiontheinsurancemaze.com9“THE GOLDEN THREAD”Assessment dataDiagnosisTreatment PlanServicesProgress Notestheinsurancemaze.com10
TREATMENT PLANS: FAQs When should plan be written?Separate from notes?Insurance clients only?How can you save time? Have list of sample goals by diagnosis But. should NOT be cookie cutter Reflective of client lifestyle, race,culture, socioeconomic status Use check boxes?theinsurancemaze.com115 BUILDING BLOCKS OF A TREATMENT PLAN1. DIAGNOSIS2. GOALS (2 minimum recommended)3. OBJECTIVES -- how you’ll measuregoal is achieved (1-3 per goal)4. TIME FRAME For goals and objectives Estimated duration of treatment Tip: Make it 6 months or less5. INTERVENTIONS, Planned(3-5 minimum) Frequency / type of sessions Main in-session interventionstheinsurancemaze.com12
WHAT IS AGOAL? Describe in broad terms what ct. wants to accomplish in treatment Should be tied to diagnosis: focus on reducing symptoms/impairment May be stated positively or negatively. "Ct will improve workattendance" or "Ct will reduce absenteeism”Examples: “Increase ability to cope with anxiety without using substances” “Reduce frequency of angry interactions at work and at home” “Decrease anxiety related to public speaking”theinsurancemaze.com13“HOW DO I CHOOSE THERAPY GOALS?” In first session, ask client1. their therapy goals (what to ask)2. how they would know if they hadreached them Rewrite their goals to be measurable andsymptom-focused: “I want to feel like my old self again” “Stop my kid from being such a brat!” “I want to trust my husband again” If client has two diagnoses, usually shouldhave one goal for eachtheinsurancemaze.com14
WHAT IS AN OBJECTIVE?Definition: How will you measure goals are being achieved. It could be: Action-oriented first steps the client will take Screening questionnaire/measurement tool to gauge progressExamples of objectives include: An alcoholic with the goal to maintain sobriety might have theobjective to go to three 12-step or Rational Recovery meetings A ct. with goal of evicting a drug-addicted son may have objective todevelop a realistic eviction plan For a ct. with goal of reducing anxiety about coming out to parents,ct. will role-play with therapist, and first come out to trusted friendtheinsurancemaze.com15S.M.A.R.T. GOALS / OBJECTIVES*Specific: Try to include specific numbers/quantities in objectivesMeasurable: Goals like “improve self-esteem” would be hard tomeasure. Journaling and scores from assessment tools can help.Attainable: Ex. Is it realistic to set a goal for your client to leavehis/her abusive relationship?Relevant: Related to client diagnosis/distress (ex. if anxiety diagnosis,treatment plan should have one goal about anxiety reduction)Time-Limited:Deadlines ensure client is making progress and hittinglandmarks along the way.*Note: There are different versions of SMART Goals; this is just one16theinsurancemaze.com
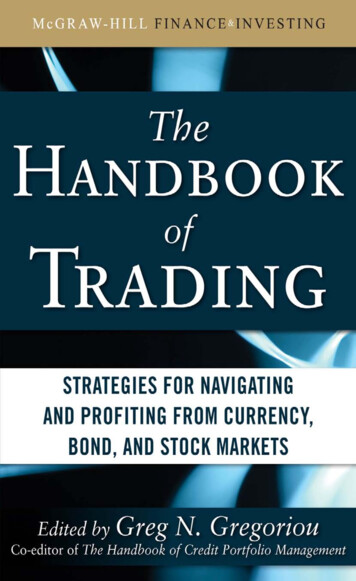
INTERVENTIONSWhat YOU will do to help the clientachieve their goals Modality (ind., couples, family, group) Frequency/length of sessions Treatment type (ex. CBT, DBT, EMDR) Key treatment methodsAVOID: “Build rapport and create safe space” Support / validate / normalize “Help ct. identify thoughts and feelings” “Help ct. cope with life problems / relationship issues”These are assumed or too vague: use clinical languagetheinsurancemaze.comGOALOBJECTIVESCt. will learn (andreport using) 2 toolsto deal with anxietyinstead of eatingReducecompulsiveeating whenanxiousCt. will keep log ofemotional eating, togather info aboutbehavior (triggers,frequency, progress)Ct. will reportemotional eatingno more thanonce weeklytheinsurancemaze.com17INTERVENTIONSWeekly individual CBT therapyExplore history of disorderedeating/secondary gains, helpidentify distorted cognitionsand emotional triggersTeach ct. techniques to dealwith anxiety, includingmindfulness, meditation,journaling, breathingexercises, and progressiverelaxationTherapist will help ct. writerelapse prevention plan,outlining how to use newcoping skills instead of eating18
MEDICAL NECESSITY:The Key to Insurance Coveragetheinsurancemaze.com19AN INCREASE INCHART REVIEWS?Due to Federal Parity Act andAffordable Care Act:Most clients now have unlimited sessionsregardless of diagnosis (some exceptions) BUT: Health plans can still refuse to cover visits they feel are not“medically necessary” “Medical necessity reviews” used to limit sessions or notreimburse, even for out-of-network therapists So .treatment plan and all notes must address medical necessity So if your notes aren’t great, get my Progress Notes Webinar.theinsurancemaze.com20
WHAT ARE HEALTH PLANS LOOKING FOR?MEDICAL NECESSITY CRITERIA DSM diagnosis; Z-code can’t usually be soleor primary (Adjustment Disorder usually OK) Necessary, not just desired Treatment goals can’t be just personal growth,self-esteem, feeling awareness, improved sex,better communication/relationships, careergrowth, improved life satisfaction/meaning Goals: Improve functioning/symptom reduction Appropriate frequency Symptoms impairing client -- ex. work, school,relationships, health/sleep, -- so say how Client is improvingtheinsurancemaze.com21QUESTIONS?If still have questions,contact me 75
GET YOUR DOWNLOADS! Treatment Plan Templates: Blank Template For client with AdjustmentDisorder with Depression For client with Anxiety Treatment Plan Updates w/each Child/Teen Therapy Goals Sample Interventions List Slide handouts Info on CE creditstheinsurancemaze.com/plans23CASE EXAMPLEYour Client,Cinderella’s PrinceCharmingYour Assessment: Met true love at ball, she ran out Has ghosted him She hasn’t returned texts He’s depressed, not sleepingtheinsurancemaze.com24
theinsurancemaze.com25GOAL #1theinsurancemaze.com26
GOAL #227INTERVENTIONStheinsurancemaze.com28
TREATMENT PLAN RESOURCES Can use Treatment Planners, ex: “The Complete Adult PsychotherapyTreatment Planner” and “The CouplesPsychotherapy Treatment Planner”(Practice Planners/Wiley) Treatment Planning Software inSimplePractice, TherapyNotes, etc. MY WARNINGS ABOUT THESE Consider DSM-5 (I’ll show you how)theinsurancemaze.com29CASE EXAMPLEYour Client,Snow WhiteYour Assessment: Depressed and bored Socially isolated Resentful towards dwarves Poor self-caretheinsurancemaze.com30
CHOOSING GOALS / OBJECTIVES FORSNOW WHITEDSM-5 Major Depression Criteria:1.2.3.4.5.6.7.8.9.10.Depressed mood most of the day, almost dailyLoss of pleasureWeight loss/gain, change in appetiteInsomnia/hypersomniaPsychomotor agitation or retardationFatigue or loss of energy nearly every dayFeelings of worthlessness or excessive guiltDiminished ability to think/concentrate; indecisivenessRecurrent thoughts of death/suicideSymptoms cause significant distress or impairment insocial/occupational/other areas31POSSIBLE GOALS/OBJECTIVES FOR SNOW WHITEGoal 1: Decrease in depression episodesObj 1: Ct. will report decrease in depression frequency,severity, duration (from daily to 1x weekly)Obj 2: Will score in Mild Range on PHQ-9Obj 3: Ct will report using 3 self-care tools learned in therapyto combat depressive triggers/episodesGoal 2: Ct. will demonstrate improved self-care and appetiteObj 1: Ct will be following self-care plan created withtherapist, including daily exercise, showering, healthy eatingGoal 3: Ct. will report decrease in social isolationObj 1: Ct will go to 3 meetings of the Disney Support GroupObj 2: Ct will initiate Zoom chat with friend once weeklytheinsurancemaze.com32
SOME POSSIBLE SNOW INTERVENTIONS1.2.3.4.5.6.7.8.9.10.Weekly CBT individual therapyIdentify coping strategies used successfully in pastAssign negative thinking journalCreate self care plan/depression coping planRefer for medication evaluation and coordinate careUrge development of/ use of support system; identify barriers toutilizationEducate client (and dwarves) about depression via written materialsGive insomnia CD to listen to before bedAssign daily exercise in woods to tire body, improve sleep, combatdepressionTeach assertiveness/ability to ask dwarves/friends for helptheinsurancemaze.com33CASE EXAMPLEYour Client,The Evil QueenYour Assessment: OCD: Obsessive thoughts, askingmirror “who is fairest of them all?” Jealousy outbursts. Wants to killthe pretty Snow White Work impairment: Performance ofroyal duties has suffered.theinsurancemaze.com34
CHOOSE GOALSUSING DSM DSM-5 OCD: Defines obsessions as:1. intrusive and unwanted recurrent and persistentthoughts, urges or images2. the individual attempts to ignore or suppress3. The obsessions are time-consuming4. The obsessions cause significant distresstheinsurancemaze.com35POSSIBLE PLAN FOR QUEEN WITH OCDGoal 1: Decrease in frequency of intrusive/unwanted thoughts/imagesObj 1: Ct. will be be able to practice thought-stopping when obsessionsoccur, and have new replacement positive affirmationsObj 2: Ct will report reduction in daily time spent on obsessionsGoal 2: When obsessive thoughts occur, they will be less intense, andcause less clinically significant distress and impairmentObj 1: Ct. will report no long avoiding townspeople due to obsessionsObj 2: Ct. will report better concentration at work, will be late no morethan once monthly and miss no more than 1 workday monthlytheinsurancemaze.com36
SOME POSSIBLE QUEEN INTERVENTIONS1.2.3.4.5.6.7.Mindfulness techniquesTeach thought-stopping and distraction techniques.Help client explore origins of beauty-anxietyChallenge irrational thinking and distorted self-talkHelp client create affirmationsTeach client breathing and relaxation exercisesDo thorough assessment of anger/violence history, currentcoping strategies, violence risk.8. Assign reading from “When Anger Hurts” to learn angermanagement skills.9. Teach DBT distress tolerance techniquestheinsurancemaze.com37HOW ABOUT COUPLES/FAMILY PLANS? With couples/families, just one plan isneeded: Pick Identified Client See webinar “Couples Therapy Billing,Documentation, and Ethical Dilemmas”at www.theinsurancemaze.com Goals can’t be solely to improverelationship, sex, trust, communication So goals for couples/family therapyplans may look very similar to individualtherapy plus possible added goalsincluding:theinsurancemaze.com38
SOME ACCEPTABLE COUPLES/FAMILY GOALS1. Address relationship issues, if contributing toclient symptoms or lack of functioning2. Assist family/partner to understand client’ssymptoms, and to respond more effectively3. Educate family/partner to improve clientcompliance with therapy goals4. Reduce negative impact of client’s conditionon partner or familytheinsurancemaze.com39COUPLE CASEEXAMPLEYour Clients, Beautyand the BeastYour assessment: Difficulty adjusting to new rel. A lot of verbal fighting Who is Identified Client? He is angry but anxious Adjustment Disorder with Anxietytheinsurancemaze.com40
Goal 1: Reduce frequency and intensity of verbal conflicts with partnerObj: Ct. will report less frequent and less severe anger episodes. Will bereporting verbal conflicts no more than once weekly, and conflicts will beshorter and less intenseGoal 2: Ct will deal more effectively with angerObj: Between sessions, ct and partner will be practicing Active Listeningand Time Outs and successfully de-escalating heated arguments whenthey occurInterventions: Partners will be asked to gather data about conflicts anddiscuss in sessions. Help couple identify conflict triggers and patterns. Willtake history of anger management in past relationships and family of origin.Teach Active Listening and Time Outs. In session, have clients use thesetools to facilitate calm communication and resolve conflictsANYTHING WRONG WITH THIS PLAN?theinsurancemaze.com41PLAN: CT. NOT READY FOR ALCOHOL ABSTINENCEGoal 1: Help client objectively assess if alcohol use is problematicObjective: Ct will gather one month’s data about alcohol use patternand ability to control alcohol intakeGoal 2: Ct will be coping with loneliness without alcoholObjective: Ct can identify 3 drinking triggers related to loneliness. Willbe practicing 3 alternate responses to loneliness without alcoholGoal 3: Build sober support systemObjective: Attend 3 AA/Rational Recovery groups, evaluate helpfulnessInterventions: Give MAST at intake. Review ct’s. alcohol use journal,assess for patterns/problems. Have ct. write/discuss history of substanceuse and negative consequences. Help ct identify emotional triggers andsituations that lead to alcohol overuse and make plan of alternate ways tocope with loneliness. Educate ct. on sober support options. Discuss ct.reactions to AA or RR to encourage engagement, if appropriate.42
PTSD CASEEXAMPLEYour client, Louse E. DriverYour assessment: Ct has had PTSD since caraccident, flashbacks Can’t drive on highway Can’t make left turnstheinsurancemaze.com43PTSD AFTER CAR ACCIDENT: GOALS/OBJECTIVESGoal 1: Report less intense emotional and/or physical reactionswhen exposed to reminders of the trauma/accident (driving)Objective: Ct. will report less than one flashback per week, andless anxiety when thinking or talking about accident, measuredby decrease in SUDS ratings (scale of 1-100)Goal 2: Client will have tools to successfully deal with anxietyObjective: Ct. will learn and utilize three coping skills to calmherself when exposed to trauma trigger (driving)Goal 3: Increase participation in previously-avoided activitiesObjective: Ct will report ability to drive on highway and to makeleft turns in car againtheinsurancemaze.com44
SOME POSSIBLE PTSD INTERVENTIONS Teach mindfulness, meditation, and relaxation techniques (progressiverelaxation, visualization, body scans/ breathing) Use CBT to help ct identify cognitive distortions that exacerbate fear Teach DBT distress tolerance techniques Provide Prolonged Exposure Therapy / Systematic Desensitization Ct will be given in vivo homework practices related to trauma/driving Ct will be asked to talk/write about trauma in detail, to help desensitize Help ct. understand trauma history, and connection to current trauma Use EMDR to help ct target and minimize effects of traumatic memories Consider medication evaluation referral / coordinate care withpsychiatristtheinsurancemaze.com45USING NOTES TO UPDATE THE PLAN Use progress notes to update the plan inbetween formal Plan updates Note changes in goals Track progress/lack of change If progressing, state what’s left to work on Document changes to plan Document Medical Necessity Mention diagnosis in each note? Get my webinar, “What’s Missing From YourCharts: Writing Great Notes” om46
HOW OFTEN TO UPDATE PLANS.AND HOW Not clearly outlined by most organizations How often may vary by your setting; 3-6 months? Can set update reminders in SimplePractice and TherapyNotes Medicare: It is expected that treatment plan “will be updated on a periodicbasis, generally at least every three months.” “Document plan at beginning of episode of care and whenthere is change, such as at periodic re-evaluations or whenclient has a new condition” “.if progress is not shown, show that treatment plan is beingadjusted as needed.”References: From https://tinyurl.com/medicaretxplan and Medicare Manual Pub. 100.08 Chap 3sec 3.3.2.1.1. (2 B.) https://tinyurl.com/MedicareManualChap347HOW TO UPDATETREATMENT PLANS For each goal and objective,identify progress, and giveexamples Name what is left to work on, orsymptoms that remain Download sample plans andupdates attheinsurancemaze.com/planstheinsurancemaze.com48
CASE EXAMPLE:Treatment Plan Update forclient with meeting anxietyGoal: Decrease anxiety relatedto work meetingsObj. 1: Report feeling less anxiouswhen in meetings, no longer missmeetings, speak once per meetingObj. 2: Keep anxiety/distortedthoughts journal, and be able toidentify and challenge distorted thoughts that fuel anxietytheinsurancemaze.com4950
TREATMENT PLAN ADJUSTMENTStheinsurancemaze.com51QUESTIONS?If you still have questions orcomments, contact me attheinsurancemaze.com/plansAll CE info, recording link, andhandouts will be there, also5275
HOW CAN I HELP YOU?Handouts/CEs: theinsurancemaze.com/plansVisit theinsurancemaze.com/store for Pre-Recorded Webinars: “What’s Missing From Your Charts: Writing Great Notes” “Telehealth Billing” “Couples Billing & Ethical Dilemmas” Insurance Webinar My book My Forms Packet (16 Essential Forms) My Billing Service List Schedule a consultationBarbara Griswold, LMFTtheinsurancemaze.combarbgris@aol.com 408-985-084653
TREATMENT PLAN RESOURCES Can use Treatment Planners, ex: “The Complete Adult Psychotherapy Treatment Planner” and “The Couples Psychotherapy Treatment Planner” (Practice Planners/Wiley) Treatment Planning Software in S