Transcription
Quality Reporting and RegistryUpdate: Challenges and Strategiesfor SuccessHeather Smith, PT, MPHSeptember 13, 20141
SETTING THE STAGE FORTOMORROW 2014 American Physical Therapy Association. All rights reserved. All reproduction or redistribution prohibited.2
The Present and Future of HighQuality Patient Care 2014 American Physical Therapy Association. All rights reserved. All reproduction or redistribution prohibited.3
Quality Reporting and PTs in 2014VMPQRSFLRPrivatepayer 2014 American Physical Therapy Association. All rights reserved. All reproduction or redistribution prohibited.4
SGR Reform and Quality ReportingPRE SGRPOST SGR(proposed)PQRS Quality reporting under MedicarePart B under several differentprograms including PQRS. Variable penalties tied to eachprogram (2.0% ) Current programs replaced by Merit‐BasedIncentive Payment System (MIPS) in 2018 Performance based on: quality, resource use,meaningful use and clinical practice improvementactivitiesFLR FLR participation is required by all FLR will be expanded to include additional variableproviders billing therapy servicesas identified by the Secretary and stakeholders inunder Medicare part B2017 (demographic info, diagnosis, severity, Claims based data submissionexpanded ICF, etc) Condition of payment Data to be submitted via web‐portal or othermechanism Data utilized to support new payment system5(case mix adjustments, episodic payment)
Future of Medicare Part B QualityReportingPrivatePayersPQRSFLRFuture reportingsystemsPTPCSSGRPAC 2014 American Physical Therapy Association. All rights reserved. All reproduction or redistribution prohibited.6
Quality ReportingTodayFutureSeparate and distinct reporting programs(FLR, PQRS, MU, etc.)One quality program under Medicare PartBVaried methods of data reportingElectronic reporting via patient registries,EHRHigh percentage of process measuresFocus on outcome measures andpatient/family centered measuresMultiple measures of patient functionOne measure of global patient functionthat crosses the continuum of careIdentification of measure gaps bygovernment/ national measurementgroupsIncreasing role of associations in thecreation of meaningful quality measuresfor professionals 2014 American Physical Therapy Association. All rights reserved. All reproduction or redistribution prohibited.7
REVIEWING THE NOW: FLR, PQRS,VM 2014 American Physical Therapy Association. All rights reserved. All reproduction or redistribution prohibited.8
Current Quality Reporting Programs Under MedicareHealthcare SettingInpatient(Acute Care Hospitals)Quality Program(s)Mandatory ReportingPayment Incentive/PenaltyIQR, Readmissions &VBPYesYesP4R & P4P in 2013Long Term Care Hospitals (LTCH)Beginning in 2014YesYesP4R Penalty 2%Inpatient Rehabilitation Facilities(IRF)Beginning in 2014YesYesP4R Penalty 2%MDS 3.0YesNoHospiceBeginning in 2014YesYesP4R Penalty2%Home HealthOASIS, HH CAHPSYesYesP4R Penalty 2%PQRSNo, payment adjustmentsfor non‐participationbeginning in 2015 (based on2013 data)Yes P4R Incentive0.5% through 2014,Penalty ‐2.0% 2016 andbeyondValue‐based Modifier(VM) ‐proposed CY2017No‐ tied to participation inPQRSYes P4P 4.0x to ‐4.0%Functional LimitationReporting (FLR)YesCondition of paymentSkilled Nursing Facilities (SNF)Outpatient9
Functional Limitation Reporting(FLR)Middle Class TaxRelief Act of 2012FLR OngoingFebruary 20122014Congress mandatesCMS to collectfunctional info onMedicarebeneficiariesreceiving therapyservices under Part BMedicarecontinues to workthrough systemmodifications;anticipatingfuture evolutionsof FLRFLR ImplementationJanuary 1, 2013Testing phase beginsfor the collection offunctional dataFinal Physician FeeSchedule RuleFLR PaymentAdjustment PhaseNovember 2012October 1, 2013Outlines theregulations aroundthe new claims‐based reportingprogram for therapyservicesOriginally slatted forJuly 1, 2013 this wasdelayed until October1; providers beganreporting processingissues in midNovember 2014 American Physical Therapy Association. All rights reserved. All reproductionor redistribution prohibited.10
From Law to linesCMSMCTRA2012 Final Physician FeeSchedule, FAQs, st CoastWPS 2014 American Physical Therapy Association. All rights reserved. All reproduction or redistribution prohibited.Noridan11
Initial FLR Claims Processing IssuesClaims splitting (1500)Delayed/ out of sequence processingIncorrect visit countsRequired reporting at 10th/20th/etc despite earlyreporting Issues with 3Gcode submission with an active POC Problems with 60 day discharge Edits in CWF on May 6 fixed many of the issues 2014 American Physical Therapy Association. All rights reserved. All reproduction or redistribution prohibited.12
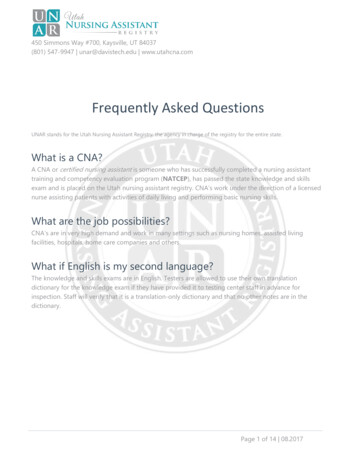
Causes of FLR Claim Rejections60NUMBER OF unt DiscrepancyDelayed PaymentClaims SplittingProcessing Out of OrderIssues With 60 Day RuleUnsuccessful Resubmission of Claim2014‐04 2014 American Physical Therapy Association. All rights reserved. All reproduction or redistribution prohibited.13
Current FLR Claims ProcessingIssues Problems with 60 day discharge Edits planned on or around September 15 Claims that were rejected prior to May 6 that havecorrect FLR data should be resubmitted for payment All rejected claims should be reviewed to checkaccuracy of FLR codes Still investigating issues case by case– Claims splitting 2014 American Physical Therapy Association. All rights reserved. All reproduction or redistribution prohibited.14
Examples of FLR ErrorsSimple or clerical errors Use of 0.00 instead of 0.01 Leaving off the GP or severity modifiers Submitting the wrong Gcode (discharge vs current)Misunderstanding of FLR guidance Reporting a single FLR code instead of two codes Changing categories mid episode without ending reporting onoriginal limitation Issues with tracking (beneficiary/ facility/ therapy service) 2014 American Physical Therapy Association. All rights reserved. All reproduction or redistribution prohibited.15
PT Participation in PQRS Total of 16individual measures 1 measures group Claims‐basedremains the mostpopular reportingmechanism (7claims measures in2014) 2014 American Physical Therapy Association. All rights reserved. All reproduction or redistribution prohibited.16
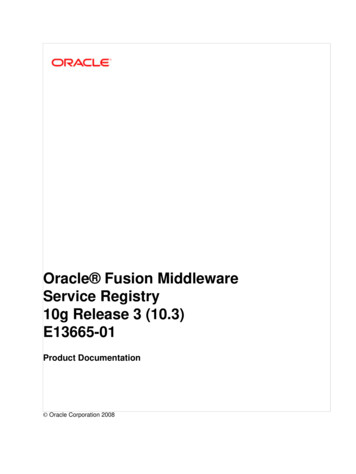
PT and OT PQRS Claims Individual2009Claims Group20102011Registry Individual2012Registry Group 2014 American Physical Therapy Association. All rights reserved. All reproduction or redistribution prohibited.17
Recent PPS Survey on PQRS Response: 540 members 85.0% participating in PQRS in 2014– The top reason sited for non‐participation: practice doesnot have resources to manage the PQRS reporting burden;we are willing to take the 2.0% penalty to avoid thereporting burden (8.0%) 83.7% report via claims 76.5% have never accessed a feedback report– Only 31.0% have received a bonus in past years 2014 American Physical Therapy Association. All rights reserved. All reproduction or redistribution prohibited.18
2014 Top Reported Measures for PTs#Measure DescriptionReporting %128Preventive Care and Screening: Body Mass Index (BMI) Screeningand Follow‐up34.1%130Documentation and Verification of Current Medications in theMedical Record45.7%131Pain Assessment Prior to Initiation of Patient Treatment65.7%154Falls: Risk Assessment48.5%155Falls: Plan of Care42.4%182Functional Outcome Assessment55.7%Based on on PPS survey results 2014 American Physical Therapy Association. All rights reserved. All reproduction or redistribution prohibited.19
Future Trends PQRSMove to 9 measures for successful reportingElimination of process based measuresMove toward outcomes measuresMeasures groups required to have at least 6measures Move toward electronic data submission – Increased use of registry, QCDR and EHR reporting 2014 American Physical Therapy Association. All rights reserved. All reproduction or redistribution prohibited.20
The Value‐Based Modifier (VM)Program VM was mandated by Section 3007 of the AffordableCare Act, to begin by 2015. This program is separatefrom PQRS. CMS will begin applying VM under the MedicarePhysician Fee Schedule (MPFS) in CY2015 (usingCY2013 data). The proposed CY2015 MPFS rule includes a proposal toexpand the program in CY2017 (using CY2015 data) toinclude:– Nonphysician Eligible Professionals (EPs) this includes PTs– Solo practitioners and groups of 2‐9 providers 2014 American Physical Therapy Association. All rights reserved. All reproduction or redistribution prohibited.21
VM Program ntsPhysician groups over 100providers*Physician groups over n EligibleProfessionals (EPs) in groups 2‐9AND solo providers2017‐1.0% to 2.0x‐2.0% to 2.0x‐4.0% to 4.0x*Group size determined by number of total eligible professionals 2014 American Physical Therapy Association. All rights reserved. All reproduction or redistribution prohibited.22
The Value‐Based Modifier (VM)and PTs The proposal to include PTs in the VM programwould begin in CY2017, however this would bebased on the PTs performance in 2015. Eligible PTs (in private practice‐ billing on the1500 form) who do not participate OR who fail tosuccessfully reporting under PQRS in CY2015 willbe assessed a ‐2.0% penalty under the PQRSprogram in CY2017 AND a ‐4.0% penalty underthe VM program CY2017. 2014 American Physical Therapy Association. All rights reserved. All reproduction or redistribution prohibited.23
The Value‐Based Modifier (VM)and PTs The VM program has a quality tieringmethodology that takes into account bothquality and cost.– The quality portion of the methodology is basedlargely on PQRS performance.– The cost portion of the methodology would nottypically apply to PTs and PTs would be given anaverage rating on this section based on CMSguidelines. 2014 American Physical Therapy Association. All rights reserved. All reproduction or redistribution prohibited.24
PQRS and VM in for PTs CY2015PQRS CY2015(calculated on NPI/TIN)Claims as Individuals: Report on 6 measures(all available PT measures) for 50% or moreof all Medicare Part B FFS patients.NO penalty in CY2017.PQRS Registry as Individuals: Report on 9measures (or if less than 9 available 8‐1measures) for 50% or more of all MedicarePart B FFS patients.NO penalty in CY2017.GPRO in a PQRS Registry: Report on 9measures (or if less than 9 available 8‐1measures) for 50% or more of all MedicarePart B FFS patients.NO penalty in CY2017.Non participation or failure to meetsuccessful reporting requirements.‐2.0% payment adjustment in CY2017.Value‐Based Modifier CY2015(calculated on TIN)Solo practitioners or groups of 2‐9 PTs or othernonphysician EPs (at least 50% of PTs/ nonphysicianEPs reporting as individuals in practice must besuccessful in PQRS CY2015).Neutral or upward payment in CY2017.Groups of 10 PTs or PTs and other EPs (at least 50% ofPT’s/ EPs reporting as individuals in group must besuccessful in PQRS in CY 2015).Downward, neutral or upward payment adjustment inCY2017.Solo practitioners or groups of 2‐9 PTs/ nonphysicianEPs AND groups of 10 PTs or PTs/ EPs where less than50% of PT’s/ EPs in group are successful in PQRS ORGroups and solo practitioners who do not participate inPQRS.25‐4.0% payment adjustment in CY2017.
BACK TO THE FUTURE: THEREGISTRY 2014 American Physical Therapy Association. All rights reserved. All reproduction or redistribution prohibited.26
27What is the Registry?The Physical Therapy OutcomeRegistry is an organized system tocollect data to evaluate patientfunction and other clinically relevantmeasures for the population ofpatients receiving physical therapyservices. The registry will serve toinform reimbursement, improvepractice, fulfill quality reportingrequirements, and promote research.
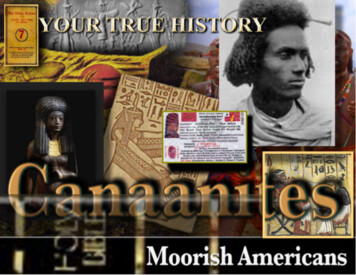
28Registry Hub & Spoke inics Allow for data to be gatheredacross the continuum of careFacilitate bi-directionalcommunication
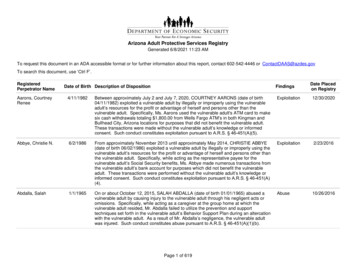
29PT Outcome Registry Guide payment policy Inform paymentcontract negotiations Demonstrate the valueof PT services Promote healthservices research Determine clinicalpractice patterns Assess adherence toCPG’sPaymentPracticeResearchQuality Fulfill quality reportingrequirements (Medicare) Support qualityimprovement initiatives
30What Data is in the Registry?Core Data Set (All ality DataPQRSFLRModules (CPGs)Intervention dataCondition specificoutcomes
31Benefits of ParticipationEnhancePatient CareImprove yourPracticeGrow yourBusiness Improve patientoutcomes Increase patientsatisfaction Improve physicaltherapist decisionmaking Further developbest practices Support qualityimprovementinitiatives Benchmark PTand practiceperformance Improveefficiency Maximizeproductivity Justify services topayers Identifytraining/educational opportunities Objectivelymarket yourpractice to avariety of payersand consumers Prove the valueof your practice Differentiate yourpractice in the PTmarket Increase referrals ements Fulfil PQRSrequirments Easily accessPQRS feedbackreports
32Registry Timeline2016 &BeyondContinuedPTOR growth2014Testing andpilot launch2015Full launch ofPTORhttp://www.apta.org/Registry
That the physical therapy profession uses standardized collection, analysis,and dissemination of intervention and outcomes data as a regular part ofpractice at all levels to determine what interventions best improve the healthof individual and society and to identify and emulate the positive deviantswithin our clinical communities.‐Alan Jette; Face into the StormQUALITY IN THE PRESENT 2014 American Physical Therapy Association. All rights reserved. All reproduction or redistribution prohibited.33
Quality Strategies for PTs Be aware of the quality environment– Fee schedule rules/ ingBilling/FeeSchedule/– www.apta.org/pqrs (VM site if the rule finalizes)– www.apta.org/flr– Other quality orPerformance/– www.apta.org/registry 2014 American Physical Therapy Association. All rights reserved. All reproduction or redistribution prohibited.34
PT and the Quality FutureOpportunities Moving towardsharmonization of standardfunctional outcome dataset/ tool Measure development andcollaboration RegistryChallenges Responding to the everchanging qualityenvironment‐ trying to stay“ahead of the curve” Need for more PT specificmeasures Future of FLR Integrating QI into practice 2014 American Physical Therapy Association. All rights reserved. All reproduction or redistribution prohibited.35
QuestionsAdvocacy@apta.orgOR800‐999‐2782 ext 8511 2014 American Physical Therapy Association. All rights reserved. All reproduction or redistribution prohibited.36
The Physical Therapy Outcome Registry is an organized system to collect data to evaluate patient function and other clinically relevant measures for the population of patients receiving physical therapy services. The registry will serve to inform reimbursement, improve practice, fulfill