Transcription
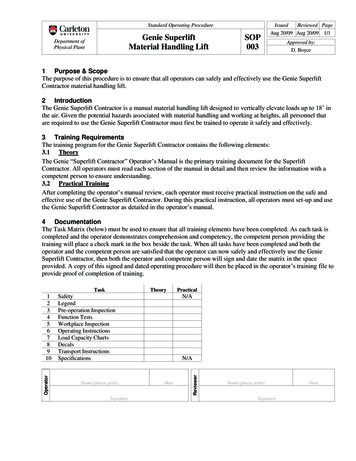
To lift or recut: Changing trendsin LASIK enhancementRoy S. Rubinfeld, MD, David R. Hardten, MD, Eric D. Donnenfeld, MD,Raymond M. Stein, MD, Douglas D. Koch, MD, Mark G. Speaker, MD, PhD,Joseph Frucht-Pery, MD, Anthony J. Kameen, MD, Gerald J. Negvesky, MDPurpose: To report serious complications caused by recutting laser in situ keratomileusis (LASIK) flaps for enhancement and reconsider the current preferredmethod of LASIK enhancement.Setting: Multiple surgeon practices.Methods: This retrospective noncomparative nonconsecutive case series comprised LASIK patients in the private practices of 9 experienced refractive surgeons and those reported in a survey of refractive surgeons. Case histories,refractions, corneal topographies, slitlamp photographs, and measurements of uncorrected and best corrected (BCVA) visual acuity after recutting LASIK flapswere collected. Surveys of refractive surgeons and an analysis of changing practice trends among the authors and these surgeons were assessed.Results: In 12 cases, significant loss of BCVA and subjective visual difficulties resulted from recutting LASIK flaps. Most surveyed surgeons had changed theirpractice from recutting to lifting flaps even 9 to 10 years postoperatively withgood results.Conclusion: Recutting flaps for enhancement should be avoided unless other alternatives are unavailable.J Cataract Refract Surg 2003; 29:2306–2317 2003 ASCRS and ESCRSResidual refractive errors commonly occur after laserin situ keratomileusis (LASIK). Surgical management of these residual errors by excimer laser photoablation (enhancements) can be performed by lifting theflap, by cutting a new flap, or by surface ablation.Considering the current popularity of LASIK, if enhancements are required in only 10% of cases, tens orpossibly hundreds of thousands of LASIK enhancementprocedures will be performed every year in the UnitedStates alone. Although we believe that most surgeonsperform enhancements by lifting flaps, many textbooks,courses, and journal articles suggest that enhancementscan be routinely performed by recutting LASIK flaps 3or more months after the primary LASIK procedure.1–11In this paper, we report the first series of seriouscomplications induced by recutting flaps for routineLASIK enhancement. We propose that the serious natureof these complications and the results of a survey of experi 2003 ASCRS and ESCRSPublished by Elsevier Inc.enced refractive surgeons warrant reevaluation of the advisability of recutting flaps for LASIK enhancement.Patients and MethodsCase histories of patients with complications after recutting LASIK flaps were collected from 9 refractive surgeons.Each contributor reviewed the patient’s chart to collect standardized information about the case. Fifty refractive surgeonsaffiliated with TLC Vision were surveyed via an Internetquestionnaire. Four e-mail reminders were sent to the surgeons to encourage completion of the survey. The surveyquestions are shown in Figure 1.Summary of CasesTwelve eyes of 12 patients developed significant complications following flap recutting for enhancement of previousLASIK surgery. The mean age of the patients at the time of theinitial LASIK surgery was 37.8 years 7.7 (SD) (range 24to 47 years). The mean preoperative spherical equivalent (SE)was 6.23 0.78 diopters (D) (range 3.75 to 9.00 D)0886-3350/03/ –see front matterdoi:10.1016/j.jcrs.2003.08.013
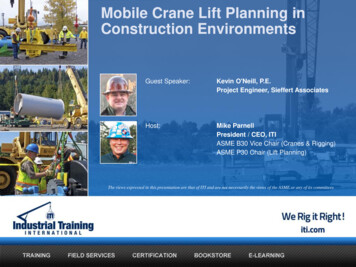
LIFT OR RECUTin the 10 myopic eyes and 4.69 1.68 D (range 3.50to 5.88 D) in the 2 hyperopic eyes. All patients had a bestcorrected visual acuity (BCVA) of 20/20; normal pachymetry;and symmetrical, unremarkable topographies before surgery.After the initial procedure, the mean best spectacle-correctedvisual acuity (BSCVA) was 20/20 (range 20/20 to 20/25)and the mean SE was 0.33 2.02 D. Before enhancement,no eye lost 2 or more lines of BSCVA.In 4 eyes, flaps were recut with the microkeratome usedin the initial procedure but with a thicker plate. Five eyeswere recut with the same microkeratome and the same plate,and 1 eye was recut with a different microkeratome with thesame plate depth. Complete data were not available for 2 eyes.Six eyes in the series were right eyes and 6, left eyes. Afterenhancement by recutting, the mean uncorrected visual acuity (UCVA) was 20/63 (range 20/30 to 20/400), the meanSE was 0.49 1.68 D, and the mean refractive cylinderwas 1.48 1.02 D. The mean time to recutting after theprimary LASIK procedure was 11.5 months (range 5.5 to26.0 months). Seven eyes lost 2 or more lines of BSCVA;however, all patients had visually significant complaints suchas monocular diplopia, glare, loss of contrast sensitivity, ghosting, and poor quality of vision. The details of the 12 cases aregiven in Table 1. Selected cases are reported below.Case 1A 45-year-old woman had uneventful bilateral LASIKfor moderate myopia. A 160 m plate was used with theAutomated Corneal Shaper威 microkeratome (Bausch & LombSurgical), and a Visx laser was used for the ablation. Postoper-Accepted for publication September 4, 2003.From Washington Eye Physicians and Surgeons (Rubinfeld), ChevyChase, Maryland, Georgetown University Medical Center (Rubinfeld)and Washington Hospital Center (Rubinfeld), Washington, DC; Minnesota Eye Consultants (Hardten) and University of Minnesota (Hardten), Minneapolis, and Regions Medical Center (Hardten), St. Paul,Minnesota; and Manhattan Eye, Ear and Throat Hospital (Donnenfeld), New York, New York, USA; Bochner Eye Institute (Stein) andUniversity of Toronto (Stein), Toronto, Ontario, Canada; Cullen EyeInstitue, Baylor College of Medicine (Koch), Houston, Texas, and NewYork Eye and Ear Infirmary, New York Medical College (Speaker),New York, New York, USA; Hadassah University Hospital (FruchtPery), Jerusalem, Israel; Greater Baltimore Medical Center (Kameen),Baltimore, Maryland, and Pocono Eye Associates (Negvesky), EastStroudsburg, Pennsylvania, USA.Presented in part at the annual meetings of the American Academy ofOphthalmology and the International Society of Refractive Surgery,New Orleans, Louisiana, USA, November 2001.None of the authors has a proprietary interest in any product mentioned.Reprint requests to Roy S. Rubinfeld, MD, Washington Eye Physicians &Surgeons, Suite 950, 5454 Wisconsin Avenue, Chevy Chase, Maryland20815, USA.Figure 1. (Rubinfeld) Survey sent to 50 refractive surgeons.atively, the patient’s left cornea developed mild to moderatediffuse lamellar keratitis (DLK) and epithelial ingrowth,which were treated with topical corticosteroid drops, liftingthe flap, and removing the epithelium. At 5.5 months, theleft eye remained somewhat myopic. The UCVA was 20/50and the BSCVA, 20/20.An enhancement procedure was performed using thesame microkeratome with a 180 m plate to cut a deeperflap. After the microkeratome pass, a subtle, thin, opalescentmembrane was observed in the bed; it was carefully repositioned without the use of saline solution and refloating. Therepositioning appeared satisfactory, and a small myopic lasertreatment was applied. The flap was then carefully replaced.The appearance of the flap under the operating microscopewas excellent, and the slitlamp examination 30 minutes aftersurgery showed excellent flap position.J CATARACT REFRACT SURG—VOL 29, DECEMBER 20032307
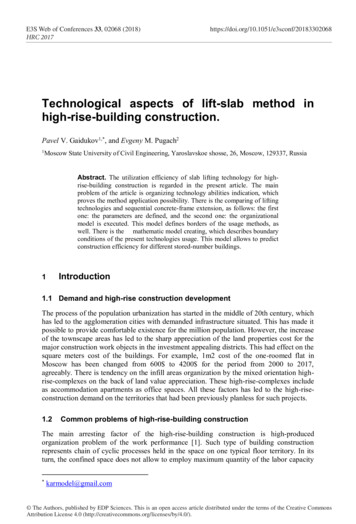
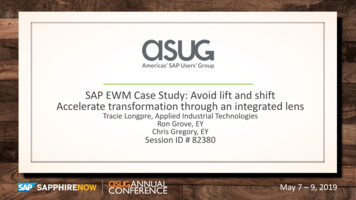
LIFT OR RECUTTable 1. Summary of 12 cases with complications after flap eratomePlate Depth ( m),Suction Ring Size (mm)Post-Enhancement(Initial Procedure/Enhancement)MRx1 8.00 1.75 100 1.75 1.75 92ACS160/180Pl 3.25 102 3.50 sphereHansatome180, 9.5/180, 9.5 1.50 0.50 103 8.50 2.75 110 0.50 1.00 60ACS180/180Too irregular to obtain4 8.50 sphere 5.00 1.00 50UnknownUnknown 5.50 1.00 585 6.25 0.25 80 1.00 sphere6 6.00 0.50 160 1.25 0.50 757 2.25 sphere 10.25 2.50 100 1.00 sphereHansatome160, 8.5/180, 9.5 0.25 1.00 132CB160/180 1.50 1.50 155Hansatome160, 8.5/180, 9.5 1.25 0.50 58 3.75 sphere 1.25 0.50 135Hansatome160, 9.5/160, 9.5 0.25 1.00 1359 5.50 0.75 13 2.50 1.25 171Hansatome(initial procedure)/ACS (enhancement)160/160, 9.5 0.25 1.75 4310 4.50 sphere 0.75 1.25 40HansatomeUnknown/180, 9.5 1.50 .75 17011 6.50 1.00 90 1.00 0.75 85Hansatome180, 8.5/180, 9.5 2.00 1.50 4512 5.25 0.75 15 1.75 sphereHansatome180, 8.5/180, 9.5 1.75 3.50 105One day after the enhancement procedure, a linear discontinuity or crease was noted in the anterior corneal stroma,oriented obliquely and superotemporally on slitlamp examination. The UCVA and BSCVA were 20/400. There wassome flap edema, although the flap position was excellent.Topical corticosteroids (prednisolone phosphate) were applied every hour for several days. No significant improvementin BCVA was noted during 1 week of this treatment. Twoweeks after the enhancement procedure, the flap was liftedand attempts were made to reposition the thin lamellar tissue.Despite the surgical procedure and continued treatment withtopical prednisolone phosphate, 19 months later the patienthad severe irregular astigmatism of 8.0 D (Figure 2) and aUCVA of 20/40 with severe ghosting, diplopia, and extremelypoor subjective quality of vision. Slitlamp examination usingretroillumination (Figure 3) demonstrated a linear lamellardiscontinuity in the area of irregular astigmatism noted onpostoperative topography. The final refraction in the left eyewas plano 3.25 10, which yielded a poor-quality BCVAof 20/40 to 20/30.Subsequent attempts to surgically repair the patient’sirregular astigmatism included flap elevation, removal of thestromal sliver, and phototherapeutic keratectomy (PTK) (Figures 4 and 5), but there was no improvement in BSCVA.myopia 12 months after the primary procedure. A new flapwas created using the same microkeratome and plate, andthe same laser was used for the ablation. A subtle tag ofperipheral corneal tissue was noted at the time of the procedure but did not appear clinically significant. Postoperatively,the patient complained of poor vision in the right eye. TheCase 3A 46-year-old woman had uneventful bilateral LASIKfor moderate myopia with an Automated Corneal Shapermicrokeratome using a 180 m plate and the Visx Star laser.The patient had bilateral LASIK enhancement for residual2308Figure 2. (Rubinfeld) Axial topographic map of Case 1 showingsevere irregular astigmatism after recutting for enhancement.J CATARACT REFRACT SURG—VOL 29, DECEMBER 2003
LIFT OR RECUTTable 1. (cont).Timing of Surgical InterventionsFinalUCVAFinalBSCVA5.5DLK, ingrowth, irreg. astig.Flap relifting, tissue repositioning, tissue excision, PTK20/4020/30 27.0Irreg. astig.None20/3020/30 312.0Irreg. astig.Flap relifting, tissue repositioning 220/20020/20012.0Irreg. astig.None20/40020/606.013.09.0Irreg. astig.None20/5020/25Irreg. astig., ingrowthFlap relifting, removal of ingrowth20/8020/50Irreg. astig.None20/5020/3012.0Irreg. astig., striaeFlap relifting, hyperthermic treatment of striae20/4020/2526.0Irreg. eg. astig.None20/6020/605.0Irreg. astig.None20/5020/30BSCVA best spectacle-corrected visual acuity; DLK diffuse lamellar keratitis; Ingrowth epithelial ingrowth; Irreg. astig. irregular astigmatism;MRx manifest refraction; PTK phototherapeutic keratectomy; UCVA uncorrected visual acuityUCVA and BSCVA were 20/200 with complaints of glareand diplopia.Slitlamp examination of the right eye with retroillumination through a dilated pupil revealed a 5.0 mm oblique ridgein the center of the pupil. The flap in the right eye was lifted,and a rolled edge of thin lamellar tissue was found in thebed corresponding to the ridge seen on slitlamp illumination.The edge was unrolled and the flap replaced and meticulouslyrepositioned. The patient’s vision did not improve, and theridge was present on retroillumination slitlamp examination(Figure 6). Two weeks later, a second attempt was made tosmooth the bed in the right eye without success. Irregularastigmatism was visible on topography (Figure 7). The Snellen visual acuity and subjective visual quality remained unchanged. A rigid, gas-permeable (RGP) contact lens wasfitted, which provided the patient with 20/20 visual acuity.details are unavailable. Two and a half years after the enhancement procedure, haze and scarring were visible in the lefteye (Figure 8) and a linear discontinuity in the flap could beseen on retroillumination slitlamp photographs. Topographyrevealed 8.0 D of irregular astigmatism over the visual axis(Figure 9), and the patient’s subjective visual acuity remainedCase 4A 46-year-old woman had bilateral LASIK for moderatemyopia outside the U.S. The type of microkeratome andlaser were not known. Postoperatively, the patient had flapedema and haze that were treated with prednisolone acetatedrops and sodium chloride 5% drops and ointment. Theedema and haze cleared but the left eye regressed; the BCVAwas 20/20 with 5.00 1.00 50.One year after the LASIK procedure, the surgeon recutthe flap and noted a “fillet” of tissue in the stromal bed,which was noted to be “wrinkled” after the microkeratomepass. Additional laser treatment was applied, although surgicalFigure 3. (Rubinfeld) Retroillumination slitlamp photograph of Case1. Note the discrete, semicircular discontinuity in the stroma (arrow)caused by a sliver of stroma produced by recutting the flap.J CATARACT REFRACT SURG—VOL 29, DECEMBER 20032309
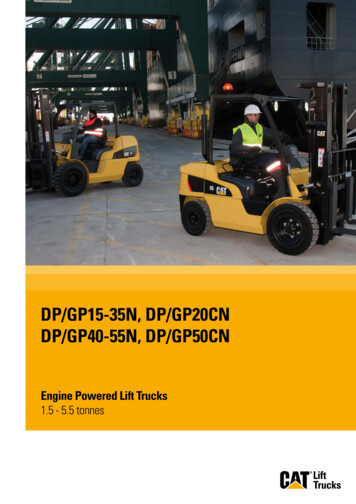
LIFT OR RECUTFigure 4. (Rubinfeld) Lamellar sliver of stromal tissue found on eleva-Figure 5. (Rubinfeld) Surgical removal of lamellar stromal tissue de-tion of the flap in Case 1. This lamellar tissue was induced by recuttingthe flap, and it could not be accurately repositioned (courtesy of LeeT. Nordan, MD).scribed in Figure 4 (courtesy of Lee T. Nordan, MD).extremely poor. The UCVA was 20/400, and the BSCVAwas 20/60 with 5.50 1.00 58. The patient complainedof severe glare, diplopia, and poor contrast and quality ofvision. An RGP contact lens improved the vision in this eyeto 20/30, but the patient was contact lens intolerant.Case 6Figure 6. (Rubinfeld) Retroillumination slitlamp photograph of foldedstromal sliver (arrow) under the LASIK flap in Case 3.Figure 7. (Rubinfeld) Axial topographic map of irregular astigmatismin Case 3 induced by flap recutting.2310A 37-year-old man had uneventful bilateral LASIK formoderate myopia with a manual CB microkeratome (Moria)using a 160 m plate and the Visx Star laser. Thirteenmonths postoperatively, an enhancement was performed inthe right eye for residual myopia. The surgeon recut the flapwith the CB microkeratome using a 180 m depth plate.The procedure was complicated by multiple lamellar sliversinvolving the flap and bed. The patient was referred forconsultation and further management.Three weeks after the complication occurred, the UCVAin the right eye was 20/80 and the BSCVA was 20/60 with arefraction of 0.25 1.50 175. On slitlamp examination,there appeared to be striae manifested by a few visible linesin the flap; these were thought to be slivers of displacedcorneal tissue. The flap was lifted, and an attempt was madeto reposition the corneal slivers. One week later, the BCVAwas 20/40 with a refraction of 1.75 1.75 155.Three and a half months later, a focal area of epithelialingrowth that extended 2.0 mm was noted. Over the next9 months, the epithelial ingrowth progressed. At this time,multiple focal areas of epithelial ingrowth extending to thepupil were noted (Figure 10). The outer flap edge was liftedin the operating room, but the epithelial cells were not locatedat this interface (Figure 11). The flap was then repositioned.One month later, the patient was brought back to the operating room and the inner flap edge was lifted and theepithelial cells gently removed with a spatula. One monthlater, a relatively clear interface was noted but the BSCVA wasJ CATARACT REFRACT SURG—VOL 29, DECEMBER 2003
LIFT OR RECUTFigure 8. (Rubinfeld) Slitlamp photograph of haze present in corneaFigure 9. (Rubinfeld) Axial topography demonstrating 8.0 D of irreg-of Case 4 2.5 years after a microkeratome transected the original flapplane during recutting for enhancement.ular astigmatism caused by recutting the flap in Case 4.20/50 with 1.50 1.50 155. The patient complained ofglare, diplopia, and poor quality of vision. One year later,the BSCVA remained 20/50 secondary to irregular astigmatism. The patient is considering a lamellar graft.Nine months postoperatively, an enhancement was performed for residual myopia by cutting a new flap using theHansatome with a 180 m plate and a 9.5 mm suction ring.Upon elevating the flap, the surgeon noted separation of ashallow flap from the deeper flap, creating 2 corneal flaps.The thin interface flap was repositioned carefully (Figure12), and excimer laser ablation was performed. After salineirrigation and repositioning with Weck-cel威 sponges (Medtronic Solan), the superior flap was laid down on top of theinterface lamellar tissue. A bandage contact lens was appliedand left in place for 3 days.Case 7A 30-year-old man had bilateral LASIK for moderateto high myopia. The procedures were performed using aHansatome威 microkeratome (Bausch & Lomb Surgical) withan 8.5 mm ring and a 160 m plate. The ablation wasperformed with a Nidek excimer laser.Figure 10. (Rubinfeld) Slitlamp photograph of multiple focal areasof epithelial ingrowth extending to the pupil in Case 6.Figure 11. (Rubinfeld) Operating microscope photograph takenafter lifting the outer flap to remove epithelial ingrowth in Case 6. Theepithelial cells were not located at this interface. Folds (closed arrow)in a stromal sliver of recut tissue were discovered instead. The openarrow indicates the edge of the lamellar sliver of stromal tissue.J CATARACT REFRACT SURG—VOL 29, DECEMBER 20032311
LIFT OR RECUTFigure 12. (Rubinfeld) Operating microscope photograph of thin,irregular sliver of stromal tissue observed after recutting the flap forenhancement in Case 7. The surgeon was attempting to reposition thethin lamellar tissue.Figure 13. (Rubinfeld) Retroillumination slitlamp photograph of interface folds (arrows) visible in the transected flap in Case 7.Ten weeks after the enhancement procedure, the patientwas referred for consultation. He complained of glare, lightsensitivity, and poor quality of vision with spectacle correction. The UCVA was 20/50, and the BSCVA was 20/30 2with 1.25 0.50 5. On retroillumination, interfacefolds were visible in the transected flap (Figure 13); cornealtopography showed irregular astigmatism. The patient continued to have difficulty with night driving and was fit withan RGP contact lens that improved the BCVA to 20/20 and improved but did not eliminate the glare.revealed marked irregular central corneal astigmatism (Figure14). Twenty-four months post enhancement, the BSCVA inthe right eye remained 20/40 with a correction of 0.25 1.75 43 and the topography continued to demonstratea highly irregular central corneal surface.Refractive Surgeon SurveyCase 9Fifty refractive surgeons were surveyed about their enhancement techniques and experience. Twenty-eight surgeons responded, and these results are presented in Figures15 to 19. On average, the surgeons recut flaps 18% of thetime in 1998; this was reduced to 1% in 2002. The majorA 39-year-old white woman had uneventful bilateralLASIK for high hyperopia with a Technolas 116 laser(Bausch & Lomb Surgical). An Automated Corneal Shapermicrokeratome with a 160 m plate was used. Twenty-sixmonths postoperatively, the UCVA in the right eye hadregressed to 20/50 with residual hyperopic astigmatism.An enhancement procedure was performed in the righteye using a 160 m plate on a Hansatome microkeratomeand a 9.5 mm suction ring. After the microkeratome pass,the flap was lifted with a spatula and a thin piece of freetissue approxim
Joseph Frucht-Pery, MD, Anthony J. Kameen, MD, Gerald J. Negvesky, MD . and 1 eye was recut with a different microkeratome with the same