Transcription
AGA Institute Rapid Review and Recommendations on the Role of Pre-Procedure SARSCoV2 Testing and EndoscopyAuthors: Shahnaz Sultan*1, Shazia M. Siddique*2, Osama Altayar3, Angela M. Caliendo4, PericaDavitkov5, Joseph D. Feuerstein6, Dawn Francis7, John Inadomi8, Joseph K. Lim9, Yngve FalckYtter5, Reem A. Mustafa10 on behalf of the AGA*co-first authorsAffiliations:1. Division of Gastroenterology, Hepatology, and Nutrition, University of Minnesota, MinneapolisVA Healthcare System, Minneapolis, Minnesota2. Division of Gastroenterology, University of Pennsylvania Perelman School of Medicine,Philadelphia, Pennsylvania3. Division of Gastroenterology, Washington University School of Medicine, St. Louis, Missouri4. Department of Medicine, Warren Alpert Medical School of Brown University, Providence,Rhode Island.5. Division of Gastroenterology, Northeast Ohio Veterans Affairs Healthcare System, CaseWestern Reserve University School of Medicine, Cleveland, Ohio6. Division of Gastroenterology and Center for Inflammatory Bowel Diseases, Beth IsraelDeaconess Medical Center, Boston, Massachusetts7. Mayo Clinic College of Medicine, Division of Gastroenterology and Hepatology, Jacksonville,FL, USA.8. Department of Internal Medicine, University of Utah School of Medicine, Salt Lake City, Utah9. Yale Liver Center and Section of Digestive Diseases, Yale University School of Medicine,New Haven, Connecticut10. Division of Nephrology and Hypertension, Department of Internal Medicine, University ofKansas Medical Center, Kansas City, Kansas.Address for Correspondence:American Gastroenterological AssociationNational Office, 4930 Del Ray AvenueBethesda, Maryland 20814E-mail: ewilson@gastro.orgTelephone: (301) 941-2618Manuscript Word Count:References:Tables and Figures: 4 Tables and 5 FiguresSupplement: 5 Tables and 2 Figures1
Keywords: COVID-19, Diagnostic test, SARS-CoV2This document represents the official recommendations of the American GastroenterologicalAssociation (AGA) Institute and was developed by select members of the the Clinical GuidelineCommittee and Clinical Practice Update Committee and approved by members of the AGAGoverning Board.Expiration Date: 6 monthsIntroductionThe genome of the SARS-CoV2 virus, the cause of COVID-19, was first identified on January12, 2020. This was a critical first step that allowed for the development of molecular diagnostictests to identify the presence of virus.1-3 At the individual patient level, testing for SARS-CoV-2infection in symptomatic patients helps to identify individuals who can be isolated to prevent thespread of disease and can inform treatment decisions aimed at reducing morbidity andmortality.4 At the population level, widespread testing of individuals (symptomatic andasymptomatic) is critical to understanding the true prevalence of disease. This information canthen inform local decisions regarding the economy and the provision of healthcare services,including the re-introduction of endoscopy across healthcare systems and ambulatory carecenters.5Tests fall under two broad categories: tests that detect virus and tests that detect the presenceof antibodies associated with the virus (serology tests). Direct detection of viral RNA is mostcommonly performed via nucleic acid amplification testing (NAAT) of specific known targets inthe genome of the virus, using RT-PCR.6 The most common sample types (or sources) areswabs that are taken from the nasopharynx and/or oropharynx, lower respiratory tract, or salivaby a trained healthcare worker or self-collection. It is important to recognize that the quality ofsample collection, as well as the source, influence test results. Development of an antibodyresponse to SARS-CoV-2 infection through the identification of antibodies indicates recent orpast infection.The predictive value of a test refers to the probability of having a condition or disease in anindividual with a positive test result (positive predictive value) and the probability of not having acondition or disease in an individual with a negative test result (negative predictive value). Apre-testing strategy in asymptomatic individuals prior to endoscopy may be informative indistinguishing people with SARS-CoV2 infection and those without SARS-CoV2 infection but itis affected by the prevalence of the disease in asymptomatic individuals.This rapid review and rapid guideline address the role of implementing a SARS-CoV2 pretesting strategy prior to endoscopy. A prior AGA guideline examined the role of PPE (includingextended use and re-use of N95/N99 respirators or PAPRs in resource-constrained settings)when testing was not readily available; the aim of this guideline was to determine the role oftesting in endoscopy re-opening.7 To inform the recommendations, a systematic review of thediagnostic performance of currently available tests for SARS-CoV2 infection was conducted. A2
survey was conducted to provide information about the threshold of risk that endoscopists werewilling to accept during endoscopy and an overview of strategies to estimate prevalence ofinfection among asymptomatic individuals is provided. Finally, the panel draftedrecommendations for the role of a pre-testing strategy for low, intermediate, and highprevalence settings and a recommendation for serology testing (Table 1).Table 1: Executive Summary of Recommendations*What is the role of a pre-testing strategy in asymptomatic individuals 48-72 hoursprior to endoscopy (including a self-quarantine between testing and endoscopy)?Benefits: Triage and PPE use to reduce the risk of infectionDownsides: Patient burden, Limited testing capacity, Testing logistics and costRecommendation 1: For most endoscopy centers where the prevalence ofasymptomatic SARS-CoV2 infection is intermediate (0.5% to 2%), the AGAsuggests implementing a pre-testing strategy using information about prevalenceand test performance (sensitivity/specificity) in combination with considerationsabout the benefits and downsides of the strategy.Conditional recommendation, low certainty evidenceRemarks:-In settings where testing is feasible and there is less perceived burden on patients, andwhen the benefits outweigh the downsides (e.g. false positives do not significantlyoutnumber the true positives), an endoscopy center may reasonably choose toimplement a pre-testing strategy. Among individuals that test negative, endoscopists andstaff should use surgical masks** for all upper and lower endoscopies. Endoscopists andstaff who are unwilling to accept the potential small risk of infection (from falsenegatives) may use N95/N99** respirator or PAPRs for upper and/or lower endoscopies.-In settings where the logistics of testing are challenging, and the downsides outweighthe benefits (e.g. the false positives outnumber the true positives) and endoscopy unitsare unwilling to accept the potential (albeit small) risk of infection then an endoscopycenter may reasonably choose not to implement a pre-testing strategy and proceed withusing higher PPE (N95/N99** respirators or PAPRs) for all proceduresRecommendation 2: For endoscopy centers where the prevalence ofasymptomatic SARS-CoV2 infection is low ( 0.5%), the AGA suggests againstimplementing a pre-testing strategy.Conditional recommendation, very low certainty evidenceRemarks:- In low prevalence settings, a pre-testing strategy may not be informative for triage dueto the high number of false positives, thus PPE availability may drive decision-making.- If PPE is available, the majority of endoscopists and staff may reasonably select to useN95/N99** respirator or PAPRs. However, a small minority, with a low risk aversion3
threshold, may reasonably choose to use surgical masks** for all upper and lowerendoscopies.Recommendation 3: For a small number of endoscopy centers in high prevalenceareas, the AGA suggests against implementing a pre-testing strategy. In“hotspots”, endoscopy may be reserved for emergency or time-sensitiveprocedures with use of N95/N99** respirators or PAPRs for all procedures.Conditional recommendation, very low certainty evidenceRemarks:- In high prevalence areas, a pre-testing strategy may not be informative for decisionsabout PPE use due to the unacceptable number of false negatives, thus PPE availabilitymay drive decision-making- If N95/N99** respirators or PAPRs are available, these may be used for all upper andlower endoscopies- A “hotspot” is defined by a surge in COVID-19 cases with an acute burden on hospitalcapacity. In hotspots, resumption of outpatient endoscopy may depend on availability ofPPE.Recommendation 4: For all endoscopy centers, the AGA recommends againstserologic testing as part of a pre-testing strategy for patients or endoscopy staff.Strong recommendation, low certainty evidenceRemarks:- Serology testing for the presence of antibodies indicates past infection and has no rolein diagnosing SARS-CoV2 infection in asymptomatic individuals prior to endoscopy.- Evidence supporting the role of seroconversion for return to work or hospital staffingpolicies is also lacking.The strength of a recommendation is expressed as strong or conditional and has thefollowing interpretation:Strong recommendation: For clinicians: most individuals should follow the recommended course of action,and only a small proportion should notConditional recommendation: For clinicians: the majority of individuals in this situation would want thesuggested course of action but many would not; different choices will beappropriate* These recommendations assume that all patients are systematically screened for COVID-19 symptomsusing the CDC screening checklist and are required to wear masks while in the endoscopy unit.** Appropriate PPE includes a face shield over the surgical mask and face shield over the N95/N99respirator (to allow for re-use/extended use in limited PPE availability settings).74
Scope and PurposeWe seek to provide an overview of the considerations of diagnostic testing in the decision to reopen or expand endoscopy operations in the setting of a pandemic. We summarize theavailable data on the diagnostic test characteristics of tests for SARS-CoV2 infection andprovide evidence-based clinical guidance on the role of pre-testing prior to endoscopicprocedures. This rapid review and guideline was commissioned and approved by the AGAGoverning Board to provide timely, methodologically rigorous guidance on a topic of high clinicalimportance to the AGA members and the public.Panel Composition and Conflict of Interest ManagementThe guideline panel included gastroenterologists, an infectious disease expert, a member of thePractice Management and Economics Committee, and guideline methodologists from theClinical Guideline Committee, and Clinical Practice Updates Committee. Panel membersdisclosed all potential conflicts of interest according to the AGA Institute policy. All memberswere required to disclose financial, intellectual or other potential conflicts.Target AudienceThe target audience of these guidelines includes gastroenterologists, advanced practiceproviders, nurses, and other health care professionals in academic centers and in privatepractice settings across various geographic locations. Patients, as well as policy makers, mayalso benefit from these guidelines. These guidelines are not intended to impose a standard ofcare for individual institutions, healthcare systems or countries. They provide the basis forrational informed decisions for clinicians, patients and other health care professionals in thesetting of a pandemic.How to use these guidelinesThis rapid guideline is intended to help clinicians make decisions about pre-procedural testingprior to endoscopy however decisions may be constrained by local health system or state-levelpolicies as well as availability of resources, specifically RT-PCR tests and PPE.Recommendations are accompanied by qualifying remarks which serve to facilitate moreaccurate implementation. They should never be omitted when recommendations from theseguidelines are quoted or translated. A summary of the recommendations is provided in Table 1with a more detailed rationale for each recommendation in the discussion section. Theimplementation considerations section in this guideline will help clinicians implement theserecommendations. This section includes a checklist for endoscopy re-opening, instructions foran online interactive tool, and a matrix to facilitate pre-testing strategy considerations in low andhigh prevalence areas accounting for testing and PPE availabilityMethods5
The evidence base to support this recommendation included (1) a systematic review and metaanalysis of the diagnostic test performance (sensitivity and specificity) of currently availabletests in the U.S. (2) a survey of gastroenterologists to understand the acceptable threshold ofrisk and (3) available data on prevalence of infection among asymptomatic individuals.Recommendations were developed using the GRADE framework.81. Systematic review and meta-analysis of diagnostic test performanceInformation sources and literature searchWe conducted a systematic literature search to identify all published and unpublished studiesthat could be considered eligible for our review with no restrictions on languages. To capturerelevant published articles, we electronically searched OVID Medline and EmBase frominception to May 16, 2020 using the MeSH term developed for COVID-19. For additionalunpublished or pre-print studies, we searched medRxiv, LitCovid, Biorxiv and SSRN on May16,2020/May 17,2020. Supplement Figure 1 (PRISMA Flow Diagram).Study selection and data extractionTwo reviewers were assigned to each database (SMS and PD to SSRN, OA and JF to Medrxivand Biorxiv, SS and RM to LitCovid) and independently screened titles and abstracts, as well aseligible full-text studies. Disagreements were resolved by discussion to reach consensus.Studies were included if they reported data on diagnostic test accuracy (cohort studies, crosssectional studies and case-control studies). All studies compared an index test to a reference“gold standard” test. Reviewers extracted relevant information into a standardized dataextraction form (Supplement Table 1). Data extracted included study characteristics (authors,publication year, country, study design), index test and reference standard, and sensitivity andspecificity of the index test. Additionally, studies that reported on prevalence of SARS-CoV2infection were also identified and reviewed.Assessment of Risk of BiasRisk of bias for studies on diagnostic test accuracy was assessed utilizing the QualityAssessment of Diagnostic Accuracy Studies (QUADAS)-2 revised tool.9 This tool assesses therisk of bias in four domains: patient selection, index test, reference standard, and flow andtiming of study. Studies were categorized as having higher quality if: a) they had a crosssectional or cohort design, as opposed to case-control design, b) included a reference standardthat is not a laboratory-developed test (LDT), and c) if there were two reference standards or atleast 1 reference standard with a second test for discordant results.Data Synthesis and AnalysisWe used the bivariate normal model to pool sensitivity and specificity using the logittransformation.10 We performed sensitivity analyses by limiting the analysis to studies at low riskof bias based on the patient selection and reference test domains of the QUADAS-2 tool. Weused the package mada version 0.5.8 in R version 3.6.3 to conduct the analysis and producethe forest plots.11, 12Certainty of Evidence and Evidence to Recommendations6
The GRADE framework was used to assess overall certainty by evaluating the evidence foreach outcome on the following domains: risk of bias, imprecision, inconsistency, indirectness,and publication bias.13, 14 The GRADE interactive summary of findings table was generatedusing the GRADEpro Guideline Development Tool.15 In developing recommendations, the panelconsidered the certainty of evidence, the balance between the desirable and undesirable effects(i.e. the benefits and downsides of a pre-testing strategy) and additional domains wereacknowledged where applicable (e.g., feasibility, resource use, acceptability). For allrecommendations, the expert panelists reached consensus. As per GRADE methodology,recommendations are labeled as “strong” or “conditional”. See Supplement Tables 2 and 3.The words “we recommend” indicate strong recommendations and “we suggest” indicateconditional recommendations.2. Risk Aversion Threshold SurveyGuideline panels often conduct internal surveys amongst panel members to determine valuesand preferences of providers. In order to gain a better understanding of a broader population ofendoscopists, the panel developed a survey open to all AGA members. The goal was tounderstand the threshold of endoscopists to accept risks associated with pre-testing to informPPE use (surgical mask versus N95/N99 or PAPR). We developed a short online survey thatwas piloted and modified prior to dissemination. Prior data has shown that endoscopy centers inNorth America are adopting pre-testing strategies.16 The purpose of our survey was to furtherunderstand risk aversion thresholds, based on false negative results, that drive decision makingfor triage and PPE. A false negative result may provide false reassurance to an individual whohas SARS-CoV2 infection, could be shedding virus, and may transmit the infection to others.The survey presented a clinical scenario of an asymptomatic patient undergoing electiveendoscopy who tests negative for SARS-CoV2 72 hours prior to the endoscopy. Respondentswere given five options for acceptable levels of risk of transmission of SARS-CoV2. The firstoption was 1/1000, with a comment stating that selecting this option would indicate willingnessto open the endoscopy center using a surgical mask only. The last option was 1/40,000 with acomment stating that selecting that option would indicate willingness to open the endoscopycenter only once N95s are available, despite a negative test result. The range of options werebased off several assumptions: a) local prevalence of 1% (intermediate), b) baseline risk ofSARS-CoV2 transmission without PPE of 50%, c) reduction of risk of COVID-19 transmissionwith PPE to 20% with surgical mask and 5% with N95 respirators.We collected responses from US-based gastroenterologists utilizing the “AGA Community”platform. The “AGA Community” is a non-public community for members of the AmericanGastroenterological Association through which gastroenterologists connect with colleagues andhave conversations about relevant issues in their field.3. Prevalence of SARS-CoV2 in Asymptomatic IndividualsA pre-testing strategy in asymptomatic individuals prior to endoscopy can be informative indistinguishing people with SARS-CoV2 infection, and those without, but it is affected by the7
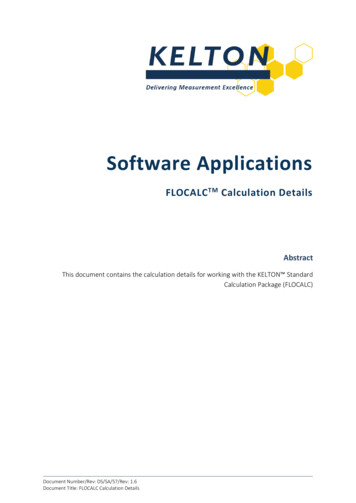
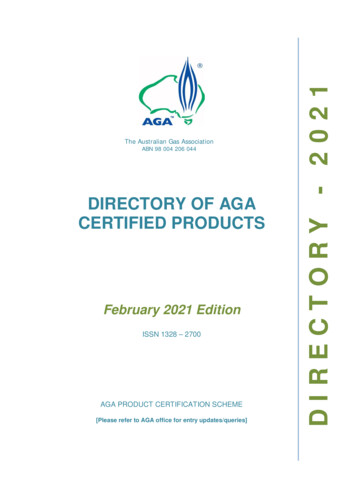
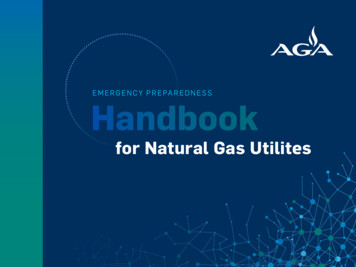
prevalence of the disease in asymptomatic individuals. To identify sources of data that provideinformation about the prevalence of infection in asymptomatic individuals we searched thepublished and unpublished literature and also reviewed public health websites. We also queriedpanel members regarding data from their local institutions.Results1. Systematic review and meta-analysis of diagnostic test performanceWe identified 12 studies that provided information for 31 comparisons about test accuracy forthe various NAAT tests.17-28 The risk of bias was rated using the QUADAS-2 (See SupplementTable 4). The pooled sensitivity was 0.941 (95% CI: 0.908 - 0.963) and pooled specificity was0.971 (95% CI: 0.958 - 0.980). We performed a sensitivity analysis for studies with low risk ofbias and found similar results: pooled sensitivity 0.929 (95% CI: 0.847 - 0.968) and pooledspecificity 0.968 (95% CI: 0.942 – 0.983). See Supplement Figure 2. An important caveat ofthese studies is that tests were validated in samples from symptomatic individuals and it is likelythat in asymptomatic individuals the tests may not perform as well and have lower sensitivityand specificity.Figure 1: Forest plot of test accuracy (pooled sensitivity and specificity)2. Risk Aversion Threshold Survey ResultsWe received 74 responses to the survey (Table 2). There was a wide distribution of answerselections: 37.8% (28/74) selected willingness to accept a risk of 1/40,000, indicating that theywould not be willing to open their endoscopy center unless N95s are available for all cases,including those with a negative SARS-CoV2 test. On the other hand, 19/74 (25.7%) selected1/1,000, indicating that they were willing to open their endoscopy units and use surgical masksregardless of testing. The remainder of the participants (27/74, 36.5%) were willing to acceptrisks between 1/2500 to 1/10,000. Survey respondents included gastroenterologists practicing inacademic institutions 23/74 (31.1%), in non-academic hospitals 15/74 (20.3%) in independent8
practice 34/74 (45.9%) and in other institutions 2/74 (2.8%). Gastroenterologists performingprocedures in private practice ambulatory centers were willing to accept higher infection riskcompared to gastroenterologists in academic centers and non-academic hospitals. Of 19participants choosing the 1 in 1,000 risk, 12 (63.2%) were in private practice.Table 2: Survey respondent characteristics by risk aversion thresholdCharacteristics by Response SelectionAllrespondents 1 in 1,000 1 in 2,500 1 in 5,000 1 in 10,000 1 in 40,000TotalSex (Male %)7419101072851 (68.9)12 (63.2)9 (90.0)10 (100.0)5 (71.4)15 (53.6)23 (31.1)4 (21.1)5 (50.0)1 (10.0)4 (57.1)9 (32.1)34 (45.9)12 (63.2)3 (30.0)4 (40.0)3 (42.9)12 (42.9)15 (20.3)2 (10.5)1 (10.0)5 (50.0)0 (0.0)7 (25.0)1 (1.4)0 (0.0)1 (10.0)0 (0.0)0 (0.0)0 (0.0)1 (1.4)1 (5.3)0 (0.0)0 (0.0)0 (0.0)0 (0.0)8.0[5.5, 37.0]8.0[4.0, 14.5]800[325, 950]450[325, 500]500[300,1000]31 [30,33.5]20[9, 25]17.5[11.3,27.5]Settings (%)Academic Medical CenterIndependent PracticeNon-Academic HospitalOtherVeterans’ AdministrationHospitalGroup size (median [IQR])7.0[4.0, 20.0]9.08.54.0[5.0, 24.0] [4.5, 18.8] [4.0, 8.3]Clinical ExperienceProcedures per year(median [IQR])Years of practice (median[IQR])500[300, 1000]20[12, 30]493[213,1075]400[263,1000]22.517.5[15.5, 30] [6.5, 25.5]3. Prevalence of SARS-CoV2 in Asymptomatic IndividualsFor diagnostic tests to inform decision-making, it is essential to determine the pre-testprobability (e.g. prevalence) of disease in asymptomatic individuals. We searched for studiesthat evaluated the prevalence of SARS-CoV2 among asymptomatic individuals but onlyidentified studies reporting on seroprevalence which were noninformative. Public websitesreporting on numbers of positive cases (predominantly in symptomatic patients) and deaths9
were reviewed but due to limitations of non-random testing, variability in availability of testing,and delays in reporting, these estimates cannot directly inform prevalence estimates inasymptomatic individuals. Acknowledging the limited publicly available evidence for accurateestimates of prevalence of SARS-CoV2 infection in asymptomatic individuals, we relied oninformation from panel members’ experiences within their health systems (based on rates ofpositive cases in asymptomatic individuals undergoing testing prior to any elective procedure)and modeling studies trying to estimate prevalence of SARS-CoV2 infection in the generalpopulation.We defined low prevalence areas as areas where the prevalence of asymptomatic infection islower than 0.5%, intermediate prevalence areas as areas where the prevalence is between0.5 and 2%, and high prevalence is greater than 2%. We defined hotspots as areas wherethere is a sudden surge in the number of daily cases with an acute burden on hospital capacity.The prevalence of exclusively asymptomatic infections is believed to be significantly lower thanthe commonly reported county or state estimates of positive cases and estimated to beapproximately 1/10th of the rates of positive cases. This is supported by a modelling study ofstate-level data which estimated that for each diagnosed symptomatic patient there may be 10asymptomatic or undiagnosed individuals in that population.29 Furthermore, based on a studyconducted between April 13 and May 15, 2020 in Miami, the prevalence in an asymptomaticpre-endoscopy population was 0.25% compared to prevalence ranges from 5.4-12.7% inneighboring regions.30 Similarly, another study at Stanford University found 2/999 total positives(0.2% prevalence).31 Members of our panel provided some information regarding local data forpositive test results in their health systems. At UW Medical Center and Harborview MedicalCenter: from March 27 - June 28, 2020 there were two (2) asymptomatic (no fever, cough orSOB) out of 1437 patients who tested positive. Prevalence in asymptomatic patients 0.14%.(B. Teng personal communication).DiscussionThe guideline panel acknowledges that local, state, and health system policies may dictaterequirements for pre-procedural testing of asymptomatic patients as well as dictate decisionsabout PPE use. The following recommendations are based on the assumption thatgastroenterologists have decision-making power over implementing a pre-testing strategy.Outcomes for decision-making: (i) triage and (ii) PPE use. A pre-testing strategy can informendoscopy operations by helping with decisions regarding triage and PPE use. Using anestimate for the prevalence of asymptomatic SARS-CoV2 infection and test performance(sensitivity and specificity) one can calculate the number of true positives (TP), true negatives(TN), false positives (FP), and false negatives (FN). All patients who test positive for SARSCoV2 infection will have their elective procedure canceled and advised to self-quarantine for 14days. A positive test result, however, includes asymptomatic individuals with SARS-CoV2infection (TP) as well as individuals who test positive but do not have infection (FP). All patientswho test negative for SARS-CoV2 infection can proceed with endoscopy and a surgical maskmay be used by endoscopists and staff for upper and lower endoscopies. A negative test result,10
however, includes individuals who do not have infection (TN) and those individuals who haveSARS-CoV2 infection but test negative (FN).The two main concerns with a pre-testing strategy are the false positives (i.e. individuals whotest positive for SARS-CoV2 but do not have the infection) and false negatives (i.e. individualswho test negative for SARS-CoV2 but do have the infection). In a patient who tests negative forSARS-CoV2 infection (false negative) and a surgical mask is used for upper endoscopy, theremay be a potential (albeit small) increased risk of infection to the endoscopy staff and falsereassurance to the individual. In a patient who tests positive for SARS-CoV2 who does not haveinfection (false positive), implications for the patient include cancellation of the procedure, selfquarantine for 14 days, apprehension, and loss of work. Below we summarize the evidence,weigh the benefits and downsides and provide the rationale for each recommendation.Recommendation 1: For most endoscopy centers where the prevalence of asymptomaticSARS-CoV2 infection is intermediate and ranges from 0.5% to 2%, the AGA suggestsimplementing a pre-testing strategy using information about prevalence and testperformance (sensitivity/specificity) in combination with considerations about thebenefits and downsides of the strategy.Conditional recommendation, low certainty evidenceRemarks:-In settings where testing is feasible and there is less perceived burden on patients, and whenthe benefits outweigh the downsides (e.g. false positives do not significantly outnumber the truepositives), an endoscopy center may reasonably choose to implement a pre-testing strategy.Among individuals that test negative, endoscopists and staff should use surgical masks** for allupper and lower endoscopies. Endoscopists and staff who are unwilling to accept the potentialsmall risk of infection (from false negatives) may use N95/N99** respirator or PAPRs for upperand/or lower endoscopies.-In settings where the logistics of testing are challenging, and the downsides outweigh thebenefits (e.g. the false positives outnumber the true positives) and endoscopy units are unwillingto accept the potential (albeit small) risk of infection then an endoscopy center may reasonablychoose not to implement a pre-testing strategy and proceed with using higher PPE (N95/N99**respirators or PAPRs) for all proceduresSummary of the EvidenceWe did not identify any comparative studies that directly assessed a strategy of pre-proceduraltesting versus no testing in asymptomatic individuals prior to endoscopy. The overall body ofevidence was limited by small numbers, poorly defined and inconsistent reference standards,and test accuracy from case-controlled studies (which can lead to inflated estimates of testaccuracy). Additionally, there was missing data in the studies regarding timing of specimencollection in relationship to onset of clinical symptoms and specimen type used for testing.Given all of these concerns, the overall certainty was low.11
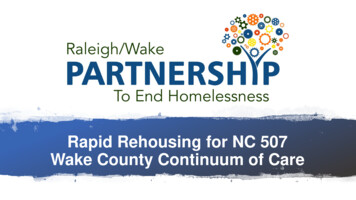
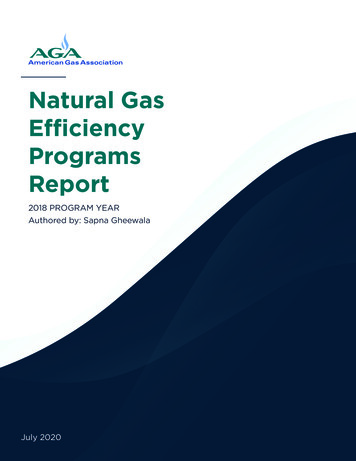
Also, there were no test accuracy studies that evaluated the performance of RT-PCR tests inasymptomatic individuals. Based on evidence demonstrating similar viral shedding in presymptomatic individuals as compared with symptomatic individuals, we applied the testaccuracy for symptomatic patients, however, we assumed that the lower boundary of the 95%confidence interval more accurately reflected test performance in the asymptomatic population.We display the summary of findings table for an intermediate prevalence setting (0.5% to 2%) inTable 2.Figure 2: GRADE Summary of Findings Table of Test Accuracy Results for Prevalence of0.5%, 1%, 2% of SARS-Co2 Infection in Asymptomatic IndividualsBenefits and DownsidesThe benefits and downsides (or pros an
Governing Board. Expiration Date: 6 months Introduction The genome of the SARS-CoV2 virus, the cause of COVID-19, was first identified on January 12, 2020. This was a critical first step that allowed for the development of molecular diagnostic tests to identify the presence of virus.1-3 At the individual patient level, testing for SARS-CoV-2