Transcription
Extracorporeal Membranous Oxygenation (ECMO)Bedside Reference ManualUniversity of California San DiegoCalling a CODE ECMO 2UCSD specific orders/documentation/chain of command 3Indications .4Contraindications .5ECMO Basics and Components 6ECMO Circuit .7Console/pump Options at UCSD . .8Cannulas 9Oxygenator and Blender .12Other ECMO Components .13ECMO Values .16Initiation/General mgmt .17VV Specific Mgmt .20VA Specific Mgmt .23Trouble Shooting .26Emergencies 30Version 1: 6/20191
Calling a CODE ECMO (2 steps)First: Patient’s ICU attending pages on call-ECMO MDs (CTSurgery and Interventional Cardiology) for discussion of thecase and decision on ECMO initiation In webpaging search “ECMO,” and select the correctlink and fill in the paging information needed Figure 1. Screenshot of the UCSD webpaging search pageSecond: If ECMO initiation is decided on, the on call ECMOMD calls a formal “CODE ECMO” by calling x6111 Will need to indicate the name of the attendingapproving ECMO as well as the type of ECMObeing initiated (cardiac anesthesia comes to VVinitiations for TEE) The formal “CODE ECMO” initiates theadditional support needed including anesthesia,perfusionist, etc2
UCSD Specific PoliciesPlacing ECMO Orders (2 order sets need to be completed)1. “ECMO Cannulation” order set Includes patient care orders, IV fluids andanticoagulation bolus2. “ECMO Maintenance” order set Includes auto-consult to palliative care,CPR/defibrillation parameters, vascularchecks, labs and maintenance medicationsincluding anticoagulation Figure 2. Screenshot of the EPIC order sets for ECMOECMO DocumentationAll ECMO documentation can be found in nursing flowsheetentitled “ECMO”Nursing Chain of Command for ECMO Related IssuesEmergencyFor any ECMO specific emergency (i.e. pump failure, arterialair bubble, no flow) RN to “Activate Crisis Action Plan” bypaging on call perfusionist and consulted ECMO attending(PCCM or ACCM)NON-emergencyRN to page on-call perfusionist who will help determineurgency of issue and appropriate next contact (primary team,ECMO MD, covering attending)3
IndicationsVA ECMO Moderately to severely reduced cardiac functionwith/without concurrent respiratory failure. Specificindications include but are not limited to: Post-MI Myocarditis Bridge to definitive therapy such as LVADor transplant Refractory ventricular arrhythmias(including consideration during cardiacarrest) Massive pulmonary embolism OB indications: Post-partumcardiomyopathy, amniotic fluid embolismVV ECMO Hypoxemic respiratory failure: ECMO should beconsidered in hypoxemic respiratory failure with a 50%mortality risk (which translates to P/F 150 on FiO2 90%) and even more so with a P/F 100 despiteoptimal care for more than 6 hours) Hypercarbic respiratory failure: refractory CO2 retentionon mechanical ventilation despite high ( 30 cm H2O)plateau pressures (e.g. status asthmaticus) To avoid mechanical ventilation in a patient awaitinglung transplant (may allow increased mobility, avoidsedation) Sudden respiratory collapse despite optimal care4
ECMO should be considered and discussed with theECMO team when: New diagnosis of Pulmonary Arterial Hypertension(with PAH team involvement) Pregnant with Pulmonary Hypertension Post partum cardiomyopathy Pre-heart or lung transplant Post heart transplant patient with vasculopathy Post lung transplant with Fi02 50% ARDS with FiO2 on ventilator 80% or consideringproningIf ECMO is indicated, the earlier they go on, the betterthey do. If you are considering ECMO (non-urgently) forone of the above conditions, email ecmo@ucsd.edu orcontact the ECMO MD on call.ContraindicationsRelative Contraindications: Advanced Age Trauma Septic Shock Advanced dementia/brain damage/severe prior stroke ESRD on dialysis Bleeding diathesis Recent or expanding CNS hemorrhage Terminal malignancy Decompensated cirrhosis Vasculature technically inaccessible Mechanical ventilation 7 days Aortic insufficiency or aortic dissectionAbsolute contraindications:5
Open chest Massive hemorrhage ( 1 PRBC per hour)ECMO BasicsTwo main modalities of ECMO: Venoarterial (VA) provides both hemodynamic andrespiratory support in the setting of cardiac failurewith/without concurrent respiratory failure. Blood istaken from the venous circulation and returned to thearterial circulation. Note, E-CPR is the use of VA-ECMO inrefractory cardiac arrest (although used at UCSD, it is notcurrently standard protocol) Venovenous (VV) provides isolated respiratory support inthe setting of lung failure. Blood is taken from andreturned to the venous circulationDepending on the ECMO cannulation, goals include thefollowing:1. Blood Oxygenation2. C02 removal3. Protective Lung ventilation4. Cardiac supportECMO Circuit Components Overview: Inflow cannula (venous): Deoxygenated blood Blood pump (capable of up to 5L.min flow) Oxygenator with inline gas blender/sweep Outflow canula (venous or arterial): oxygenated bloodAdditional Components May Include: Saturation Sensor- for H&H SvO2 Flow probe- sits on arterial tubing and measures flow, anddetects air bubbles Pre- and post-oxygenator pressure monitor6
Console for adjustmentsPorts for accessHeat Exchanger and heater/cooler7
The ECMO CircuitFigure 3. Circuit in Graphic Form. Cyi 20198
ECMO Console/Controller/Pump Options at UCSDMaquet Cardiohelp – Preferred. Can be managed byRNsFigure 4 Maquet Cardiohelp System. Adapted from the Maquet Cardiohelp brochureMaquet Rotaflow – alternative option, can only bemanaged by a perfusionistFigure 5. Maquet Rotaflow ECMO system. Adapted from Getinge rotoflow brochure.Blood Pump: Centrifugal Note with the cardiohelp system, the disposable component(HLS module) contains the blood pump as well as theoxygenator and heat exchanger The pump speed is set by the provider between 0 – 4000RPM’s (which can drive up to 5 L/min of blood flowdepending on the circuit)9
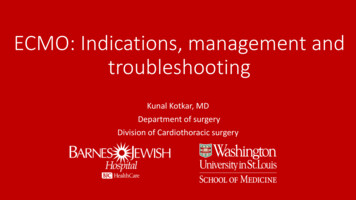
The ECMO CircuitCannulas: Increased resistance to blood flow with smaller diameter,longer cannulas (by way of Poiseuille’s Law, R 8 L/ r4) A cannula with increased resistance causes a greaterpressure drop; goal pressure drop across venous cannulais 40 mm Hg and across an arterial cannula is 100 mmHgFigure 6. Flow Rate and Pressure Drop based on Cannula Diameter. Increasing cannulasize yields a larger flow rate with a small pressure drop. Red signifies an arterialcannula (length of 23 cm); blue signifies a venous cannula (length of 55 cm). Adaptedfrom the Maquet Cardiohelp System brochure10
VA ECMO Cannulas: Arterial cannula: 15 – 25 Fr, Venous cannula 19 – 25 Fr Peripheral or Central cannulation Peripheral cannulation usually percutaneous Open cannulation- peripheral cannulation cut down viathe femoral or internal jugular vein for the venousdrainage and the femoral or axillary artery for arterialoutflow Central cannulation- median sternotomy or thoracotomy.The venous access is generally from the right atrium andthe arterial access via the ascending aortaVV ECMO Cannulas: Drainage cannula 22 – 30 Fr, Return cannula is slightlysmaller at 15 – 23 Fr Generally placed via peripheral cannulation via Seldingertechnique with inflow: outflow options as follows: Femoral (IVC):Internal Jugular (RA) or subclavian Femoral (IVC):Femoral (RA) Single dual lumen cannula in the internal jugular orsubclavian vein (most common option used atUCSD). See following section for more detailsVAV cannulation: Sometimes utilized as well Return cannulas to both venous and arterial side Option for patients who start on VV and thenrequire VA as heart fails; also option for PHpatientsFigure 7. Medtronic venous and arterial cannulas. Note the arterial cannula’s haveside port. Adapted from Getinge website11
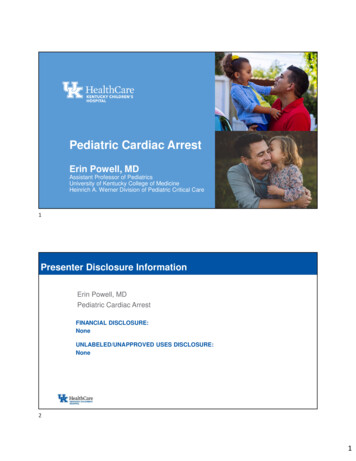
Single Dual Lumen Cannulas: Drainage access point resting in the IVC and SVC and thereturn port in the right atrium directed at the tricuspidvalve (most common option used at UCSD). Single lumenoptions are generally between 13 – 31 Fr and include thefollowing: Avalon ELITE bi-caval dual lumen catheter MC3 Crescent jugular dual lumen catheter Placed with TEE guidance to confirm placement Dressing markings on skin to ensure migration has notoccurred Advantages include maximizing flow rate while minimizingthe risk of recirculationFigure 8. Graphic Representation of the Avalon ELITE Bi-caval Dual Lumen Catheter.On the left, cannula shown entering the R internal jugular vein and terminating in theIVC. On the right, close up showing drainage ports in the SVC and IVC with return portresting in the RA with the jet aiming at the tricuspid valve. Adapted from Lezar et al, JPed Surgery, 201212
Oxygenator and Blender: Composed of a heparin-coated polymethylpenenehollow fiber membrane. Removes carbon dioxide, oxygenates blood In line with the Gas Blender and SweepFigure 9. Blender set-up. C. Yi. 2019 Oxygenation is affected by gas blender (i.e. FdO2) andECMO blood flow Ventilation is affected by sweep (usually started at 1:1to blood flow) but is independent of blood flow Both are affected by diffusion gradients and surfacearea based on Fick’s Law of Diffusion (Vgas α (A/T) * D* (P1 – P2))Figure 10. Fick’s Law of Diffusion. Adapted from Respiratory Physiology, 10e.John West 2015.13
Additional ECMO Components:SvO2 Probe: Connected on venous side, just proximal to theoxygenator Measures (very reliably) SvO2 and H&H May not work if patient has high lipids, or a PaO2 45mm Hg SvO2 (and lactate) are surrogate markers of O2delivery (DO2) and O2 consumption (VO2)Pressure Sensor: Measures venous, arterial and inlet pressures (seenext section)Figure 11. Arterial side of Cardiohelp HLS oxygenator. C. Yi. 201914
Flow probe: Connected on the arterial side, just distal to theoxygenator Measures blood flow in L/min, and detects air If air is detected, machine intervention is set toautomatically alarm, and to reduce RPMs to zero. Willinitiate high priority alarm for no flow, and air bubbledetectionFigure 12. Flow probe attached to arterial tubing. C. Yi. 2019Heat Exchanger: Connects to oxygenator and circulates warm water fortemperature regulation Actively warms to 37 ºC Can also passively cool (by blood being outside of thebody and exposed to room air) but cannot activelycool, so if therapeutic hypothermia is desired, theArctic sun or thermoguard should be considered.Figure 13. Cincinnati SubZero Heater. C. Yi. 2019, and Fig 14. Cardioquip Heater.Cardioquip.com15
The Cardiohelp ConsoleHome Screen:Figure 14. Cardiohelp Home Screen C. Yi. 2019Lab Screen:Figure 15. Cardiohelp lab Screen C. Yi. 201916
ECMO ValuesVariableDefinition“Normal” ValueSpeedRotation per minuteof pump0-4000. Usuallyaround 3500Titrated by RN/Perfusionist to maintainordered flowVFlow in liters perminute2-5L/minOrdered by ProviderPVENPressure the pumpgenerates to pullvenous blood -150mmHgMore negative venous pressure Assess for kink, clot, or volumePARTPressure pump mustgenerate to returnblood 300mmHgIncreased arterial pressure Assess forkink, clot, or high blood pressurePINTPressure pump mustgenerate to pushthrough oxygenator 300mmHgNot clinically significant: used tocalculate DeltaPDelta P: Pressure dropacross oxygenator.Tells us if oxygenatoris compromised dueto clotsUsually around20 mmHgAbnormal if 40 or if doubles frombaseline.TARTReturn blood temp370 CHeater set by nursing/perfusion perprovider orderSV02Dependent on CO,oxygen consumption,H&H, and FdO2.65-75%Measured on venous tubing just afteroxygenator.PIf high, considerrecirculation.(VV maybeslightly lowerdue to lack ofoxygen and lowarterialsaturation)Hb 7g/dLMeasured on venous tubing just afteroxygenator.Hct 25%Measured on venous tubing just afteroxygenator.17
ECMO InitiationInitiation: After sedation and/or neuromuscular blockade,cannulation can begin Heparin bolus (20-100 U/kg) is given via IV formulationafter the wire is in place; goal ACT 150 seconds Set temperature on heat sensor (normothermia) andinitiate ECMO as follows: Set sweep gas flow rate (usually starts as 1:1 ratiowith goal blood flow) Set FdO2 to 100% ECMO flow rate is increased to 2000 RPMs followedby removal of the cannula clamps ECMO flow rate is increased over the next 5-10minutes to achieve goal blood flow (BSAxflow index;flow index generally 1.8 L/min/m2) Once goal flow is achieved, ventilator can generallybe set to lung protective settings Address sedation, neuromuscular blockade needs(see subsequent section) Address anticoagulation needs (see subsequentsection)Sedation/Analgesia: Pharmacokinetics and pharmacodynamics ofmedications is affected, via changes in volume ofdistribution (VD) and clearance Expect considerably higher doses of all sedation andpain medications (especially propofol and fentanyl) Prolonged use of propofol (at higher doses) canincrease lipids and cause failure of the SvO2 sensor18
General ECMO ManagementGuidelines outlined by ELSO Crisis action plan: all patients on ECMO shouldhave a Crisis Action Plan and EmergencyVentilator settings posted in the room If ECMO flow stops, patient lines should beclamped to prevent back flow (arterial isclammed first; venous is unclamped first) Orders written for goal blood flow, then RPMsare titrated Orders written for goal Co2. Then Sweeptitrated: Starts at 1:1 to ECMO blood flow. Cannula sites: cautious with all positioning dueto risk of migration/dislodgement Dressings are occlusive and changed q7days and PRN Limb ischemia can develop; pulse checksare necessary Monitor for hemolysis with usual hemolysis labs(LDH, haptoglobin, fibrinogen, coags) If high levels of hemolysis are seen, flowrate should be reduced19
General ECMO ManagementAnticoagulation: Following the heparin bolus during cannulation, aheparin gtt is initiated based on ECMO specificheparin protocol (included in ECMO order set) unlesscontraindicated ACTs followed initially, then aPTTs q6 hoursafter heparin adjustment (goal generally 4060sec) ATIIIs daily after 3 daysLab Goals:Lab TestNormal ValuesTargeted valueson ,000/mL 50,000/mLFibrinogen150-400mg/dL 180mg/dLHgb/Hct35-45% 25%ACT70-120s180-200sATIII75-120% 40%ECHO contrast: can cause micro bubbles in circuit whichtrigger the pump to alarm, and reduce RPM to zero Should be avoided when possible When necessary, advise ECMO specialist totemporarily turn off arterial air bubbleintervention20
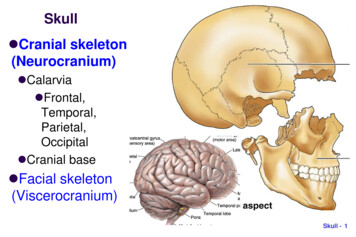
VV ECMO ManagementPre-ECMO mortality calculated using the RESP Score(respscore.com) Validated tool to predict survival for a patientreceiving ECMO for respiratory failure Variables include age, duration of mechanicalventilation, etiology of respiratory failure, NMBuse, NO use, HCO3- infusion, PaCO2 and PIP Scored between -22 and 15 to yield 5mortality classes (I-V with class I having thehighest chance of survival and V having thelowest) A RESP score of 0 (class III) 40-60% chance ofsurvival Can be calculated at RESPSCORE.COMFigure 16. RESP Score versus Survival. Based on a cohort study of 2355 patients.Dotted black lines and curved black lines signify the 95% and 99% confidence intervals,resp. Adapted from Schmidt et al, AJRCCM, 201421
VV ECMO Management 60-70% of cardiac output (CO) can be re-routed throughthe oxygenator Blood flow should be 2/3 of CO If unable to oxygenate, consider lowering CO withbeta blockers (e.g. esmolol) or other CO depressants CO formula: CO LPM x (SaO2(ECMO circuit) SvO2(patient)) / (SaO2(patient) – SvO2(patient)) Oxygenation is dependent on the FdO2 as well as thepercentage of the cardiac output going through theoxygenator, Hb concentration and the oxygenation of thevenous blood not passing through the oxygenator(including coronary sinus blood) Chest compressions are OKAY Blood gases: ABGs are accurate and can be drawn anywhere VBGs are only accurate when drawn from venousside of ECMO machine Fick CO is not accurate (as MvO2 is not accurate) ECHO EF and CO measurement generally accurateVentilator Management Ideally managed at low setting in effort to “rest” lungs Low RR ( 10 BPM), moderate PEEP (5-15 cm H2O ), VT 6cc/kg, FiO2 50%, PIP 30cm H2O; can utilize longinspiratory time ECMO FdO2 titrated to oxygenation with the followinggoals: SaO2 100%; SvO2 60-75%; PaO2 40-50 mm Hg;SpO2 85-100% Ventilation: pCO2 35-45 mm Hg; pH 7.35-7.4522
Weaning VV Consider weaning on VV ECMO following improvementin the underlying respiratory failure as evidence by thefollowing: Increasing PaO2 or decreasing PaCO2 withoutchanges on the ventilator or ECMO settings Improving compliance Radiographic Improvement Done in conjunction with CT Surgery ECMO blood flow remains the sameIf primary ECMO indication is for Oxygenation: FiO2 incrementally titrated down to 21%, thensweep turned to 0L/min Monitor hemodynamics and venous saturation.After an hour, draw ABG. If SaO2 95% and PaCO2 50 mm Hg, consider decannulationIf primary ECMO indication is for Hypercarbia: Sweep and FiO2 incrementally titrated down tosweep of 0L/min Monitor hemodynamics and venous saturation.After an hour, draw ABG. If SaO2 95% and PaCO2 50 mm Hg, consider decannulation Ventilator settings will be adjusted to account for lessECMO support Ensure that the ventilator settings allow room forincreasing support once decannulated During decannulation perfusionist must be present23
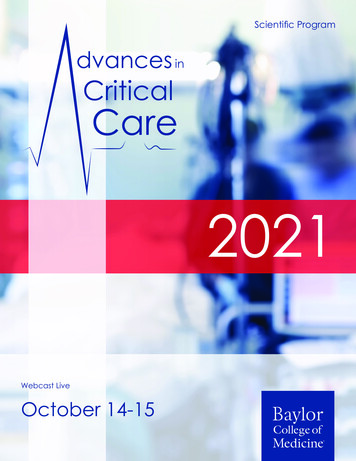
VA ECMO Management Pre-ECMO mortality calculated using the SAVE Score(save-score.com) Validated tool to predict survival for a patientreceiving ECMO for cardiogenic shock Variables include age, weight, duration ofmechanical ventilation, PIP, etiology of cardiogenicshock, pre-ECMO objective data including HCO3-,pulse pressure and diastolic pressure Scored between -35 and 17 to yield risk classes I-V(I with the highest rate of survival (75%) and V withthe lowest (18%)) SAVE score of 0 (class III) 40% chance ofsurvival Can be calculated at SAVE-SCORE.COMFigure 17. SAVE Score versus Survival. Based on a cohort study of 3846 patients.Curved blue lines and curved black lines signify the 95% and 99% confidence intervals,resp. Adapted from Schmidt et al, Euro Heart Journal, 201524
General Considerations: VA NO chest compressions while ECMO is running CO measurements (including FICK) are not accurate asECMO contributes to CO EF on ECHO only accurate if ECMO flow is reduced to 11.5 L CVP not accurate as inflow cannula empties into RA(falsely elevated) ECMO can increase afterload, leading to LV distensionwhich may be offloaded by IABP or Impella Blood gases: ABGs should be drawn from right radial/brachialarterial line if femoral arterial access and from afemoral arterial line if axillary arterialcannulation. VBGs can be drawn from anywhereConvergence: VA With myocardial recovery the point of convergence ispushed more distal along the aorta (meaning native CObegins taking over cerebral and coronary perfusion) Upper body hypoxemia: North-South Syndrome;Harlequin Syndrome Correction of such phenomenon can be achievedby increased ECMO flow rates to overcomenative CO or increasing the oxygen content ofpulmonary venous bloodFigure 18. Convergence variation for VA ECMO with femoral artery cannulation .Adapted from Rao et al, Circ Heart Failure, 201825
Ventilator Management: VA Ideally managed at low setting as outlined in priorsection for VV ECMO although with VA ECMO theECMO FiO2 is kept between 70-100% to keep SpO2 95% Other settings outlined in prior section: Low RR ( 10 BPM), moderate PEEP (5-15 cm H2O ), VT 6cc/kg, FiO2 50%, PIP 30cm H2O; can utilize longinspiratory timeWeaning: VA Consider weaning if improvement of the underlyingcardiac function is seen as evidenced by: Improved ScvO2 (with no change in VO2) Improved cardiac function on TTE Improved hemodynamics via PAC Done in conjunction with CT surgery ECMO blood flow is slowly decreased by 0.5 L/min at atime Flow should not go below 2 L/min due toincrease risk of VTE Blender FiO2 and sweep stay the same Ventilator settings will be adjusted to account for lessECMO support Ensure that the ventilator settings allow roomfor increasing support once decannulated During decannulation perfusion must be present*If you are weaning a VA patient who is on ECMO forrespiratory support, involve perfusion and CT surgery26
ECMO TroubleshootingECMO Specific Complications: Recirculation Caused by cannula migration or occlusion Signs include color change on venous line,increased SvO2, low SpO2 Bleeding/Hemorrhage Common locations include surgical incision site,cannula site, prior invasive procedural site, intrathoracic intra-abdominal, intra-cranial orretroperitoneal bleeding Coagulopathy, Hemolysis, Heparin-InducedThrombocytopenia Thrombosis Includes DVT and CVA Limb Ischemia (when using femoral oraxillary/subclavian cannula strategy) A separate antegrade cannula for leg perfusion isoften added Complications from the mechanical circuit are rare butinclude thromboembolism, membrane oxygenatorfailure, air entrainment, tubing rupture, accidentaldecannulation27
ECMO TroubleshootingMore negative P ven with Tube Chattering (subsequent dropin blood flow):(Note, when chattering is seen, the flow should be decreasedfirst) Hypovolemia/Bleeding can lead to hemolysis leading toa rise in plasma free Hb and LDH; can see chattering in thecircuit. Note, hemolysis and chattering can also be seenwith positioning as well as high pump speeds ( 3000RPM) Treat with fluid (crystalloid/colloid), blood product,assess/address bleeding source Increased intrathoracic pressure including mechanicalobstruction such as tamponade, PTX Treat with reduction in mean airway pressure (i.e.reduce PEEP) Bedside echo to rule out tamponade Note, tube thoracostomy for PTX can becomplicated by significant bleeding diatheses Increased intra-abdominal pressure: abdominalcompartment syndrome Treatment to address intra-abdominalhypertension and may include paracentesis,decompressive laparotomy Ensure venous cannula in correct positionMore negative P ven without Tube Chattering (subsequentdrop in blood flow): Venous cannula or tubing issue such as kink,thrombus or small cannula size Treatment includes correcting any kinks,increasing anticoagulation/switchingpharmacologic agent, consider adding asecond drainage cannula28
Increase in Part, and no change in P Arterial cannula problem such as kink, thrombus,small cannula or high SVR and MAP Treat as above by fixing kink,increasing/changing anticoagulation orupsizing the cannulaNo change in Part, and increase P Gas exchange device failureLow O2 saturation: Check that oxygen source is connected, on, and notkinked Ensure the blood flow has not decreased Assess for re-circulation Assess patient for increased oxygen consumption On VV ECMO ensure that the CO is not too high Consider why and fix the problem (e.g. fever;sepsis) or reduce CO with beta blocker, orsedation, etc.Elevated CO2 despite sweep titration: Water vapor can condense in the oxygenator, resultingin poor clearance. Clear by intermittently increasingsweep to 10L for a few seconds Blender failure – swap blender to switch to O2 tank at a1:1 sweep to blood flow ratio29
Lack of Pulsatility (VA-ECMO): If pulsitility is variable, ensure adequate ventilatorsupport to mitigate native cardiac output shunt. Lack of arterial pulsatility can be a representation ofpoor contractility of the heart and the heart’s inabilityto overcome the increase in afterload provided by theECMO. Need to assess for LV distention, consider LVvent Without pulsatility, blood can become stagnantand lead to thrombus formation In addition, ongoing venous drainage from thesbianand bronchial veins into the LA can lead to increasedLVEDV and hence LVEDP which can decrease coronaryperfusion (diastolic pressure – LVEDP) In the setting of severe AI or MR, this can lead tosignificant LA hypertension and cardiogenicpulmonary edema and hemorrhage Management includes modalities such as IABP,Impella, Atrial septostomy, direct LVdecompression (venting)Flow Arrest: Unintentionally Clamps left in place (immediately afterECMO initiation) Pump Failure (Very rare! The only time hand crank isused) Significant Thrombus formation Air entrained Cannula migration or vessel dissection30
ECMO Emergencies (very RARE):Figure 19. Cardiohelp hand crank used for pump failure. Note: as you turn the crank,lights on the top will indicate RPM (NOT LPM). C. Yi. 201931
References Del Sorbo, Lorenzo, Marcelo Cypel, and Eddy Fan. Extracorporeal life support foradults with severe acute respiratory failure. The Lancet Respiratory Medicine. 2014;2.2: 154-164. Zapol et al. Extracorporeal membrane oxygenation in severe acute respiratory failure.A randomized prospective study. JAMA. 1979;242(20):2193–6. Gattinoni L et al. Low frequency positive pressure ventilation with extracorporeal CO 2removal in severe acute respiratory failure. JAMA. 1986; 267(7):881-86. Peek et al. Efficacy and economic assessment of conventional ventilatory supportversus extracorporeal membrane oxygenation for severe adult respiratory failure(CESAR): a multicentre randomised controlled trial. Lancet. 2009;374(9698):1351–63. Combes et al. Extracorporeal membrane oxygenation for severe acute respiratorydistress syndrome. NEJM. 2018;378:1965-1975. Schmidt M et al. The PRESERVE mortality risk score and analysis of long-termoutcomes after extracorporeal membrane oxygenation for severe acute respiratorydistress syndrome. Intensive Care Medicine. 2-013; 39:1704-1713. Zheu et al. Early extracorporeal membrane oxygenator-assisted primary percutaneouscoronary intervention improved 30-day clinical outcomes in patients with ST-segmentelevation myocardial infarction complicated with profound cardiogenic shock. CritCare Med. 2010;38:1810–1817. Tsao et al. Extracorporeal membrane oxygenation-assisted primary percutaneouscoronary intervention may improve survival of patients with acute myocardialinfarction complicated by profound cardiogenic shock. J Crit Care. 2012;27(530):e1–e11. Del Sorbo, Lorenzo, Marcelo Cypel, and Eddy Fan. Extracorporeal life support foradults with severe acute respiratory failure. The Lancet Respiratory Medicine. 2014;2.2: 154-164. Schmidt et al. Predicting survival after ECMO for refractory cardiogenic shock: thesurvival after veno-arterial ECMO (SAVE score). European Heart Journal. 2015.Doi10.1093/eurheart/ehv194. Schmidt et al. Predicting Survival after ECMO for Severe Acute Respiratory Failure: Therespiratory ECMO Survivial Predication (RESP score).American Journal RespiratoryCritical Care Medicine. 2014. Doi10.1164/rccm.201311-2023OC. West, John. Respiratory Physiology: The Essentials. Ninth Edition. Lippincott, Williamsand Wilkins. 2012. Philadelphia, PA. Lazar DA et al. Venovenous cannuilation for extracorporeal oxygenation using abicaval dual-lumen catheter in neonates. J of Pediatric Surgery. 2012;47:430-34. Rao P et al. Venoarterial extracorporeal membrane oxygenation for cardiogenic shockand cardiac arrest. J of Circ Heart Failure. 2018;11:1-17. Chauhan S, Subin S. Extracorporeal membrane oxygenation, an anesthesiologist’sperspective: physiology and principles. Part I. Ann of Card Anesth. 2011;14:218-219. Schmidt M et al. Predicting Survival after Extracorporeal membrane Oxygenation forSevere Acute Respiratory Failure. The Respiratory Extracorporeal membraneOxygenation Survival prediction Score. American Journal of Repiratory and CriticalCare Medicine. 2014; 189;11. Schmidt M et. Al. Predicting Survival after Extracorporeal membrane Oxygenation forRefractory shock: The SAVE Score. European Heart Journal. 2015; 36;33;2246-4456.32
33
Figure 4 Maquet Cardiohelp System. Adapted from the Maquet Cardiohelp brochure Maquet Rotaflow - alternative option, can only be managed by a perfusionist Figure 5. Maquet Rotaflow ECMO system. Adapted from Getinge rotoflow brochure. Blood Pump: Centrifugal Note with the cardiohelp system, the disposable component