Transcription
August 2020Advising Congress on Medicaid and CHIP PolicyDirected Payments in Medicaid Managed CareThe 2016 Medicaid managed care rule created a new option for states to require managed care plans topay providers according to specific rates or methods, referred to as directed payments. Typically, directedpayments are used to establish minimum payment rates for certain types of providers or to requireparticipation in value-based payment arrangements that advance the state’s quality and access goals.This brief reviews the history of directed payment policy and examines the use of directed payments basedon MACPAC’s review of directed payments approved as of June 6, 2019.Supplemental Payments and Managed CareUnder the Medicaid statute, states have broad flexibility to design their own payment methods under feefor-service (FFS) arrangements. The two broad categories of payments are (1) base payments, which arepaid per service, and (2) supplemental payments, which are typically made in a lump sum for a fixed periodof time (MACPAC 2020a). In fiscal year (FY) 2018, states made a total of 56 billion in supplementalpayments to hospitals, mental health facilities, nursing facilities, and physicians, which was 36 percent oftotal FFS payments to these providers (MACPAC 2019a).States also have flexibility to finance the non-federal share of Medicaid payments from multiple sources,including state general funds, provider taxes, and intergovernmental transfers (IGTs) from localgovernments. In general, most FFS base payments are financed by state general funds, while most FFSsupplemental payments are financed by provider taxes or IGTs (MACPAC 2020a).1Under actuarial soundness rules, states may not make supplemental payments for services covered underthe managed care contract. This is because if rates are sufficient to cover the reasonable, appropriate, andobtainable costs of providing services covered under the managed care contract, then plans and providerswould not need additional payments for these services.One consequence of the move to managed care is that it can lead to a loss of supplemental paymentfunding for some providers. Such losses can be substantial given that as of July 2017, over two-thirds ofMedicaid enrollees were enrolled in managed care, and managed care accounted for about half ofMedicaid benefit spending in FY 2018 (MACPAC 2019a). For this reason, some states excluded certainservices or populations from managed care or sought demonstration waiver authority under Section 1115of the Social Security Act to continue making supplemental payments that are tied to delivery systemreforms or uncompensated care costs.2Prior to 2016, a small number of states offset the loss of FFS supplemental payments by increasingcapitation rates paid to managed care organizations (MCOs) and requiring MCOs to direct these additional
2funds to particular providers. These payments, known as pass-through payments, were typically not tied touse of services and were often financed by providers through IGTs or provider taxes.In 2016, the Centers for Medicare and Medicaid Services (CMS) made a comprehensive update to Medicaidmanaged care regulations (CMS 2016).3 As part of this regulatory update, CMS required states to phaseout the use of pass-through payments while also creating a new option for states to direct payments toproviders under certain conditions. Specifically, CMS required that directed payments be tied to utilizationand delivery of services, be distributed equally to specified providers under the managed care contract,advance at least one goal in the state’s managed care quality strategy, and not be conditioned on providerparticipation in intergovernmental transfer (IGT) agreements (42 CFR § 438.6(c)).As noted above, states may also use Section 1115 demonstration waivers to continue makingsupplemental payments to some providers, such as delivery system reform incentive payments (DSRIP).However, CMS has indicated that it does not plan to renew existing DSRIP demonstrations and isencouraging states to develop plans to sustain the progress made on delivery system reform goals underDSRIP by increasing the use of value-based payment (VBP) strategies in managed care. Directed paymentsare one mechanism that states can use to require MCOs to use specific VBP models.Directed Payment OptionsIn 2017, CMS issued additional guidance and a pre-print form for states to use when applying for approvalof directed payment arrangements (CMS 2017). The pre-print form includes checkboxes and spaces forstates to indicate the option it is pursuing and describe its program.4 Directed payment arrangements arecategorized into two broad categories: State-directed fee schedules with minimum and maximum amounts for particular services, or uniformdollar or percentage increase in payment above negotiated capitated rates. The state may propose touse an approved state plan fee schedule, a Medicare fee schedule, or an alternative fee scheduleestablished by the state. Value-based purchasing directed payment arrangements require payments to participate in specifiedVBP initiatives, such as pay-for-performance incentives or shared-savings arrangements foraccountable care organizations (ACOs). States may also design their own VBP models.States do not have to have a directed payment arrangement in order for MCOs to adopt state plan paymentrates or to implement value-based payment arrangements; current regulations allow MCOs to negotiatesuch provider payment policies. For example, in MACPAC’s recent review of hospital payment policies infive states, several MCOs noted that they paid hospitals using state FFS payment rates and methods eventhough it was not required (Marks et al. 2018). Similarly, in MACPAC’s review of value-based payment inmanaged care, several MCOs reported that they were implementing VBP initiatives without a state-directedpayment (Bailit 2020).
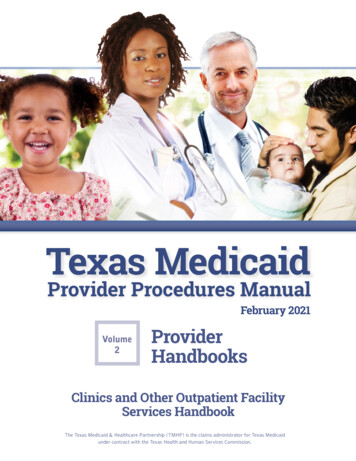
3CMS Review ProcessCMS reviews directed payment pre-prints using a process similar to that used to review Medicaid stateplan amendments. After an initial review of the state submission, CMS may send clarifying questions andrequest revisions before official approval. Directed payment arrangements are typically approved for oneyear at a time (to correspond with the length of MCO contracts and capitation rate approvals), but statescan receive multi-year approval in some circumstances. CMS has not made approved directed paymentpre-prints publicly available.After approval, states must incorporate the directed payment arrangement into their managed carecontracts and capitation rates. The portion of the capitation rate that is attributable to directed paymentsis included in the actuarial rate certification that CMS reviews, but information on spending on directedpayment arrangements is not publicly available.Use of Directed PaymentsAs of June 6, 2019, CMS had approved 121 directed payment arrangements in 34 states.5 About threequarters of those were state-directed fee schedules, and about one-quarter were state-directed VBParrangements (Figure 1).FIGURE 1. Distribution of Types of Approved Directed Payment Arrangements, 2019Directedfeeschedules76%Fee schedule typeMinimum fee scheduleUniform dollar orpercentage increaseMaximum feescheduleVBP24%Share of fee schedulearrangements61%34%11%VBP typePay for performancePopulation-basedpaymentBundled paymentOtherShare of VBParrangements52%24%7%31%Notes: VBP is value-based purchasing. Based on analysis of 121 directed payment arrangements approved as of June 6, 2019.Analysis excludes prior versions of directed payment arrangements that have been renewed or amended after they were initiallyapproved (n 57). Totals do not sum because one directed payment arrangement can include multiple types of fee schedules orVBP.Source: MACPAC, 2020, analysis of directed payment pre-prints approved as of June 6, 2019.
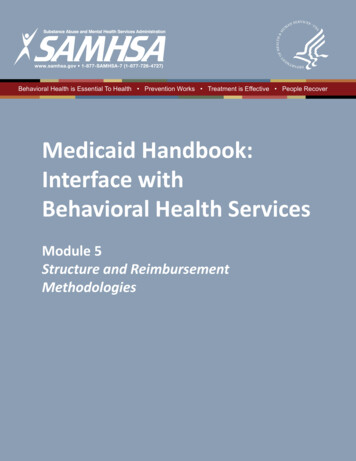
4Directed fee schedulesAlmost two-thirds of directed fee schedule directed payment arrangements approved as of June 2019established a minimum fee schedule for a class of providers. Most of these arrangements required MCOsto use the Medicaid state plan fee schedule or the Medicare fee schedule. About one-third of directed feeschedule arrangements required MCOs to increase payments to providers by a uniform dollar amountduring the managed care rate year, similar to a lump sum supplemental payment in FFS which is alsomade for a fixed period of time (Table 1).Of the 92 unique state directed fee schedules, 40 (43 percent) were targeted to hospitals and 32 (35percent) were financed by provider taxes or IGTs, which was slightly higher than the share that werefinanced by state general funds (32 percent). Other provider types targeted included physicians, mentalhealth providers (institutions and practitioners), and nursing facilities.TABLE 1. Number and Type of State Directed Fee Schedules by Provider Type and Funding Source,2019Program characteristicsTotalProvider typeHospitalsPhysicians and otherprofessional service providersMental health providersNursing facilitiesDental providersHCBS providersTransportation providersOther clinicsFunding sourceState general fundIntergovernmental transferHealth care-related taxOther non-state general fundNot specifiedType of directed fee scheduleMinimum feeUniform dollar orMaximum feeschedulepercentage increaseschedule563110Total uniqueprogramsShare 31011114–912–129181453432%20%15%5%37%Notes: HCBS is home and community-based services. Totals do not sum because a single directed payment arrangementcan target multiple provider types or have multiple funding sources.– Dash indicates zero.Source: MACPAC, 2020, analysis of directed payment pre-prints approved as of June 6, 2019.States are using directed payments for a variety of purposes. The amount of spending also varies.6 Forexample, New Jersey estimated that its program to increase payments for childhood screenings by 10per visit would cost a total of 5.9 million; Michigan estimated that its hospital rate increase program
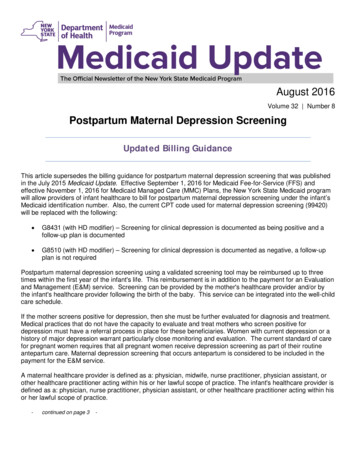
5would cost a total of 1.7 billion. In state fiscal year (SFY) 2016, directed payments accounted for 40percent of managed care payments to hospitals and were larger than FFS supplemental payments tohospitals in Michigan (Marks et al. 2018).7Value-based purchasingAbout half of the 29 VBP directed payment arrangements approved as of June 2019 were pay-forperformance incentives, and the rest were tied to cost and quality goals, such as bundled payments orshared savings payments to ACOs.8 State-directed VBP programs were often targeted to hospitals. MostVBP directed payment arrangements (62 percent) were financed with state general funds, which is higherthan the share financed by IGTs or provider taxes (17 percent) (Table 2).TABLE 2. Number and Type of State Directed Value-Based Purchasing Programs by Provider Type andFunding Source, 2019ProgramcharacteristicsTotalProvider typeHospitalsPhysicians and otherprofessional serviceprovidersMental healthprovidersNursing facilitiesDental providersHCBS providersTransportationprovidersOther clinicsFunding sourceState general fundIntergovernmentaltransferHealth care-related taxNot specifiedPay forperformance(Category 2APM)15Type of directed VBPBundledPopulationpaymentbased payment(Category 3(Category 4APM)APM)27Total uniqueprogramsOther �––––3––132710%7%24%Notes: APM is alternative payment model. APM categories refer to the categories identified by the Healthcare Payment Learning and ActionNetwork. HCBS is home and community-based services. Totals do not sum because a single directed payment arrangement can targetmultiple provider types or have multiple funding sources.– Dash indicates zero.Source: MACPAC, 2020, analysis of directed payment pre-prints approved as of June 6, 2019.
6In some states, directed payments are being used to complement and sustain DSRIP programs. Forexample, in SFY 2018, California was authorized to make 640 million in directed payments to publichospitals as part of its Quality Incentive Payment (QIP) program, in addition to the 1.4 billion in paymentsfor these hospitals that was authorized under the state’s Public Hospital Redesign Incentives in Medi-Cal(PRIME) program (the successor to the state’s DSRIP program).9 In October 2019, the state released aproposal to fully transition its PRIME program to a managed care directed payment that would make asimilar amount of payments to safety net hospitals based on performance on a common set of qualitymeasures (DHCS 2019).Policy IssuesAlthough many directed payment arrangements codify FFS payment policies in managed care, someprovide large amounts of additional funding to providers above the base payment rate for services. Theseadditional payments to providers in managed care raise many of the same types of policy questions assupplemental payments in FFS. Specifically, questions arise about whether this additional funding istargeted appropriately and based on measures of need rather than on the availability of financing for thenon-federal share of the payment. However, provider-level data on directed payments are not available tothat would allow us to analyze these questions.In 2018, CMS proposed modifying its review process for directed payments; the agency would no longerrequire additional review of state directed fee schedules that use approved FFS rates and would allow formulti-year approval of VBP directed payment arrangements. In addition, CMS proposed allowing states tomake new pass-through payments for up to three years for populations or services that are newlytransitioned from FFS to managed care (CMS 2018). This proposed rule has not been finalized.In MACPAC’s comment letter on the proposed 2018 managed care rule, the Commission raised concernsabout the lack of transparency of directed payments and pass-through payments and suggested that CMScollect and report payment data at the provider level. In addition, the Commission also noted theimportance of monitoring the existing requirement that directed payments advance the goals of a state’smanaged care quality strategy (MACPAC 2019b).10Endnotes1In state fiscal year 2012, 70 percent of FFS base payments were financed by state general funds, compared to 36 percentof disproportionate share hospital (DSH) payments and 22 percent of non-DSH supplemental payments financed by stategeneral funds (GAO 2015).2For example, 12 states currently have approved delivery system reform incentive payment (DSRIP) or DSRIP-like programs,and 9 states have uncompensated care pools authorized under Section 1115 demonstrations (MACPAC 2020b).3In 2018, CMS proposed additional revisions to this rule that have not yet been finalized (CMS 2018).
74The directed payment pre-print does not include specific questions about how states finance directed payments, but statesmay include information on the funding sources for directed payment arrangements on their applications or in response toquestions from CMS.5Analysis excludes prior versions of directed payment arrangements that have been renewed or amended after they wereinitially approved (n 57).6Although CMS does not include a question on the directed payment pre-prints about states’ anticipated spending underdirected fee schedules, some states included this information in their responses to CMS’s questions.7MACPAC interviewed Michigan state officials in 2018 as part of a study about the development of Medicaid hospitalpayment policies and learned that the state’s directed payment arrangement is intended to preserve funding to hospitalspreviously made through pass-through payments that are no longer permissible under the 2016 managed care rule. Stateofficials noted that the transition from pass-through payments to directed payments resulted in a change in the distributionof payments among hospitals because of the requirement that directed payments be tied to the utilization and delivery ofservices. This directed payment arrangement is financed by provider taxes and the total amount of funding is based on theamount of provider tax revenue received (Marks et al. 2018).8The directed payment pre-print provides states with the option to classify their VBP models using the Health Care PaymentLearning and Action Network framework, but among the pre-prints that MACPAC reviewed, not all states used thisframework and some directed payment arrangements overlapped multiple categories.9The amount of funding under the QIP program is based on the amount of pass-through payments that California waspreviously making to public hospitals. The quality improvement goals for QIP are intended to be complimentary to the qualityimprovement goals for PRIME (CAPH 2018).10State quality strategies are public documents that outline the goals of each state’s managed care program and its processfor conducting independent reviews of MCO performance. The 2016 managed care rule added the requirement that statemanaged care quality strategies be updated and evaluated at least once every three years (42 CFR § 438.340).ReferencesBailit Health. 2020. State strategies to promote value-based payment through Medicaid managed care: Final report to theMedicaid and CHIP Payment and Access Commission. Washington, DC: Bailit n-five-states/California Association of Public Hospitals (CAPH). 2018. Quality incentive program: Medicaid managed care rule. September14. Oakland, CA: CAPH. ram-medicaid-managed-care-rule/.Centers for Medicare & Medicaid Services (CMS), U.S. Department of Health and Human Services. 2020. CMCS Informationalbulletin regarding “Medicaid Managed Care Options in Responding to COVID-19.” May 14, 2020. Baltimore, MD: ters for Medicare & Medicaid Services (CMS), U.S. Department of Health and Human Services. 2018. Medicaid Program:Medicaid and the Children’s Health Insurance Program (CHIP) Managed Care. Proposed Rule. Federal Register 83, no. 220(November 14): 57264–57299. ns-health-insurance-plan-chip-managed-care.
8Centers for Medicare & Medicaid Services (CMS), U.S. Department of Health and Human Services. 2017. CMCS Informationalbulletin regarding “Delivery system and provider payment initiatives under Medicaid managed care contracts.” November 2,2017. Baltimore, MD: CMS. ownloads/cib11022017.pdf.Centers for Medicare & Medicaid Services (CMS), U.S. Department of Health and Human Services. 2016. Medicaid andChildren's Health Insurance Program (CHIP) Programs; Medicaid Managed Care, CHIP Delivered in Managed Care, andRevisions Related to Third Party Liability. Final Rule. Federal Register 81, no. 88 (May 6): 16-09581.Department of Health Care Services (DHCS), State of California. 2019. California advancing and innovating Medicaid(CalAIM) proposal. October 28, 2019. Sacramento, CA: /CalAIM/CalAIM Proposal 102819.pdf.Marks, T. K. Gifford, S. Perlin, et al. 2018. Factors affecting the development of Medicaid hospital payment policies: Findingsfrom structured interviews in five states: Final report to the Medicaid and CHIP Payment and Access Commission.Washington, DC: Health Management Associates. states/.Medicaid and CHIP Payment and Access Commission (MACPAC). 2019a. MACStats: Medicaid and CHIP data book.December 2019. Washington, DC: MACPAC. https://www.macpac.gov/macstats/.Medicaid and CHIP Payment and Access Commission (MACPAC). 2019b. Letter from Penny Thompson to Seema Vermaregarding “CMS-2408-P Medicaid program: Medicaid and Children’s Health Insurance Plan (CHIP) managed care.” January14, 2019. naged-care-rule/.Medicaid and CHIP Payment and Access Commission (MACPAC). 2020a. Base and supplemental payments to hospitals.Washington, DC: MACPAC. nd-supplemental-payments-to-hospitals/.Medicaid and CHIP Payment and Access Commission (MACPAC). 2020b. Delivery system reform incentive paymentprograms. Washington, DC: MACPAC. -reform-incentive-paymentprograms/.Pettersson, J., B. Mori, L. Roth, and J. Clarkson. 2018. Approved Medicaid state directed payments: How states are using §438.6(c) “preprints” to respond to the managed care final rule. Seattle, WA: re-using-438 ule/.U.S. Government Accountability Office (GAO). 2015. States' increased reliance on funds from health care providers and localgovernments warrants improved CMS data collection. Report no. GAO-14-627. Washington, DC: GAO.https://www.gao.gov/products/D08098.
The 2016 Medicaid managed care rule created a new option for states to require managed care plans to pay providers according to specific rates or methods, referred to as directed payments. Typically, directed . to use the Medicaid state plan fee schedule or the Medicare fee schedule. About one-third of directed fee