Transcription
(2021) 21:195Min et al. BMC ARCH ARTICLEOpen AccessA comparison of postoperative outcomesafter open and laparoscopic reductionof Petersen’s Hernia: a multicenter observationalcohort studyJae‑Seok Min1†, Kyung Won Seo2†, Sang‑Ho Jeong3,5* , Ki Hyun Kim2, Ji‑ho Park4, Ki Young Yoon2,Tae‑Han Kim5, Eun‑Jung Jung3, Young‑tae Ju3, Chi‑Young Jeong3, Ju‑Yeon Kim3 and Young‑Joon Lee3AbstractBackground: The aim of this multicenter cohort study was to compare the clinical courses between open and lapa‑roscopic Petersen’s hernia (PH) reduction.Method: We retrospectively collected the clinical data of patients who underwent PH repair surgery after gastrec‑tomy for gastric cancer from 2015–2018. Forty patients underwent PH reduction operations that were performed bysix surgeons at four hospitals. Among the 40 patients, 15 underwent laparoscopic PH reduction (LPH), and 25 under‑went open PH reduction (OPH), including 4 patients who underwent LPH but required conversion to OPH.Results: We compared the clinical factors between the LPH and OPH groups. In the clinical course, we found nodifferences in operation times or intraoperative bowel injury, morbidity, or mortality rates between the two groups(p 0.05). However, the number of days on a soft fluid diet (OPH vs. LPH; 5.8 vs. 3.7 days, p 0.03) and length of hospi‑tal stay (12.6 vs. 8.2 days, p 0.04) were significantly less in the LPH group than the OPH group. Regarding postopera‑tive complications, the OPH group had a case of pneumonia and sepsis with multi-organ failure, which resulted inmortality. In the LPH group, one patient experienced recurrence and required reoperation for PH.Conclusion: Laparoscopic PH reduction was associated with a faster postoperative recovery period than open PHreduction, with a similar incidence of complications. The laparoscopic approach should be considered an appropriatestrategy for PH reduction in selected cases.Keywords: Petersen’s hernia, Internal hernia, Laparoscopy, Gastric neoplasm*Correspondence: jshgnu@gmail.com†Jae-Seok Min and KyungWon Seo contributed equally to this study5Department of Surgery, Gyeongsang National University Collegeof Medicine and Gyeongsang National University Changwon Hospital,11, Samjeongja‑ro, Seongsan‑gu, Changwon‑si, Gyeongsangnam‑do,Republic of KoreaFull list of author information is available at the end of the articleBackgroundInternal hernia can occur as a result of the artificial mesenteric opening left by entero-entero anastomosis orPetersen’s space after a Roux-en-Y anastomosis. Petersen’s hernia (PH) is rare but potentially fatal complicationthat can develop as the result of strangulation or perforation of a herniated small bowel [1]. Therefore, PH shouldbe treated as soon as possible following its detection.Recently, it was reported that the incidence of internalhernia was higher after laparoscopic gastrectomy than The Author(s) 2021. Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, whichpermits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to theoriginal author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images orother third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit lineto the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutoryregulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of thislicence, visit http:// creat iveco mmons. org/ licen ses/ by/4. 0/. The Creative Commons Public Domain Dedication waiver (http:// creat iveco mmons. org/ publi cdoma in/ zero/1. 0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
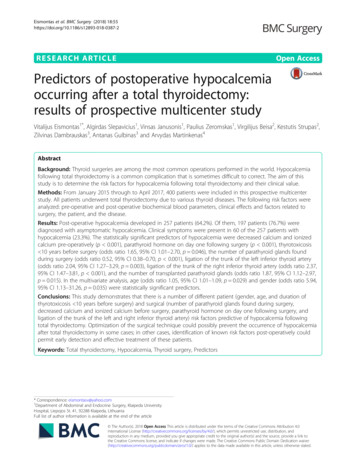
Min et al. BMC Surg(2021) 21:195after open gastrectomy, possibly because of poor adhesion after laparoscopic surgery [2].Laparoscopic surgery is a recommended treatmentmodality for cancer (stomach, colon, liver, biliary)because it is associated with faster postoperative recovery, a lower incidence of complications, and better quality of life outcomes of patients than open surgery [3–8].Laparoscopic internal hernia reduction in the small segment of the small bowel has been reported, but the surgical outcomes associated with laparoscopic PH reductionhave not been reported [9, 10]. The aim of this multicenter cohort study was to compare the clinical coursesbetween open and laparoscopic PH reductions. This isthe first report involving a large multicenter cohort ofgastric cancer patients after gastrectomy.MethodsA retrospective observational study was designed andcarried out according to the principles of the Declarationof Helsinki, 1989. This study was approved by the institutional review board (approval number of first author’sinstitution, IRB-D-1909-009-002, and correspondingauthor’s institution, GNUH-IRB-2020-3-32).Page 2 of 7Fig. 1 Diagram of patient enrollmentOperationsDecision of open vs. laparoscopic reductionThe decision to perform laparoscopic reduction or openreduction was made by the surgeon after determiningwhether the patient had undergone laparoscopic surgeryin the past, whether the patient presented with poor vitalsigns in the emergency room, and the statuses of boweledema and dilation in the abdominal cavity on abdominalCT.PatientsWe retrospectively collected the clinical data of patientswho underwent PH repair surgery after gastrectomy forgastric cancer from 2015–2018. Between 2015 and 2018,a total of 40 PH operations were performed at four hospitals (Changwon & Jinju Gyeongsang National University Hospitals, Dongnam Institute of Radiological andMedical Sciences, and Kosin University Gospel Hospital). Among the 40 patients, 15 underwent laparoscopicPH reduction (LPH), 4 underwent LPH with open conversion, and 21 underwent open PH reduction (OPH).Therefore, a total of 25 patients underwent OPH (Fig. 1).Six expert surgeons have been meeting and sharingtheir experiences with LPH. All the surgeons were specialists in laparoscopic gastrectomy with experience inperforming more than 200 cases.The data of patients who underwent emergency surgery from 2015 to 2018 for mechanical ileus caused byPH were collected. The inclusion criteria for this studywere as follows: (1) previous radical surgery for histologically proven gastric adenocarcinoma; and (2) no evidenceof other distant metastases.We collected data regarding the operation, postoperative complications, and course by retrospective chartreview after surgery. We compared the past gastric cancer surgery method, TNM stage, surgical information,and postoperative course.Open reductionThe operation began with an incision at the site of theprevious incision, and an additional incision was madeif necessary. During the incision, adhesiolysis was carefully performed to prevent injury to organs with adhesions. After the abdominal wall was opened, the viabilityof the herniated small bowel was determined. If the herniation direction was easy to detect, surgery was performed immediately. However, it was sometimes difficultto determine the correct direction of herniation. In thesecases, we performed the following. First, we identified theileocaecal valve and fully reduced the herniated bowel.After complete reduction, we checked the status of bowelperforation and necrosis. If the bowel was not viable evenafter reduction, we resected the damaged small bowelsegment. We closed Petersen’s space with non-absorbable sutures.Laparoscopic reductionWe inserted the first trocar at just inferior to the umbilicus or in the lower abdomen area by an open methodwith a new incision. Mostly, we performed the reduction using three or four trocars. The intra-abdominalreduction process was the same as that performed inthe open method. However, it was difficult to determine
Min et al. BMC Surg(2021) 21:195the correct direction of herniation with a laparoscope.Therefore, we identified the ileocaecal valve, traced thebowel proximally to identify the herniating segment thenreduced it with gentle traction. After complete reduction,we checked the status of bowel perforation and necrosis. If the bowel was not viable even after reduction, weresected the damaged small bowel segment. We closedPetersen’s space with non-absorbable sutures (supplement Video).The possibility of damage or bleeding in the smallintestine is higher during laparoscopic hernia reductionthan during open reduction due to forceful pulling oflaparoscopic graspers. We recommend open conversionfor patients with a poor pneumoperitoneum condition orseverely damaged bowel, as reduction is difficult due tosevere bowel edema.Statistical analysisFor statistical analysis, SPSS Statistics version 24 (IBMSPSS, Inc., Chicago, IL, USA) was used. Continuousdata were compared using unpaired students’ t-test andPage 3 of 7presented as standard deviations, and non-continuous variables were evaluated as chi square tests. For allanalyses, p values below 0.05 were considered statisticallysignificant.ResultsPatient demographicsBetween 2015 and 2018, a total of 40 PH operations wereperformed at the four hospitals. The patient demographics are described in Table 1. The average age of patientswas 63.9 years old, and the ratio of men to women was4:1 (32:8). The TNM stage at past gastrectomy was as follows: the highest was stage I, which accounted for 60%;stage II accounted for 22.5%; stage III was the lowest andaccounted for 5%; and unknown TNM stage accountedfor 12.5%. Regarding past surgeries, there were 11 totalgastrectomies (TGs), 24 distal gastrectomies (DGs) and 2proximal gastrectomies (PGs). The past surgical methodscomprised laparoscopic methods in 28 cases, open methods in 7 cases, and unknown methods in five cases. Themean period between operations was 28.2 months. TheTable 1. Patients demographicsFactorsValueAge (years)SexTNM stage of Gastric cancer*Previous operationPrevious op Approach methodMale8 (20 %)I24 (60%)II9 (22.5%)III2 ( 5%)Unknown5 (12.5%)TG with RNY-EJ11 (27.5%)DG with B II17 (42.5%)DG with RNY-GJ2 (5%)DG with uncut RNY-GJ5 (12.5%)PG with double tract2 (5%)Unknown3 (7.5%)Open gastrectomy28 (70%)Laparoscopy assisted7 (17.5%)Unknown5 (12.5%)28.2 45.7Time duration between pain to hernia operation (hour)Operation timeSmall bowel injury during reductionHospital stay (day)MorbidityMortality32 (80 %)FemalePeriods between previous operation (Month)Approach method63.9 12.1Open reduction51.3 96.421 (52.5%)Laparoscopic reduction15 (37.5%)Open conversion of laparoscopic reduction4 (10.0%)79.5 25.1 minutes4 (10%)10.9 6.84 (10%)1 (2.5%)*AJCC TNM stage 8th edition, GIST gastrointestinal stromal tumor, TG total gastrectomy, RNY Roux-en Y, EJ esophagojejunostomy, B II Billroth II, GJ gastrojejunostomy,PG proximal gastrectomy
Min et al. BMC Surg(2021) 21:195Page 4 of 7mean duration between the presentation of pain and hernia operation was 51.3 h.Regarding the approach for PH reduction, 15 patientsunderwent LPH, 4 patients underwent LPH with openconversion, and 21 underwent OPH. Therefore, a totalof 25 were OPH (Fig. 1). The causes of open conversionwere difficulty in creating a pneumoperitoneum (n 2)and difficulty in laparoscopic reduction due to smallbowel and mesentery thickness (n 2). The mean operation time was 79.5 min; 4 patients experienced smallbowel injury during reduction. The mean hospital staywas 10.9 days. The morbidity rate was 10% (4 cases), andthere was one mortality.operations, TNM stage, previous operation, previousapproach method, preoperative white blood cell (WBC)count, or erythrocyte sedimentation rate (ESR) (p 0.05,Table 2).Comparison of clinical factors between the LPH groupand the OPH groupPostoperative complicationsWe compared the clinical factors between the LPH andOPH groups. We found that the OPH group was older(68.8 years) than the LPH group (55.7 years) (p 0.001)and had a higher C-reactive protein (CRP) level (OPHvs. LPH; 5.5 vs. 0.72, p 0.03). However, there were nodifferences in sex, initial symptoms, duration betweenComparison of operations and postoperative clinicalcourses between the OPH group and LPH groupWe found no differences in operation time or intraoperative bowel injury, morbidity, or mortality rates (p 0.05).However, the number of days on a soft fluid diet (OPH vs.LPH; 5.8 vs. 3.7 days, p 0.03) and length of hospital stay(12.6 vs. 8.2 days, p 0.04) were significantly less in theLPH group than in the OPH group (Table 3).In OPH group, one case of pneumonia and one case ofsepsis with multi-organ failure resulted in mortality. Inthe LPH group, one patients experienced recurrence ofPH at postoperative day 8, and he underwent a secondreduction by the open method (Table 4). The patientwas discharged 16 days after reoperation without othercomplications.Table 2. Clinicopathologic comparison between Laparoscopic reduction group (Laparo group) and open reduction group (Opengroup)FactorsOpen group (N 25)Lapro group (N 15)P value68.8 10.455.7 10.4 .9 56.525.4 20.20.77II45III20unknown5040.0 83.370.7 116.4DG with B II107DG with RNY11DG with uncut RNY22PG with double 0,025 5.0458,546 2,7680.305.5 10.50.72 1.10.03Age (years)SexInitial symptomMalePeriods between previous operation (month)TNM stage of Gastric cancer*ITime duration between pain to hernia operation (hour)Previous operationPrevious approach methodPreop LaboratoryTG with RNY EJESRCRP1914723.7 25.21310416.3 13.9*AJCC TNM stage 8th edition, GIST gastrointestinal stromal tumor, TG total gastrectomy, RNY Roux-en Y, EJ esophagojejunostomy, B II Billroth II, PG proximalgastrectomy, WBC white blood cell, ESR erythrocyte sedimentation rate, CRP C-reactive protein0.680.130.350.500.200.39
Min et al. BMC Surg(2021) 21:195Page 5 of 7Table 3. Comparisons of operation data and postoperativeclinical courses between the open reduction group (Opengroup) and laparoscopic reduction group (Laparo group).Clinical factorOpen group (N 25,%)Lapro group (N 15,%)P valueOperation time83.1 26.173.6 23.10.252 (13.3%)0.625.8 3.13.7 2.10.032 (8%)Bowel injury2 (8%)during opera‑tionSFD start dayHospital stayMorbidityMortality12.6 7.41 (4%)8.2 4.90.041 (6.7%)1.001.0ASIS anterior superior iliac spine, SMV superior mesenteric veinTable 4 . Postoperative complicationsComplicationsOpen groupLapro groupPneumonia10Sepsis with multi-organ failure10Petersen’s hernia recur01DiscussionThe aim of this multicenter cohort study was to comparethe clinical courses between open and laparoscopic PHreductions. Laparoscopic reduction is not always possible, but if so then the postoperative recovery courseis generally better, and operative wounds are generallysmaller with the laparoscopic approach than with opensurgery. However, to the best of our knowledge, no onehas reported a comparison between laparoscopic andopen PH reduction. The present multicenter observational cohort study is the first to report some advantageof laparoscopic PH reduction in terms of postoperativerecovery.PH is a very rare disease that occurred in only 0.54%of patients who underwent gastrectomy for gastric cancer (2417; the number of patients requiring PH reductionsurgery was 13) between 2015 and 2018. In a previousstudy, the incidence of PH after gastrectomy was 0.42%,which was similarly low compared to our data [2, 3]. ForPH reduction surgery, the open method is the standard procedure due to the following: first, it is difficult todevelop pneumoperitoneum due to bowel edema andbowel dilation in the abdominal cavity; second, bowelreduction is difficult due to bowel wall and mesenteryedema, and usually the whole small bowel is herniated;third, experience in laparoscopic PH reduction is limited[2, 9, 11]. In our group, the first laparoscopic reductionwas performed in 2014 in Kosin University Hospital;since then, gastric experts from the four centers sharetheir experiences with laparoscopic PH reduction during regular meetings. Sharing their experiences facilitatesthe application of laparoscopic PH reduction becauseall surgeons are gastric cancer surgery specialists withexperience in performing more than 200 laparoscopicgastrectomies.Laparoscopic surgery has advantages. We found thatthe number of days on a soft fluid diet and postoperativehospital length of stay were significantly less in the laparoscopic reduction group than in the open group. Thereason for the faster recovery is likely that laparoscopicsurgery resulted in fewer operative wounds and less painthan open surgery. Additionally, if the bowels were notmanipulated excessively by the surgeon during laparoscopy, a postoperative diet could be permitted quickly,causing a potential decrease in the length of hospital stay.Recently, the application of the laparoscopic approachfor primary gastrectomy has increased; however, onestudy reported the possibility of an increased incidenceof internal hernia [2]. They reported that laparoscopic TGwas associated with a higher incidence of internal herniathan open TG (4.5%, 29/638 vs. 0.8%, 4/475), with thesame results for laparoscopic DG compared with openDG (2.7% vs. 0.9%). In the multivariate analysis, theyfound that non-closure of mesenteric defects, the laparoscopic approach, and a total laparoscopic approach wereindependent risk factors for internal hernia. We expectedthe incidence of PH to be higher in primary laparoscopicgastrectomy patients; however, the incidence of PH washigher in primary open gastrectomy patients. This maybe because more patients underwent open gastrectomythan laparoscopic gastrectomy in the past. Even thoughthere was only a small number of PH cases included inthis study, interestingly, the laparoscopic or open primaryapproach for gastrectomy did not affect the incidenceof PH. In contrast, a recent study reported that closureof the mesenteric space (5.5%) significantly decreasedthe cumulative incidence of reoperation for small bowelobstruction by internal hernia after surgery compared tono mesenteric closure (10.2%) [12]. Therefore, to reducepostoperative complications, especially the incidence ofinternal hernia after gastrectomy surgery, the closure ofmesenteric defects should be performed [2]. The centersincluded in this study routinely repair mesenteric defectsafter gastrectomy and have recently started performingclosure of Petersen’s space to prevent PH.In terms of postoperative complications, pneumonia generally occurs more frequently in patients whoundergo open surgery; open surgery patients also experience more wound pain than patients who undergominimally invasive surgery [7]. In this study, the onepneumonia patient was an 80-year-old individual whowas at increased risk for postoperative complications
Min et al. BMC Surg(2021) 21:195due to age. In the laparoscopic group, a complication ofinternal hernia recurrence after reduction surgery wasobserved. This suggests that we need to close defectsmore carefully because reduction and closure afterlaparoscopic surgery is more difficult than after manualopen surgery.There were some limitations to our study, such asthe small number of PH reduction surgeries especiallylaparoscopic reduction surgeries. All the surgeons participating in the present study were specialists in gastric cancer surgery with experience in performing morethan 200 laparoscopic gastrectomies. However, thesurgeons did not have many chances to face the casesof Petersen’s hernia which needed a reduction surgery,because the incidence of Petersen’s hernia is very low.In addition, since this is a retrospective observationalcohort study, there might be a selection bias in determining the surgical approach method before surgery.The patients were not randomized in choosing theirsurgical approach. The surgeon might have chosenpatients with easy recovery as a laparoscopic approachmethod. Nevertheless, to the best of our knowledge,this is the first report comparing the surgical outcomesassociated with open and laparoscopic approaches forPH reduction.ConclusionsLaparoscopic PH reduction was associated with fasterpostoperative recovery and a similar incidence of complications compared with open surgery. The laparoscopic approach should be considered an appropriatestrategy for PH reduction in selected cases.AbbreviationsPH: Petersen’s hernia; LPH: Laparoscopic Petersen’s hernia reduction; OPH:Open Petersen’s hernia reduction; TG: Total gastrectomy; DG: Distal gastrec‑tomy; PG: Proximal gastrectomy; CRP: C-reactive protein; WBC: White bloodcell; ESR: Erythrocyte sedimentation rate.AcknowledgementsNo applicable.Authors’ contributionsJSM-Conceptualization, Methodology, Validation, Investigation, Resources,Data Curation, Project administration, Writing; KWS-Conceptualization,Methodology, Investigation; SHJ-Conceptualization, Methodology, Investi‑gation, Writing; JHP, KUY, THK-Investigation, Resources, Data collection; EJJ,YTJ, CYJ, JYK, YJL-Investigation, Data collection, project administration. Allauthors, JSM, KWS, SHJ, JHP, KUY, THK, EJJ, YTJ, CYJ, JYK, and YJL have read andapproved the manuscript for publication. All authors read and approved thefinal manuscript.FundingNot Applicable.Availability of data and materialsNot Applicable.Page 6 of 7DeclarationsEthics approval and consent to participateAll procedures followed were in accordance with the ethical standards of theresponsible committee on human experimentation (institutional and national)and with the Helsinki Declaration of 1964 and later versions. The exemp‑tion from informed consent requirement was permitted by GyeongsangNational University Hospital in Changwon (GNUCHIRB-202003032) and atthe Dongnam Institute of Radiological and Medical Sciences in Busan, KoreaInstitutional Review Board (IRB-D-1909-009-002).Consent for publicationNot Applicable.Competing InterestsDr. Jae-Seok Min, Kyung Won Seo, Ki Hyun Kim, Sang-Ho Jeong, Ji-ho Park, KiYoung Yoon, Tae-Han Kim, Eun-Jung Jung, Young-tae Ju, Chi-Young Jeong,Ju-Yeon Kim, Young-Joon Lee, and have no conflicts of interest or financial tiesto disclose.Author details1Department of Surgery, Cancer Center, Dongnam Institute of Radiologicaland Medical Sciences, Busan, South Korea. 2 Department of Surgery, Kosin Uni‑versity Gospel Hospital, Busan, South Korea. 3 Department of Surgery, Gyeong‑sang National University School of Medicine, Jinju, South Korea. 4 Departmentof Surgery, Gyeongsang National University Hospital, Jinju, South Korea.5Department of Surgery, Gyeongsang National University College of Medicineand Gyeongsang National University Changwon Hospital, 11, Samjeongja‑ro,Seongsan‑gu, Changwon‑si, Gyeongsangnam‑do, Republic of Korea.Received: 28 October 2020 Accepted: 8 April 2021References1. Petersen W. Ueber darmveschlingung nach der gastro-enterostomie.Arch Klin Chir. 1900;62:94–114.2. Kang KM, Cho YS, Min SH, Lee Y, Park KB, Park YS, Ahn SH, Park DJ, Kim HH.Internal hernia after gastrectomy for gastric cancer in minimally invasivesurgery era. Gastric Cancer. 2019;22:1009–15.3. Guideline Committee of the Korean Gastric Cancer Association (KGCA),Development Working Group & Review Panel. Korean practice guidelinefor gastric cancer 2018: an evidence-based, multi-disciplinary approach. JGastric Cancer. 2019;19:1–48.4. Kim W, Kim HH, Han SU, Kim MC, Hyung WJ, Ryu SW, Cho GS, Kim CY,Yang HK, Park DJ, Song KY, Lee SI, Ryu SY, Lee JH, Lee HJ, Korean Laparoendoscopic Gastrointestinal Surgery Study Group. Decreased morbidityof laparoscopic distal gastrectomy compared with open distal gastrec‑tomy for stage i gastric cancer: short-term outcomes from a multicenterrandomized controlled trial (KLASS-01). Ann Surg. 2016;263:28–35.5. Hu Y, Huang C, Sun Y, Su X, Cao H, Hu J, Xue Y, Suo J, Tao K, He X, Wei H,Ying M, Hu W, Du X, Chen P, Liu H, Zheng C, Liu F, Yu J, Li Z, Zhao G, ChenX, Wang K, Li P, Xing J, Li G. Morbidity and mortality of laparoscopic versusopen d2 distal gastrectomy for advanced gastric cancer: a randomizedcontrolled trial. J Clin Oncol. 2016;34:1350–7.6. Johansson M, Thune A, Nelvin L, Stiernstam M, Westman B, Lundell L.Randomized clinical trial of open versus laparoscopic cholecystectomy inthe treatment of acute cholecystitis. Br J Surg. 2005;92:44–9.7. Qaseem A, Snow V, Fitterman N, Hornbake ER, Lawrence VA, Smetana GW,Weiss K, Owens DK, Aronson M, Barry P, Casey DE Jr, Cross JT Jr, FittermanN, Sherif KD, Weiss KB. Risk assessment for and strategies to reduce perio‑perative pulmonary complications for patients undergoing noncardio‑thoracic surgery: a guideline from the American College of Physicians.Ann Intern Med. 2006;144:575–80.8. Veldkamp R, Kuhry E, Hop WC, Jeekel J, Kazemier G, Bonjer HJ, HaglindE, Påhlman L, Cuesta MA, Msika S, Morino M, Lacy AM. Laparoscopicsurgery versus open surgery for colon cancer: short-term outcomes of arandomised trial. Lancet Oncol. 2005;6:477–84.
Min et al. BMC Surg9.(2021) 21:195Sakamoto T, Kawarai Lefor A. Laparoscopic reduction and closure ofan internal hernia secondary to gynecologic surgery. Case Rep Surg.2017;2017:5948962.10. Goudsmedt F, Deylgat B, Coenegrachts K, Van De Moortele K, Dil‑lemans B. Internal hernia after laparoscopic Roux-en-Y gastric bypass:a correlation between radiological and operative findings. Obes Surg.2015;25:622–7.11. Kojima K, Inokuchi M, Kato K, Motoyama K, Sugihara K. Petersen’s herniaafter laparoscopic distal gastrectomy with Roux-en-Y reconstruction forgastric cancer. Gastric Cancer. 2014;17:146–51.Page 7 of 712. Stenberg E, Szabo E, Agren G, Ottosson J, Marsk R, Lonroth H, Boman L,Magnuson A, Thorell A, Naslund I. Closure of mesenteric defects in lapa‑roscopic gastric bypass: a multicentre, randomised, parallel, open-labeltrial. Lancet. 2016;387:1397–404.Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims in pub‑lished maps and institutional affiliations.Ready to submit your research ? Choose BMC and benefit from: fast, convenient online submission thorough peer review by experienced researchers in your field rapid publication on acceptance support for research data, including large and complex data types gold Open Access which fosters wider collaboration and increased citations maximum visibility for your research: over 100M website views per yearAt BMC, research is always in progress.Learn more biomedcentral.com/submissions
pitals (Changwon & Jinju Gyeongsang National Univer-sity Hospitals, Dongnam Institute of Radiological and Medical Sciences, and Kosin University Gospel Hospi-tal). Among the 40 patients, 15 underwent laparoscopic PH reduction (LPH), 4 underwent LPH with open con-version, and 21 underwent open PH reduction (OPH).