Transcription
PostoperativePain Management –Good ClinicalPracticeGeneral recommendationsand principles forsuccessful pain managementProduced in consultation with theEuropean Society of Regional Anaesthesiaand Pain Therapy
Project chairman and co-ordinator:The authors and the publishers have written the information relatingto the medications and their dosages with utmost care and inaccordance with the routines of the authors' clinical practice, whichmay not agree with the manufacturer's recommendations. Therefore,the prescriber is expected to read the dosage recommendations andcontraindications in the prescribing information for the drugs anduse them at their own discretion.Acknowledgements:All rights reserved. This booklet is protected by copyright. No part of thiswork may be processed, translated, reproduced or distributed in any formwhatsoever (by photocopy, microfilm or any other technique) without thewritten consent of the publisher (AstraZeneca).The Wong-Baker Faces Pain Rating Scale is from Hockenbury MJ,Wilson D, Winkelstein ML. Wong's Essentials of Paediatric Nursing, Ed 7,St Louis, 2005, p 1259. Copyright, Mosby. Used with permission fromElsevier.This booklet has been produced in consultation with the EuropeanSociety of Regional Anaesthesia and Pain Therapy (ESRA) with financialsupport from AstraZeneca, including financial support for editorialassistance from Evelyn Frearson BSc and for graphic design by LyntonCreative Communications Ltd.The publishers would like to thank Dag Selander, MD, PhD (Selmedic AB,Gothenburg, Sweden), for his contribution as medical consultantproviding editorial advice and revision during the production of thisbooklet.Professor Narinder Rawal, MD, PhDDepartment of Anesthesiology and Intensive CareÖrebro University HospitalSE-701 85 Örebro, SwedenAuthors:Dr Jose De Andrés, MD, PhDAssociate Professor of AnesthesiologyValencia University Medical SchoolChairman, Department of Anesthesiologyand Critical CareDirector of the Multidisciplinary PainManagement CenterValencia University General HospitalTres Cruces s/n, 46014-Valencia, SpainDr H B J Fischer, MBChB, FRCAConsultant AnaesthetistDepartment of AnaesthesiaAlexandra HospitalWoodrow Drive, RedditchWorcs B98 7UB, EnglandDr Giorgio Ivani, MDPediatric AnesthesiologistChairman, Division PediatricAnesthesia and ICU"Regina Margherita" Children's HospitalPiazza Polonia 94, 10126 Turin, ItalyDr Torben Mogensen, MD, PhDMedical Director, Hvidovre HospitalUniversity of CopenhagenDK-2650 Hvidovre, DenmarkDr Patrick Narchi, MDAnesthesia DepartmentCentre Clinical16800- Soyaux, FranceProfessor François J Singelyn, MD, PhDAssociate ProfessorDepartment of AnesthesiologyUniversité Catholique de Louvain Schoolof MedicineCliniques Universitaires St LucAvenue Hippocrate 10/18211200 Brussels, BelgiumDr Rudolf Stienstra, MD, PhDVice-chairmanDepartment of AnesthesiologyLeiden University Medical CenterLeiden, The NetherlandsProfessor Hinnerk Wulf, MDProfessor and Chairman, Lecturer inAnesthesiology and Intensive CareMedicineDepartment of Anesthesiology andIntensive Care MedicineUniversity HospitalD 35033 Marburg, Germany
PostoperativePain Management –Good ClinicalPracticeGeneral recommendationsand principles forsuccessful pain managementProduced in consultation with theEuropean Society of Regional Anaesthesiaand Pain Therapy
ContentsContentsContents8. Day case surgery331. Introduction and objectives1a. Requirements for effective day case surgery analgesia2. Goals of pain treatment2b. The role of regional analgesia in day case surgery333. Physiology of pain3c. Postoperative pain management in day case surgery34a. Positive role of pain4i. Systemic analgesiab. Negative effects of pain4ii. Regional analgesiac. The mechanism of peripheral pain sensitisation5d. The mechanism of central sensitisation64. Assessment of paina. Specific tools for pain assessmentb. Selection of suitable assessment tool898333535Single shot techniques35Continuous techniques35d. Assessment, documentation and management of painfollowing discharge9. Paediatric analgesia363810a. Symptoms of pain in children385. Patient education11b. Education for children396. Treatment options16c. Assessment of pain in children3916d. Drug selection41i. Balanced (multimodal) analgesia16e. Regional analgesia in children41ii. Opioids19iii. Non-opioids21iv. Adjuvants23v. Regional analgesia2310. Patient groups with special problems for pain managementContinuous Central Neuraxis Blockade (CCNB)2311. Risk management/discharge criteriaContinuous Peripheral Nerve Blockade (CPNB)25a. Sequential analgesia26b. Management of the insensate limb4929c. Support following discharge50c. Documentationa. Pharmacological methods of pain assessmentInfiltration blocksb. Non-pharmacological methods of pain treatment7. Structure of an acute pain management service30i. Local anaesthetic agents42f. Routes of administration42g. Doses of analgesic agents in children4312. Appendix47494951a. Staff training30a. Recommended reading51b. Audit and quality control30b. Useful web sites57c. Sources of patient leaflets57
1. Introduction and objectives1Effective postoperative pain management has a humanitarian role, butthere are additional medical and economic benefits for rapid recoveryand discharge from hospital. A number of factors contribute to effectivepostoperative pain management including a structured acute painmanagement team, patient education, regular staff training, use ofbalanced analgesia, regular pain assessment using specificassessment tools and adjustment of strategies to meet the needs ofspecial patient groups, such as children and the elderly.Recent advances in pain control provide greater potential for effectivepostoperative management. This document reflects the opinions of apanel of European anaesthesiologists. Its aims are to raise awareness ofrecent advances in pain control and to provide advice on how toachieve effective postoperative analgesia. The recommendations andadvice are general principles of pain management and do not providedetailed advice for specific surgical procedures.11Although the choice of drugs shown here is indicative, adjustments will be required to take account ofindividual patient variation and are the responsibility of the prescribing physician.1
232. Goals of pain treatment3. Physiology of painEffective pain management is now an integral part of modern surgicalpractice. Postoperative pain management not only minimises patientsuffering but also can reduce morbidity and facilitate rapid recovery andearly discharge from hospital (see section 8, page 33), which can reducehospital costs.Pain is a personal, subjective experience that involves sensory,emotional and behavioural factors associated with actual or potentialtissue injury. What patients tell us about their pain can be very revealing,and an understanding of how the nervous system responds and adaptsto pain in the short and long term is essential if we are to make sense ofpatients’ experiences. The wide area of discomfort surrounding awound, or even a wound that has healed long ago, such as anamputation stump, is a natural consequence of the plasticity of thenervous system. An understanding of the physiological basis of pain ishelpful to the sufferer, and the professionals who have to provideappropriate treatment.The goals of effective and appropriate pain management are to:lImprove quality of life for the patientlFacilitate rapid recovery and return to full functionlReduce morbiditylAllow early discharge from hospitalAccording to the International Association for the Study of Pain (IASP),pain is defined as"An unpleasant sensory and emotional experience associated withactual or potential tissue damage, or described in terms of suchdamage." (IASP 1979)There is individual variation in response to pain, which is influenced bygenetic makeup, cultural background, age and gender. Certain patientpopulations are at risk of inadequate pain control and require specialattention. These include:lllPaediatric patientsGeriatric patientsPatients with difficulty in communicating (due to critical illness,cognitive impairment or language barriers)Postoperative pain can be divided into acute pain and chronic pain:ll2Acute pain is experienced immediately after surgery (up to 7 days)Pain which lasts more than 3 months after the injury is considered tobe chronic pain3
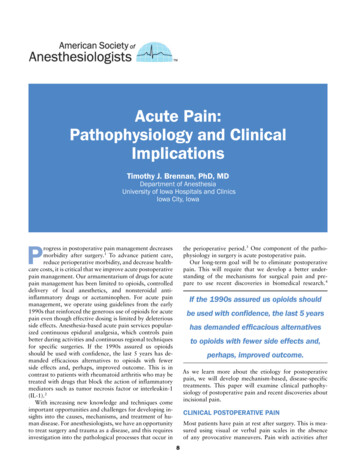
33Acute and chronic pain can arise from cutaneous, deep somatic orvisceral structures. Surgery is typically followed by acute pain and correctidentification of the type of pain enables selection of appropriate effectivetreatment. The type of pain may be somatic (arising from skin, muscle,bone), visceral (arising from organs within the chest and abdomen), orneuropathic (caused by damage or dysfunction in the nervous system).Patients often experience more than one type of pain.Long term negative effects of acute pain:llSevere acute pain is a risk factor for the development of chronicpain1There is a risk of behavioural changes in children for a prolongedperiod (up to 1 year) after surgical painThere are two major mechanisms in the physiology of pain:3.a. Positive role of painlAcute pain plays a useful "positive" physiological role by:lllProviding a warning of tissue damageInducing immobilisation to allow appropriate healing3.b. Negative effects of painNociceptive (sensory): Inflammatory pain due to chemical,mechanical and thermal stimuli at the nociceptors (nerves thatrespond to painful stimuli).Neuropathic: Pain due to neural damage in peripheral nervesor within the central nervous system.During normal physiology, pain sensations are elicited by activity inunmyelinated (C-) and thinly myelinated (Ad-) primary afferent neuronsthat synapse with neurons is the dorsal horn of the spinal cord. Sensoryinformation is then relayed to the thalamus and brainstem.Short term negative effects of acute pain include:lllllllEmotional and physical suffering for the patientSleep disturbance(with negative impact on mood and mobilisation)Cardiovascular side effects(such as hypertension and tachycardia)Increased oxygen consumption(with negative impact in the case of coronary artery disease)Impaired bowel movement(while opioids induce constipation or nausea, untreated pain mayalso be an important cause of impaired bowel movement or PONV*)Negative effects on respiratory function(leading to atelectasis, retention of secretions and pneumonia)Delays mobilisation and promotes thromboembolism(postoperative pain on mobilisation is one of the major causes fordelayed mobilisation)* PONV Postoperative Nausea and Vomiting.4Repetitive activation of C- nociceptive receptors produces alterations incentral as well as peripheral nervous systems.3.c. The mechanism of peripheral pain sensitisationNormally, C- fibres (slow-conducting fibres that transmit dull achingpain) are silent in the absence of stimulation, but following acute tissueinjury in the presence of ongoing pathophysiology, these nociceptorsbecome sensitised and release a complex mix of pain and inflammatorymediators leading to pain sensations (Figure 1, page 6).1Several investigations into chronic pain have concluded that 20% to 50% of all patients with chronic painsyndromes started with acute pain following trauma or surgery, but the role of effective pain treatment in preventingthis risk is not clear.5
3Figure 1.Mechanism of peripheral sensitisation3cord dorsal horn neurons (known as ‘wind up’). This allows the size ofthe dorsal horn neuron’s receptive field to grow (Figure 2). This process,called central sensitisation, occurs with any tissue damage. As withsensitisation of primary afferent nociceptors, this sensitisation of centralpain transmission is a normal physiological response of the undamagednervous system.Figure 2.Pain mediators3.d. The mechanism of central sensitisationThe responses in the CNS are primarily physiological. Centralsensitisation is a physiological process and, only if there is continualfiring of C-nociceptors over time, will these processes leads to morechronic pain syndromes.Sustained or repetitive C-nociceptor activity produces alterations in theresponse of the central nervous system to inputs from the periphery.When identical noxious stimuli are repeatedly applied to the skin at acertain rate, there is a progressive build-up in the response of spinal67
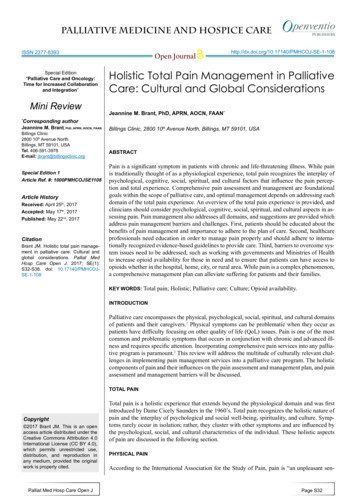
444. Assessment of painAssessment of pain is a vital element in effective postoperative painmanagement. The principles of successful pain assessment are shownin Table 1.lUnexpected intense pain, particularly if associated with altered vitalsigns, (hypotension, tachycardia, or fever), is immediately evaluated.New diagnoses, such as wound dehiscence, infection, or deepvenous thrombosis, should be considered.lImmediate pain relief without asking for a pain rating is given topatients in obvious pain who are not sufficiently focused to use apain rating scale.lFamily members are involved when appropriate.Table 1Principles of successful pain assessmentlAssess pain both at rest and on movement to evaluate the patient'sfunctional status.lThe effect of a given treatment is evaluated by assessing painbefore and after every treatment intervention.lIn the surgical Post Anaesthesia Care Unit (PACU) or othercircumstances where pain is intense, evaluate, treat, and re-evaluatefrequently (e.g. every 15 min initially, then every 1-2 h as pain intensitydecreases).lOn the surgical ward, evaluate, treat, and re-evaluate regularly(e.g. every 4-8 h) both the pain and the patient's response totreatment.lDefine the maximum pain score above which pain relief is offered(the intervention threshold). For example, verbal ratings score of3 at rest and 4 on moving, on a 10-point scale.lPain and response to treatment, including adverse effects, aredocumented clearly on easily accessible forms, such as the vitalsign sheet. This is useful for treatment, good communicationbetween staff, auditing and quality control.l8Patients who have difficulty communicating their pain requireparticular attention. This includes patients who are cognitivelyimpaired, severely emotionally disturbed, children, patients who donot speak the local language, and patients whose level ofeducation or cultural background differs significantly from that oftheir health care team.4.a. Specific tools for pain assessmentSpecific pain assessment scales are used to quantify pain. The use ofone scale within a hospital ensures that everyone in the team "speaks thesame language" regarding the intensity of pain. The patient's own reportis the most useful tool. The intensity of pain should therefore be assessedas far as possible by the patient as long as he/she is able tocommunicate and express what pain feels like. Always listen to andbelieve what the patient says.A number of different patient self-assessment scales are available(Figure 3, page 12):A. Facial expressions: a pictogram of six faces with differentexpressions from smiling or happy through to tearful. This scale issuitable for patients where communication is a problem, such aschildren, elderly patients, confused patients or patients who do notspeak the local language.B. Verbal rating scale (VRS): the patient is asked to rate their pain on afive-point scale as "none, mild, moderate, severe or very severe".9
44C. Numerical rating scale (NRS): This consists of a simple 0 to 5 or0 to 10 scale which correlates to no pain at zero and worst possiblepain at 5 (or 10). The patient is asked to rate his/her pain intensity asa number.llThe treatment strategy to be continued is discussed by the physicianresponsible for the patient in conjunction with the ward nurses.The physician and nurses pay attention to the effects and side effectsof the pain treatment.D. Visual analogue scale (VAS): This consists of an ungraduated,straight 100 mm line marked at one end with the term " no pain" andat the other end "the worst possible pain". The patient makes a crosson the line at the point that best approximates to their pain intensity.The VRS and NRS are the most frequently used assessment tools in theclinical setting while the VAS scale is primarily used as a research tool.4.b. Selection of suitable assessment tool (Figure 3, page 12):When selecting a pain assessment tool ensure that:llIt is appropriate for the patient's developmental, physical, emotional,and cognitive statusIt meets the needs of both the patient and the pain managementteam4.c. DocumentationDocument pain regularly, take appropriate action and monitor efficacyand side effects of treatment. Record the information in a well-definedplace in the patient record, such as the vital sign sheet or a purposedesigned acute pain chart.ll10The nurse responsible for the patient reports the intensity of pain andtreats the pain within the defined rules of the local guidelines.The physician responsible for the patient may need to modify theintervention if evaluation shows that the patient still has significant pain.11
44Figure 3Choice of assessment toolFig A. Wong-Baker Faces Pain Rating Scale1NoFaces painassessmentscale(Fig A)012345NO HURTHURTSLITTLE BITHURTSLITTLE MOREHURTSEVEN MOREHURTSWHOLE LOTHURTSWORST246810AlternatecodingPatient0Fig B. VRS2VRS painassessmentscale(Fig B)able tocommunicateLittlepainNo painMediumpainLargepainWorstpossible painwell ?YesNRSassessmentscale(Fig C)Fig C. NRS20Worstpossible painModerate painNo pain12345678910Fig D. VAS2VASassessmentscale(Fig D)Visual analogue scale (VAS)No pain1212Worstpossible painWith permission from Elsevier.Adapted from McCaffery M, Pasero C. Pain: Clinical Manual 1999 with permission from Elsevier.13
555. Patient educationPatients are unlikely to be aware of postoperative pain treatmenttechniques and as the success of pain relief is influenced by theirknowledge and beliefs, it is helpful to give patients (and parents in caseof children) detailed information about postoperative pain and paintreatment. Adequate information gives the patient realistic expectationsof the care that can be provided (pain relief, not a "pain free status").This information can include:lllllThe importance of treating postoperative painAvailable methods of pain treatmentPain assessment routinesGoals (optimum pain scoring) (see section 2, page 2)The patient's participation in the treatment of painInformation for the patient can be given in different ways (in combination):lllllSelect a pain assessment tool, and teach the patient to use it.Determine the level of pain above which adjustment of analgesia orother interventions will be considered.Provide the patient with education and information about pain control.Emphasise the importance of a factual report of pain, avoidingstoicism or exaggeration.The "Patient Information Project" is a useful source of information forpatients who require information about anaesthesia and postoperativepain management. This is a joint project between the Royal College ofAnaesthetists and the Association of Anaesthetists of Great Britain andIreland, together with patient representative groups. The website is:www.youranaesthetic.infoVerbal informationWritten and/or audiovisual information- Brochures- Wall posters- Video films- Web pagesA preoperative discussion with the patient and relatives can include thefollowing:lll14Discuss the patient's previous experiences with pain and preferencesfor pain assessment and management.Give the patient information about pain management therapies thatare available and the rationale underlying their use.Develop with the patient a plan for pain assessment andmanagement.15
666. Treatment optionsEffective treatment of postoperative pain includes a number of factors,including good nursing, non-pharmacological techniques, such asdistraction, and balanced (multimodal) analgesia to provide adequatepain relief with optimal drug combinations used at the lowest effectivedoses.6.a. Pharmacological methods of pain treatment1Postoperative pain management should be step-wise and balanced(Figure 4, page 18). The four main groups of analgesic drugs used forpostoperative pain management are shown in Table 2 opposite, withexamples of drugs listed in each group.Table 2Pharmacological options of pain managementNon-opioid analgesicsParacetamolNSAIDs, including COX-2 inhibitors*Gabapentin, pregabalin2Weak opioidsCodeineTramadolParacetamol combined with codeineor tramadolStrong odoneAdjuvants**KetamineClonidine6.a.i. Balanced (multimodal) analgesiaBalanced (multimodal) analgesia uses two or more analgesic agents thatact by different mechanisms to achieve a superior analgesic effectwithout increasing adverse events compared with increased doses ofsingle agents. For example, epidural opioids can be administered incombination with epidural local anaesthetics; intravenous opioids can beadministered in combination with NSAIDs, which have a dose sparingeffect for systemically administered opioids.Balanced analgesia is therefore the method of choice wherever possible,based on paracetamol and NSAIDs for low intensity pain with opioidanalgesics and/or local analgesia techniques being used for moderateand high intensity pain as indicated (Figure 4, page 18).* At the time of writing, COX-2 inhibitor drugs are subject to scrutiny by internationalregulatory bodies with regard to adverse outcomes when used for long-term oralprescription or for pain relief in patients with cardiovascular problems such as myocardialinfarction, angina pectoris, hypertension. Rofecoxib has been withdrawn fromsales and prescription of valdecoxib has been suspended pending further research intoits adverse events profile for cardiovascular morbidity and the occurrence of severemuco-cutaneous side effects. The injectable COX-2 inhibitor, parecoxib remains availablefor short-term use in treating postoperative pain. All NSAIDs should be used with care inpatients with cardiovascular disease.** These adjuvants are not recommended for routine use in acute pain managementbecause of their adverse side effects. Their use should be restricted to specialists inmanaging pain problems.116The example doses given are indicative and do not take account of individual patient variation.2Gabapentin and pregabalin are approved for pain management but at the time of writing there is little published datato recommend the use of these drugs for acute pain management.17
66Figure 46.a.ii. Opioids1Treatment options in relation to magnitude of postoperativepain expected following different types of surgery1Table 3Morphine and weak opioidsMildintensity painModerateintensity painSevereintensity painMorphineFor example:Inguinal herniaVaricesLaparoscopyFor example:Hip replacementHysterectomyJaw surgeryFor example:ThoracotomyUpper abdominal surgeryAortic surgeryKnee replacementAdministration(i) Paracetamol and woundinfiltration with localanaestheticDosage:IV PCA(ii) NSAIDs (unlesscontraindicated) and(iii) Epidural local analgesia ormajor peripheral nerve orplexus block or opioidinjection (IV PCA)(i) Paracetamol and wound infiltration withlocal anaestheticSubcutaneous(i) Intravenous.(ii) Subcutaneous by continuous infusion orintermittent boluses via indwelling cannula.(iii) Intramuscular (not recommended due to incidenceof pain. 5-10 mg 3-4 hourly).Bolus: 1-2 mg, lockout: 5-15 min (usually 7-8 min),no background infusion.0.1-0.15 mg/kg 4-6 hourly, adapted in relationto pain score, sedation and respiratory rate.MonitoringPain score, sedation, respiratory rate, side effects.CommentsSide effects such as nausea, vomiting, sedationand apnoea.No other opioid or sedative drug should beadministered.(ii) NSAIDs (unless contraindicated) and(iii) Peripheral nerve block(single shot or continuous infusion) oropioid injection (IV PCA)continued overleaf(i) Paracetamol and wound infiltration with local anaesthetic(ii) NSAIDs (unless contraindicated) and(iii) Regional block analgesiaAdd weak opioid or rescue analgesia with small incrementsof intravenous strong opioid if necessary118The examples given here represent levels of pain commonly experienced and are subject to individual variation andcontra-indications may apply.1The doses and routes of administration of drugs described above are general examples and each patient should beassessed individually before prescribing.19
66Table 3 (continued)6.a.iii. Non-opioids1Table 4CodeineParacetamolAdministrationOralDosage3 mg/kg/day combined with paracetamol.A minimum of 30 mg codeine/tablet is required.MonitoringPain score, sedation, side effects.CommentsAnalgesic action is likely to be due to conversion tomorphine. A small number of patients derive nobenefit due to absence of the converting enzyme.TramadolAdministrationAdministration(i) Intravenous: Start 30 min before the end ofsurgery.(ii) Oral administration as soon as possible.Duration: as long as required.Dosage4 x 1 g paracetamol/day (2 g propacetamol/day).Dose to be reduced (e.g. 3 x 1 g/day) in case ofhepatic insufficiency.MonitoringPain scores.CommentsShould be combined with NSAID and/or opioids orloco-regional analgesia for moderate to severe pain.(i) Intravenous: inject slowly (risk of high incidenceof NV).(ii) Intramuscular.(iii) Oral administration as soon as possible.Table 5Dosage50-100 mg 6 hourly.AdministrationOral.MonitoringPain score, sedation, respiratory rate, side effects.DosageParacetamol 500 mg codeine 30 mg.4 x 1 g paracetamol/day.CommentsTramadol reduces serotonin and norepinephrinereuptake and is a weak opioid agonist.In analgesic efficiency, 100 mg tramadol isequivalent to 5-15 mg morphine.Sedative drugs can have an additive effect.MonitoringPain score, sedation, side effects.CommentsAnalgesic action is likely to be due to conversionto morphine. A small number of patients deriveno benefit due to absence of the convertingenzyme.Combination of codeine paracetamolNV nausea and vomiting120The doses and routes of administration of drugs described above are generally examples and each patient should beassessed individually before prescribing.1The doses and routes of administration of drugs described above are general examples and each patient should beassessed individually before prescribing.21
66Table 66.a.iv. AdjuvantsNSAIDs1Administration(i) Intravenous: administration should start at least30-60 min before end of surgery.(ii) Oral administration should start as soon aspossible.Duration: 3-5 days.Dosage examples(i) Conventional NSAIDs include:ketorolac: 3 x 30-40 mg/day (only IV form)diclofenac: 2 x 75 mg/dayketoprofen: 4 x 50 mg/day(ii) Selective NSAIDs include:meloxicam 15 mg once dailyCOX-2 inhibitors are now licensed for postoperativepain management. They are as efficient asketorolac but reduce GI side effects. Examplesinclude: parecoxib: 40 mg followed by 1-2 x40 mg/day (IV form) or celecoxib: 200 mg/day.However, there is some debate due tocardiovascular risks in patients witharteriosclerosis. *See note below Table 2, page 17MonitoringComments122Pain scores.Renal function in patients with renal or cardiacdisease, elderly patients, or patients with episodesof severe hypotension. Gastrointestinal side effects.Non-selective NSAIDs would be combined withproton inhibitors (i.e. omeprasol) in patients at riskof gastrointestinal side effects.Can be added to the pre-medication.Can be used in association with paracetamoland/or opioids or local regional analgesia formoderate to severe pain.In addition to systemic administration of NSAIDs or paracetamol, weakopioids and non-opioid analgesic drugs may be administered "onrequest" for moderate or severe pain. These include ketamine andclonidine. Clonidine can be administered orally, intravenously orperineurally in combination with local anaesthetics. However, the sideeffects could be significant. The most important ones are hypotensionand sedation. Ketamine can be administered via oral, intramuscular orintravenous routes. It has also significant side effects.6.a.v. Regional analgesiaContinuous Central Neuraxis Blockade (CCNB)CCNB is one of the most effective forms of postoperative analgesia,but it is also one of the most invasive. However, CCNB remains the firstchoice for a number of indications, such as abdominal, thoracic, andmajor orthopaedic surgery, where adequate pain relief cannot beachieved with other analgesia techniques alone.CCNB can be achieved via two routes:llContinuous epidural analgesia - the recommended first choiceContinuous spinal analgesia - should be limited to selected casesonly, as there is less experience with this techniquePostoperative epidural analgesia is usually accomplished with acombination of a long-acting local anaesthetic and an opioid, in diluteconcentrations. Long-acting local anaesthetics are preferred becausethey are associated with less tachyphylaxis. Maintenance techniques inepidural analgesia include:lContinuous Infusion (CI): An easy technique that requires littleintervention. The cumulative dose of local anaesthetic is likely to behigher and side effects are more likely than with the other twotechniques.The doses and routes of administration of drugs described above are general examples and each patient should beassessed individually before prescribing.23
6ll6Intermittent Top-up: Results in benefits due to frequent patient/staffcontact but can produce a high staff workload and patients may haveto wait for treatment.Patient-Controlled Epidural Analgesia (PCEA): This technique produceshigh patient satisfaction and reduced dose requirements compared withCI. However, sophisticated pumps are required and accurate catheterposition is important for optimal efficacy.Examples of drugs and dosages for use in continuous epidural analgesiaare shown in Table 7.Table 7After major orthopaedic lower limb surgery, clinical studies showperipheral nerve blocks are as effective as epidural and that both arebetter than IV opioids. Examples of drugs and dosages for use incontinuous peripheral analgesia are shown in Table
7. Structure of an acute pain management service 30 a. Staff training 30 b. Audit and quality control 30 8. Day case surgery 33 a. Requirements for effective day case surgery analgesia 33 b. The role of regional analgesia in day case surgery 33 c. Postoperative pain management in day case surgery 34 i. Systemic analgesia 35 ii. Regional .