Transcription
IHC IN DIAGNOSTICSTHE SELECTION OF WHICH ANTIBODIES TO USE IN DIAGNOSTICHISTOPATHOLOGY DEPENDS ON SEVERAL VARIABLE:1) Ab AVAILABILITY FOR SPECIFIC ANTIGENS :- SPECIFIC FOR A TISSUE/ ORGAN AND OF THE PATHOLOGICALLESIONS ORIGINATING FROM IT - LINEAGE-SPECIFIC (eg Thyroglobulinfor the thyroid)- SPECIFIC FOR A GROUP OF TISSUES - LINEAGE-RESTRICTED (egcytokeratins in epithelial tissues)2) POSSIBILITY OF ANTIBODIES TO REACT WITH ANTIGEN SPECIFICALLYIN FORMALIN FIXED AND PARAFFIN EMBEDDED TISSUES3) POSSIBILITY OF SEARCHING POSITIVE OR NEGATIVE DIFFERENTANTIGENS TO CONFIRM THE DIAGNOSIS - ANTIBODY PANEL4) HISTOLOGICAL RECOGNITION OF A SUSPECTED LESION FORCONFIRMATION OR DIFFERENTIAL DIAGNOSIS BETWEEN A LIMITEDNUMBER OF LESIONS (eg differential diagnosis between different types ofspindle-cell sarcoma)
IHC IN DIAGNOSTICS1.2.3.4.It requires time, human and financial resourcesMany antibodies with different sensitivity and specificityResult depends on preanalytical factorsSemi-quantitative subjective interpretation. The intensity of thestaining and the percentage of positive cells are evaluated.H score (histo) [1 (% cells 1 ) 2 (% cells 2 ) 3 (% cells 3 )]The score can vary in the range 0 - 300. Cases can be classified as positiveor negative according to specific cut-off.
IHC IN DIAGNOSTICSKnowledge of the nature of targeted antigens is an important factorin the interpretation of the results. The following details are alwaysto consider:ü The expression pattern of the antigens (nuclear, cytoplasmic,membranous, or extracellular).ü Stability of antigens during tissue processing. Optimal andstandardized tissue fixation and processing and as a rule, badH&E sections mean bad immunohistochemistry results.ü Histopathologists deal with neoplasia with heterogeneous cellpopulations with high potential of genotypic and phenotypicvariations. The reason for the atypical antigen expression can bein the biology of the tumor or the nature of the antibodies used.ü Standardized reporting is very helpful in organizing theinformation to reach an accurate diagnosis.ü Despite the high sensitivity of IHC and the large number ofavailable antibodies, immunohistochemistry—as any method—has its own limits.
IHC IN DIAGNOSTICS1. EPITHELIAL Ab2.MESENCHIMAL Ab3.HEMOLYMPHOPOIETIC Ab4.HORMONES, HORMONAL RECEPTORS AND RELATED PROTEINS5.ONCOPROTEIN, GROWTH FACTORS AND THEIR RECEPTORS6.CELL CYCLE ASSOCIATED MARKERS7.MARKERS OF EXTRACELLULAR MATRIX (es Laminins)
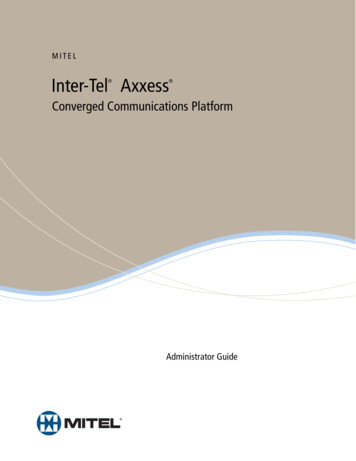
important to remember that the immunoprofileof tumors may be a subject of exceptions or(see carcinomapannels)Cytokeratin positivenon-epithelial tumors(see panel 1.4)LymphomaS100See panels 1.3,1.4(see lymphomapanels)Pan-Cytokeratin -- Neuroectodermal tumors- Nerve & nevrve sheattumors- Neuroblastoma- Cartilaginous tumors- Lipomatous tumorsSALL-4Oct-4VimentinLeucocyte common antigen(LCA)Pan-CytokeratinEpithelial tumors /Carcinomahistochemical markers have to be interpreted inthe appropriate morphological context.Germ cell tumors(see individualpanels)CD68FascinPan-Cytokeratin - Small cell-, endocrine- &neuroendocrine carcinomas- Myoepithelial tumors- Granulosa cell tumorHMB45Melan ATyrosinaseSOX-10Histiocytic /dendritic celltumors(see panel 1.13)(see individual panels)(see individual panels)- Melanoma- Clear cell sarcomaAlgorithm 1.1 Primary Screening Antibody PanelImmunohistochemistry in Tumor Diagnostics Muin S.A.Tuffaha, Hans Guski, Glen Kristiansen. 2018 Springer
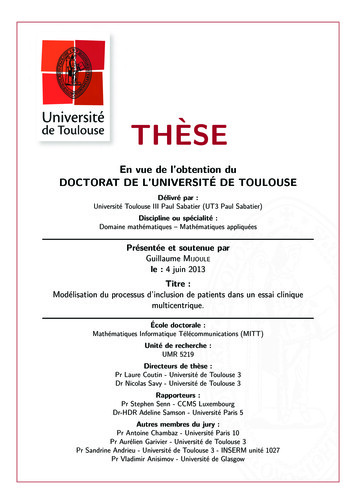
Algorithm 1.5 Carcinomas with Cytokeratin/Vimentin Co-expressionPan-Cytokeratin CK7 / CK20 -/ CK7 /CK20 (see panel 1.7)CK7 - /CK20 CEA -CK7 - /CK20 (see panel 1.8)CEA S100 -CK5/6/13p63CEA UroplakinCEA GATA-3Polyoma virus- Transitional cell carcinoma- Brenner tumorCA 125CDX-2Cadherin-17VillinEndocervical adenocarcinomaPDX-1CA19.9NSEMerkel cell carcinomaCDX-2SATB-2VillinMucinous ovarian carcinomaPancreatobiliary adenocarcinomaColorectal adenocarcinomaGastric adenocarcinomaImmunohistochemistry in Tumor Diagnostics Muin S.A.Tuffaha, Hans Guski, Glen Kristiansen. 2018 SpringerAlgorithm 1.6 CK7/CK20 Expression Pattern in Carcinomas
CK7 /CK20 alcitoninCEA-Salivary gland tumors-Tumors of skin adnexaEstrogen &ProgesteronereceptorsNapsin AMedullary thyroidcarcinomaThyroglobinPAX-8CK 5/6/14p63- PAX-8- CD117PulmoraryadenocarcinomaSalivary glandtumorsSquamous cellcarcinomaThymomaCK19CD15CD56 -Follicular thyroidcarcinomaPapillary thyroid rcinomaBreast carcinomaPAX-8WT-1P16Serous ovarian carcinomaAlgorithm 1.7 Cytokeratin CK7 /CK20 CarcinomaImmunohistochemistry in Tumor Diagnostics Muin S.A.Tuffaha, Hans Guski, Glen Kristiansen. 2018 SpringerPan-Cytokeratin CK7 -/CK20 -
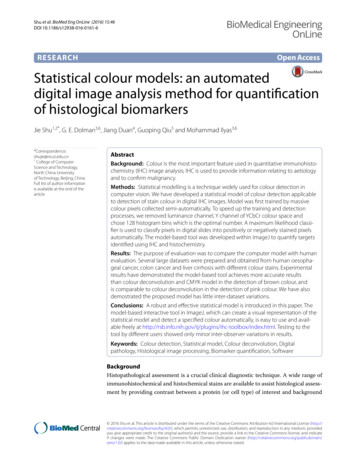
EPITHELIAL TISSUES MARKERS: CYTOKERATINSÄCytokeratins are the most important markers used for thediagnosis of epithelial neoplasms. Cytokeratins are intermediatefilament proteins building an intracytoplasmic network betweenthe nucleus and cell membrane of epithelial cells. Cytokeratinsare a complex family composed of more than 20 isotypes anddivided into 2 types: type I (acidic group) including cytokeratins9–20; type II (basic group) including cytokeratins 1–8ÄMoll’s catalog- it groups the cytokeratins according to theirMW and isoelectric point. Therefore they are subdivided into 3groups: high MW, mean MW and low MW.ÄSimple epithelium: 7-18, 8-18
EPITHELIAL TISSUES MARKERS: CK-LMW785452181920454046CK-HMW Simple epitheliumand glandulartypeDifferent cytokeratins are expressed in different epithelial tissues and at differentstages of differentiation; consequently, different epithelial types of tumors havedifferent specific cytokeratin expression profiles, which usually remain constant afterneoplastic transformation
EPITHELIAL TISSUES MARKERS: CYTOKERATINS-To define the epithelial origin of a neoplasm and characterize it.In IHC sections, cytokeratins reveal typically a diffuse cytoplasmic expression pattern;nevertheless, abnormal staining patterns such as perinuclear and dot-like expressionpatterns are characteristic for different neuroendocrine tumors. No pan-cytokeratin reactsabsolutely with all cytokeratins; nevertheless, cytokeratin cocktails are very effective inscreening for epithelial differentiation or epithelial neoplasmsDifferent Abs: - Broad spectrum cytokeratins (AEl/AE3): Ab cocktail recognizing most epithelialneoplasms. E1 reacts with type I cytokeratins and AE3 with type II cytokeratins. AE1/AE3 is awidely used as pan-cytokeratin marker but lacks the reactivity with cytokeratin 18. Fewepithelial tumors are negative or weakly positive for this cocktail such as hepatocellular andrenal cell carcinoma Positive control: tonsils, appendixPitfallsDifferent cytokeratins are also expressed in various non-epithelial tissue types andneoplasms or in tumors with features of epithelial differentiation. (some soft tissue tumors,melanoma, mesothelioma ) The aberrant expression of cytokeratin in mesenchymaltumors is usually patchy and may show dot-like expression pattern. The diagnosis of carcinoma based only on a positive pan-cytokeratin reaction is one of the sources of seriousmistakes in tumor diagnosis. For appropriate diagnosis, it is always advisable to determinethe cytokeratin profile of the tumor and then to search for other tissue-specific markers.
endometrium,ig. 2.3 Characteristictransitional cellot-like perinuclearFig. 2.3 Characteristicxpression of CK20dot-likeinperinuclearcarcinoma,Merkel cell carcinomaexpression of CK20 inhepatocellularMerkel cell carcinomacarcinoma, renalcell carcinoma,neuroendocrinecarcinomacarcinoma, and less frequently transitional celllung, femalecarcinoma (Fig. 2.4). Also characteristic, is thegenitaltract,dot-like perinuclear stainingpatternin MerkelFig. 2.3 Characteristicdot-like perinuclearexpression of CK20 inMerkel cell carcinomahepatocytes,proximal ls, smoothmuscle cells,myofibroblasts,endothelialcells,arachnoid cellsPositive control: appendixDiagnostic Approach Cytokeratin 18 is a type Icytokeratin, an intermediate filament expressedin simple epithelial cells and found in themajority of non-squamous carcinomas includingadenocarcinoma of unknown origin and neuroendocrine carcinoma in addition to hepatocellularand renal cell carcinoma.Diagnostic Pitfalls It is important to considerig. 2.4 Metastaticthat endothelial cells of lymphatic and smallolorectal adenocarciFig. 2.4 Metastaticoma with strong CK20venous vessels are positive for cytokeratin 18—colorectal adenocarcixpressionnoma with strong CK20expression which can also be a component of different cytoFig. 2.4 Metastaticcolorectal adenocarcikeratin cocktails—thatmight mimic thenoma with strong CK20intravascular tumorexpressionspread. Cytokeratin 18 is alsostanta@impactsnetwork.euexpressed in smoothmuscle cells and smoothstanta@impactsnetwork.eutional epithelium, the expression of cytokeratin20 is restricted to the umbrella cells, whereas carDiagnosticApproachcinomain situ showsa transepithelialCytokeratinexpression19 is a type Icytokeratin and the smallest human cytokeratinfound in both simple and complex epithelium. Itis positive in the majority of carcinomas and hasa limited use in differentiating between carcinoma types.Sorce:Cytokeratin19 strongly labelspapilImmunohistochemistryin TumorEditorsGuski,lary thyroidDiagnostics,carcinomaandTuffaha,can beused inKristiansen. Publisher Springercombination with other markers such as CD56and p63 to differentiate between papillary andfollicular thyroid carcinomas, as the latter is usually negative or very weak positive for cytokeratin 19 (see related chapter) [9].Cytokeratin 20Expression pattern: cytoplasmicMain diagnosticExpression inuseother tumorsMerkel tocellularcarcinoma,transitional cellcarcinomaPositive control: appendixAdenocarcinomaof thegastrointestinaltract, pancreas,and extrahepaticbile duct system,mucinous ovariantumorsExpressionin normalcellsGastric andcolorectalepithelium,umbrellacells oftransitionalepitheliumDiagnostic Approach Cytokeratin 20 is a type
CK5,6, breast cancerCK8, breast cancer
MARKERS FOR MUSCLE CELLS-DESMIN: Desmin stains cardiac, skeletal, and smooth muscle cells andtumors derived from these cells. The intensity of desmin expressioncorrelates with the differentiation grade of muscle or muscle tumor. fferentiation/rhabdomyosarcoma. It is expressed in myofibroblasts, butnot in myoepithelial cells.-Muscular Actin (HHF35): it reacts with both skeletal and smooth muscleactins and accordingly stains both smooth muscle and skeletal muscletumors. It is expressed by myofibroblosts as well as myoepithelial cells.-MYOGENIN (MyoD1): it is a myogenic transcriptional regulatory factor. Ittakes part in the early stages of skeletal muscle differentiation. Maindiagnostic use: Rhabdomyosarcoma.-MIOGLOBIN AND α-SARCOMERIC ACTIN: Rhabdomyosarcoma (skeletalmuscle tumors)-ACTIN for SMOOTH MUSCLE CELLS: Leiomyosarcomas (smooth muscletumors).
cell carcinoma, hepatocellularcarcinoma, gastric adenocarcinoma,skin adnexal tumors, uterine leiomyomaand leiomyosarcomaPositive control: normal breast tissuefallopian tube mucosa, sweatglands, salivary glands, hepatocytes,pituitary glandSTEROID HORMONES RECEPTORSDiagnosticareApproachreceptors (ER)The expressionof estrogen familyreceptors (ER) isEstrogen receptors (ER)a Estrogenmemberof thesteroidofaare a member of the steroid family of ligand- good marker for the majority of breast carcinoligand-dependent transcriptionfactorstypesdependent transcription factorsand include andtwo mas inincludeaddition to tumorstwoof uterine ntorigin.Adequateandrapidtissuefixationwithencoded by two differentgenes on different chromosomes, thechromosomes, the alpha type (ER-α) and beta buffered neutral formalin is required for optimalalpha type (ER-α) andtypebetatype(ER-β).ThestainER-αtypeis mainly(ER-β); eachtype includesdifferent spliceresults. For allsteroid receptors,any atternotherthannuclearmustbeinterpretedasexpressed in both epithelialand stromal cells of the breast, uterus,in different organs and different tissue types [1]. negative. The expression of ER-α type is anplacenta, liver, CNS, Theendothelium,andProgesteroneisanti-aER-α type is mainly expressedin both bone.epi- importantpredictor for the response to thethelial andof the breast, uterus, pla- hormonetherapy (Fig.parenchyma10.1) [2]. Few scoringsteroid hormone involvedinstromalthecellsdifferentiationof breastcenta, liver, CNS, endothelium, and bone, systems were suggested for semiquantitative estiand endometrium in additiontotypemilkwhereas the ER-βis mainlyproteinexpressed in thesynthesis.mation of estrogen Progesteroneand progesterone receptors.prostate, testes, ovary, spleen, thymus, skin, and The modified scoring system suggested in 1987receptors (PgR) are goodmarker for breast carcinomas and haveendocrine glands including thyroid and parathy- by Remmele, the modified scoring system sugroid glands, adrenalglands, and the pancreas.more specificity than estrogenreceptorsas theyareexpressedonlygested in1985 byMcCarty, and the AllredscorAnyway, many tissue types show the expression ing system proved to be the most practical andin a limited number of tumorsas endometrialcarcinoma .of both receptorsuchtypes.simplest systems. The three systems depend onImmunohistochemistry in TumorDiagnostics Muin S.A.Tuffaha, Hans Guski,Glen Kristiansen. 2018 SpringerFig. 10.1 Strongnuclear expressionof estrogen receptorsin breast carcinoma
CELL PROLIFERATION MARKERS-PCNA (Proliferating Cells Nuclear Antigen): it is a DNA polymerase associatedprotein. It is highly expressed in the late G1 phase and during S phase of thecell cycle.-Ki-67 (MIB1): proliferation index – it is expressed in all cell cycle phases,excluded G0.MARKERS OF TUMOR AGGRESSIVENESS-EGFr: Epidermal growth factor receptor-1 (EGFR, Erb1) is a member of type Ireceptor tyrosine kinase family, a transmembrane glycoprotein normallyexpressed on the membrane of various types of normal epithelial and nonepithelial cells. It binds EGF o TGFα. Higher EGRFr expression isassociated to higher tumor aggressiveness.-C-erbB2 (HER2 / neu): Human epidermal growth factor receptor-2 (HER-2).During carcinogenesis, the amplification of the HER-2 occurs, causing theoverexpression of the HER-2 receptor, which is characteristic for few typesof human carcinomas, mainly breast and gastric adenocarcinomas.-P53: p53 mutation is a common event in cancer. Mutations within the TP53cause the overexpression and accumulation of mutated p53 protein not able tobind DNA to stimulate the p21 synthesis acting as a stop signal in the cell cycle,consequently causing an uncontrolled proliferation of involved cells. Theoverexpression of p53 is associated with different neoplastic and preneoplasticlesions.
P53 in HGSO carcinoma
Papillary renal cell carcinoma RCC CA IX Clear cell renal cell carcinoma CD117 Chromophobe renal cell carcinoma Collecting duct carcinoma Arginase Hep Par 1 AFP Glypican-3 Hepatocellular carcinoma Algorithm 1.5 Carcinomas with Cytokeratin/Vimentin Co-expression Pan-Cytokeratin CK7 / CK20 -/ CEA CDX-2 Cadherin-17