Transcription
ReviewReviewAntibody validationJennifer Bordeaux, Allison W. Welsh, Seema Agarwal, Elizabeth Killiam, Maria T. Baquero, Jason A. Hanna,Valsamo K. Anagnostou, and David L. RimmDepartment of Pathology, Yale University School of Medicine, New Haven, CT, USABioTechniques 48:197-209 (March 2010) doi 10.2144/000113382Keywords: antibody; validation; immunohistochemistry; immunofluorescenceAntibodies are among the most frequently used tools in basic science research and in clinical assays, but there are nouniversally accepted guidelines or standardized methods for determining the validity of these reagents. Furthermore,for commercially available antibodies, it is clear that what is on the label does not necessarily correspond to what is inthe tube. To validate an antibody, it must be shown to be specific, selective, and reproducible in the context for whichit is to be used. In this review, we highlight the common pitfalls when working with antibodies, common practices forvalidating antibodies, and levels of commercial antibody validation for seven vendors. Finally, we share our algorithmfor antibody validation for immunohistochemistry and quantitative immunofluorescence.IntroductionAntibodies are among the most commonlyused research tools, routinely used forWestern blot (WB), immunoprecipitation(IP), enzyme-linked immunosorbent assays(ELISA), quantitative immunofluorescence(QIF), and immunohistochemistry (IHC).They are also important tools in clinicalmanagement with extensive use in bothlaboratory medicine (ELISA assays andflow cytometry) and anatomic pathology(IHC). In anatomic pathology, IHC servesas a diagnostic, prognostic, and predictivemethod and IHC readings directly influencethe management of patients in the clinicalsetting. For example, the assessment ofestrogen receptor α (ER-α), and humanepidermal growth factor receptor 2 (HER2)by IHC in breast cancer patients is the definitive test to determine whether or not apatient will receive therapies that can costas much as 100,000 per year. Thus, in theclinic, as well as in the research laboratory,careful accurate validation of antibodyreagents is critical for correct results.The influence of antibody-based testson clinical decisions has led to a numberof publications that have highlightedthe unmet need for standardization ofsuch assays and development of antibodyvalidation guidelines (1–8). Althoughmany groups have enunciated the need,there are no universally accepted guidelines for best practice in antibody-basedtests. There are a number of books onthe topics by world leaders such as CliveVol. 48 No. 3 2010Taylor and David Dabbs, and recently, anad hoc group published a set of “recommendations” (2). However, these worksfocus on the clinical aspects of IHC,often using subjective criteria and oftennot taking advantage of recent scientificadvances that allow more quantitativeevaluation of antibodies. Conversely, thereare other groups that have done biologically rigorous evaluation of antibodiesusing surface plasmon resonance (9) andeven X-ray crystallization of antibodiesbound to their antigens (10), methods thatare unachievable in a routine research orclinical setting. The wide range of rigorand methodology in what is used forvalidation is probably responsible for alack of consensus on a single method forantibody validation. Here we presentan overview of antibody validationapproaches and the pitfalls associated withthe failures of validation. This work specifically focuses on assessment of prognosticand predictive cancer-related biomarkerson formalin-fixed paraffin embedded(FFPE) tissue.What is antibody validation?The FDA defines validation as “the processof demonstrating, through the use of specificlaboratory investigations, that the performance characteristics of an analyticalmethod are suitable for its intendedanalytical use” ulatoryInformation/Guidances/UCM070107.pdf).197For antibodies, one must demonstrate thatthey are specific, selective, and reproduciblein the context for which they are used.When it comes to IHC, standardizationcan be quite challenging due to the numberof pre-analytical, analytical, and postanalytical factors known to influencestaining in FFPE tissue. Variable time tofixation, inadequate fixation period, differences in fixative used, and tissue processingcan all affect tissue antigenicity (5,11).Antibody clone and dilution, antigenretrieval, detection system, and interpretation of results using different cutoff pointsare also important variables that regulateIHC measurements (3,12) (V.K.A., unpublished data). Here we focus on analyticalfactors and highlight the importance ofproper antibody validation, especially forIHC or QIF use.Common pitfalls inantibody studiesNonspecific antibodiesA recent editorial by Michel et al. (13)emphasizes the lack of target specificityfor 49 antibodies against 19 subtypes ofG protein–coupled receptors calling formore stringent antibody validation criteria.Examples highlighted by the authorsincluded double-knockout mice lackingthe M 2 and M 3 subtypes of muscarinicreceptors still staining positive for M2 andM 3 receptor antibodies (14), and tripleknockout mice for the three α1-adrenoceptorwww.BioTechniques.com
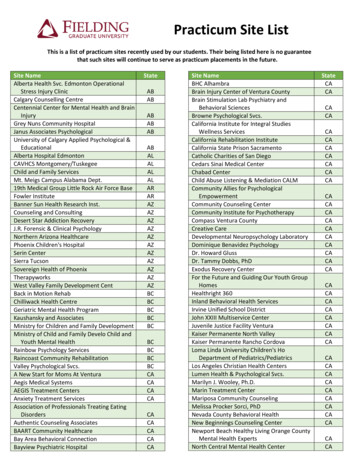
Reviewsubtypes demonstrating staining patternssimilar to wild-type mice (15).Determining the specificity of anantibody is in part dependent on the typeof the immunogens: synthetic peptidesor purified proteins. Synthetic peptidesprovide the advantage of knowingthe amino acid sequence to which theantibody binds; however, these peptidesdo not necessarily recapitulate the 3-Dstructure or post-translational modifications of the native protein (16). As a result,antibodies generated against a syntheticpeptide may not work well when a proteinis in its native conformation with intact3-D structure. Such antibodies may not beuseful for IP or IHC experiments, but maybind the protein of interest after it is fullydenatured when running SDS WB. Theopposite could also be the case, especiallyif the immunogen was the purified protein,where the antibody works well for proteinsin their native conformation, but not whendenatured. Thus WB cannot be an absolutestandardization for antibody binding inIHC or other assays where the antigen isin its native conformation.The native versus denatured confirmation is further complicated by methodsused to fix tissue. Epitopes that are notexposed in the native proteins can beexposed in fixed tissue and vice versa, eventhough they may not be truly denatured.Thus, an antibody could recognize oneepitope in fresh tissue, but when appliedto fixed tissue recognize another epitope(17,18). A representative example is anepitope on BCL-2 (41–54 amino acids) thatis exposed when BCL-2 is present in thecytoplasm but is inaccessible in the nuclearcompartment most likely due to interactionwith other proteins (19). However, whenBCL-2 is phosphorylated at sites close tothe epitope, the epitope becomes available,as seen when the protein is extracted fromcells or denatured by SDS (20).The issue of epitope specificity isfurther complicated by the choice ofmonoclonal versus polyclonal antibodies.Polyclonal antibodies represent a pool ofantibodies against the immunogen andtypically show a higher probability fordetection in a range of different conditions, whereas a monoclonal antibodyis more likely to work in only one set ofconditions. Polyclonal antibodies mightnevertheless contain superior affinityclones. Perhaps the best example of this isthe FDA- approved Herceptest antibodyfrom Dako, which is the industry standardfor HER2 testing in breast cancer (21).Monoclonal antibodies are more pure,since they are produced from singleclones of fused cells producing immuneVol. 48 No. 3 2010ABCDFigure 1. Examples of non-specific antibodies for HoxA1 and phospho-4EBP1. (A) Cell lysates weredenatured and separated by SDS PAGE, transferred to nitrocellulose and blotted with a mousepolyclonal antibody against HoxA1. A band of the expected molecular weight is seen in CaCo2lysate (marked by the arrow). Note the numerous bands in all cell lines at unexpected molecularweights. (B) A representative example of IHC staining on FFPE breast carcinoma tissue for HoxA1.Note the cytoplasmic staining for a nuclear transcription factor. (C) Western blot for phospho-4EBP1. Arrow denotes band at the expected molecular weight; again, all lysates show numerousbands at unexpected molecular weights. (D) A representative example of IHC staining on FFPElung carcinoma tissue for p-4EBP1. Note the predominantly nuclear localization for a proteinexpected to localize to the cytoplasm and nucleus.globulins. However, these clones may begrown in host animals where the ascitesfluid containing the secreted antibody iscollected (16,18); therefore, these antibodypreparations may be contaminated byantibodies other than the monoclonalantibody of interest. A study by Spicer et al.demonstrated that seven of 20 monoclonalantibody preparations (35%) they analyzedhad staining patterns localized to theGolgi cisternae unrelated to the antigenicspecificity of the antibody, and that fiveof these cross-reactive antibodies failedto even stain the antigen of interest (22).Antibody validation efforts in our lab haveshown similar lack of specificity, even inmonoclonal antibodies. Figure 1 providestwo examples of nonspecific antibodiestested in our lab. In Figure 1A, a mousepolyclonal antibody against HoxA1 (B01P;Abnova, Taipei City, Taiwan) was used toprobe lysates from ten cell lines by WB. Theexpected molecular weight is 37 kD and aband of this size was seen in the CaCo2198lysates (denoted by the arrow). All of thelysates show several bands above and belowthis expected molecular weight at a lowersignal level, such that if this antibody werevalidated only against a cell line transfectedto overexpress HoxA1, these bands wouldhave been missed. This level of noise as seenby WB raises concerns about nonspecificity. Figure 1B provides a representativeexample of the staining pattern seen withthis HoxA1 antibody on breast carcinomatissue. The predominately cytoplasmicstaining for a homeobox transcriptionfactor indicates that this antibody shouldnot be used for IHC or IF methods. Figure1C provides an example of a monoclonalantibody for phospho-4EBP1 (rabbit MAb,clone 236B4; Cell Signaling Technology,Beverley, MA, USA) showing a band ofthe expected molecular weight (denoted bythe arrow) as well as numerous additionalbands at higher molecular weights. Figure1D is a representative example of thenuclear staining observed when using thiswww.BioTechniques.com
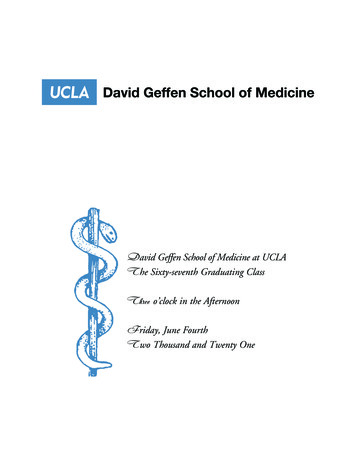
ReviewACBDFigure 2. Lack of reproducibility is seen with the VEGF VG-1 clone antibody. (A) IHC on FFPE lung carcinoma tissue with VG-1 (1:50 dilution) demonstrates specific staining of expected localization. (B)Serial sections of our lung TMA stained with VG-1 (1:50) do not correlate with each other. (C,D) IHCstaining of serial sections of the same patient tissue showing a high level of positivity in Run 1 (C) isnegative for VEGF in Run 2 (D). Inset represents cytokeratin staining of the tumor for reference.antibody for IHC on FFPE lung carcinomatissue when the expected localization forp-4EBP1 is cytoplasmic.Non-reproducible antibodiesPoor correlations between antibody lotsare cause for concern, as demonstrated bya recent study from our lab on antibodiesagainst the Met tyrosine kinase receptor(23). Strikingly, two different lots of themonoclonal 3D4 Met antibody stainedon an array of 688 breast cancer casesshowed opposite staining patterns—onenuclear and one membranous and cytoplasmic—with a regression between the two lotshaving an R 2 value of 0.038 (23). Anotherexample of non-reproducible antibodieswas demonstrated by Grimsey et al. (2008)with antibodies supposedly targeting thecannabinoid CB1 receptor. The authorstested multiple lots of antibodies fromvarious commercial sources by both WBand IF against HEK cells transfectedwith HA-tagged CB1 receptor. Only twoof the six antibodies tested showed specificmembranous staining that co-localizedwith detection using an anti-HA antibody.Additionally, WB analysis on HEK celllysates demonstrated that the antibodieswith poor IF specificity detected proteinsof incorrect molecular weight, no proteinsat all, or proteins present in wild-typeVol. 48 No. 3 2010HEK cells which do not even express theCB1 receptor (24).Some examples of non-reproducibilitycan be very subtle. Figure 2 shows twoexamples of what appears to be specificstaining with expected localization.However, staining with the same conditions on a serial section of the TMA (representing the same patient tissues) showsan extremely poor correlation. VEGF isa secreted growth factor and as such, weexpected cytoplasmic staining on patienttissues with the VG-1 clone (Figure 2A).Staining on a serial section of the sametissue microarray with the same lot ofantibody was not reproducible, with anR 2 value of 0.016 (Figure 2B).Current practice inantibody validationAntibody specificityWB is widely used to determine anantibody’s specificity and is an appropriate first validation step if the antibodyrecognizes the denatured antigen. The firstindication that the antibody is specific forthe selected target would be observing asingle band at the known molecular weightfor the target. Presence of multiple bands orbands not at the proper molecular weight200could represent the same target at differentpost-translational modification status,breakdown products, or splice variants.However, such observations should raiseconcerns for using this antibody for furtherexperiments. Major et al. (2006) publishedtheir database AbMiner as a resource forinformation including the immunogen,vendor, and antigen on over 600 commercially available monoclonal antibodiesthat the group validated via WB againstpooled cell lysates from each of the NCI-60cell lines. An antibody was consideredvalidated if it produced a band (or bands)of the expected molecular weight(s) for thetarget protein (25).While this type of antibody validationis a useful first step, it only guarantees that agiven antibody will provide accurate resultsfor WB analysis. If the goal is to use theantibody for IHC or IF, then the user mustdemonstrate that the antibody is also ableto specifically recognize its target whenused for those applications. Antibodypedia is also an online portal for sharingantibody validation data for WB, IHC,and IF. Only antibodies commerciallyavailable are submitted, and in addition toa validation score, the inclusion of originalexperimental data is required. (26).Antibody specificity has also beenevaluated by using blocking peptidesespecially for IHC (27). These peptidesare the sequences used to generate theantibody and are incubated with theantibody in great excess. The antibody withand without the blocking peptide is thenused to stain tissue known to express thetarget of interest. If the antibody is specific,the addition of the blocking peptide willresult in loss of staining on the tissue.An example using this technique wasrecently published (27) for the validationof phospho-specific antibodies for ERα.Although this method demonstrates thatthe antibody is specific for the immunogenfrom which it was generated, it does notprove selectivity of the antibody sinceoff-target binding activity of the antibodywill also be inhibited by pre-adsorptionwith the blocking peptide. So whileblocking peptides can prove that anantibody is bad, when nonspecific stainingis seen in the presence of the peptide, theycannot prove that an antibody is good.Blocking peptides had been used with anumber of the G protein–coupled receptorantibodies and have been found not to beselective upon more stringent validation(13). Thus, we do not typically includeblocking peptides as part of our antibodyvalidation process.The key to proving antibody specificity is often the correct use of controls.A negative control, including no primarywww.BioTechniques.com
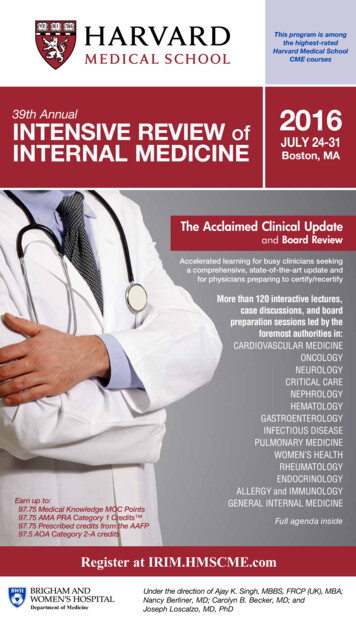
ReviewFigure 3. The Rimm Lab Algorithm for antibody validation of IHC/QIF. Step 1 of antibody validation is using cell lines in vitro to test antibody specificity. Step 2 (below the dotted line) involves further validation of antibody on tissue microarray (TMA) for expected target localization and reproducibility between assay runs and different antibody lots.antibody in an IHC or QIF experiment,is valuable but insufficient. A betternegative control is a cell line or tissuethat is known not to express the proteinof interest. Knockout cells thus providethe best negative controls. Similarly,non-expressing cells, transfected withthe protein of interest, provide the bestpositive controls. Since these reagents areoften beyond the reach of many labs, thereare other approaches that can be used toobtain comparable control results. Oftenthere are readily available cell lines thathave been biologically proven not toexpress a specific protein of interest. Forexample, H1650 cells are PTEN-null andthereby make a good negative control forPTEN antibodies. Similarly, overexpression can be valuable as a positivecontrol. For example, A431 cells overexpress wild-type EGFR and can be used as apositive control for anti-EGFR antibodies.An alternative to knockout cell controls issiRNA or shRNA knockdown controls,as will be discussed with our Rimm LabAlgorithm of antibody validation.Finally, another type of quality controlslide has been developed by Sompuram etal. that couples peptides to glass slides thatmimic the epitope of the native antigen andare therefore specific controls for a givenVol. 48 No. 3 2010monoclonal antibody (28). The drawbackto this type of control is that it only works formonoclonal antibodies, as the antibody mustinteract with a known epitope in order togenerate the appropriate peptide controls.Antibody reproducibilityAn important criterion for validation andstandardization is antibody reproducibility.This means staining of the same antibodyover time with different lots on differentdays, as well as comparison of a newantibody to either a previously validatedantibody or to a second independent meansof measuring the target that would yieldsimilar results (29). There are not manystudies on reproducibility of antibodies,since this is often assumed when using newlots of the same antibody or new aliquotsof an antibody used previously by the samelab. Our lab published one such example ofthis type of evaluation (23), and a similarwork to show assay reproducibility hasbeen done for HER2 by Gustavson andcolleagues (30).A second issue related to reproducibility is when a new reagent is introducedand there is a desire to compare the newantibody to previously validated standards.This sort of study is seen more commonlyin the literature. For example, van der Vegt202et al. compared HER2 IHC staining of283 breast adenocarcinomas on tissuemicroarrays with the 4B5 rabbit monoclonalantibody to the previously established CB11mouse monoclonal antibody. Additionally,both antibodies were also compared toeach other and to the corresponding FISHscores for each case. The authors found nosignificant differences in sensitivity, specificity, or predictive values between the twoantibodies, validating that 4B5 could beused to assess HER2 expression (31). Asecond example by Zafrani et al. comparedantibodies for ER and PR with IHC tobiochemical determination using enzymeimmunoassay and found significant linksbetween the two methods (32). A similarstudy by Sasano et al. validated the useof an aromatase monoclonal antibody bycorrelating the IHC score with biochemicalactivity as determined by product isolationassays (33). Sometimes this is done in anattempt to prove superiority of a new reagent.In those cases, investigators must comparethe reagents in the setting of intended usewith outcome or response to therapy, not theprevious assay, as the criterion standard. Agood example of this is the work of Cheanget al. that showed the ER antibody SP-1 tobe more prognostic and predictive than thecurrent standard 1D5 (34), although thiswww.BioTechniques.com
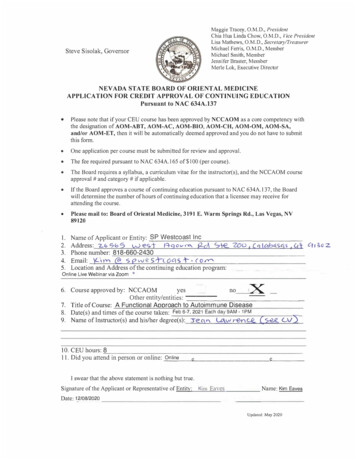
ReviewABFigure 4. Stathmin expression is reduced by siRNA. (A) WB of BT-20 lysates 24 h post-mock;control scrambled siRNA or Stathmin siRNA transfection demonstrates specific reduction inStathmin levels. GAPDH serves as a loading control. (B) BT-20 cells were fixed in 4% PFA 24 hpost-transfection with scrambled control or Stathmin siRNA, and IF with Stathmin demonstratesa reduction in Stathmin expression.conclusion was later disputed by Brock andcolleagues (35).Vendor-based validationof commercial antibodiesIt is estimated that there are over 180antibody companies that produce over350,000 antibodies for the researchand clinical markets (www.antibodyresource.com/onlinecomp.html). So it isnot surprising that there are commercially available antibodies against a hugecollection of target proteins. When onebuys a kit to isolate DNA, it is generallysafe to assume it will not end up purifyingprotein. However, the same is not true forantibodies. Just because the manufacturerclaims an antibody is specific for proteinZ does not necessarily mean that it willonly bind protein Z and not a range ofother proteins (29,36). In 2005, RamosVara noted that the information aboutantibodies targeting the same antigenvaried significantly depending on themanufacturer (16). In fact, it is now clearthat the responsibility for proof of specificity is with the purchaser, not the vendor.Different vendors provide different levelsof validation, depending on their approachto the balance between making a profit andproviding high quality. For this review, wesought to compare the level of validationand amount of information provided byseven different companies (referred toherein simply as Companies 1–7) to therandomly selected molecule AMPKβ1.The companies are not revealed sinceonly 7 of over 180 were chosen at random;furthermore, the level of validation atsome companies varies based on theproduct. When available, we comparedthe validation protocol on the datasheetfor phospho-specific antibodies, as theserequire another level of specificity andvalidation (37,38).In general, we found three levelsof validation. The least validation wasVol. 48 No. 3 2010observed for Company 1’s phosphoAMPKβ1 polyclonal antibody. No information was readily available on its website or datasheet describing any level ofantibody validation criteria. The datasheetitself contained minimal information aboutthe antibody including a brief backgroundon the target with corresponding references, recommended applications andstarting dilutions for WB, IF, and ELISA.However, no examples of successful use inany of these applications are provided andnone of the references provided had utilizedthis antibody. The datasheet also includesthe animal host and immunogen source as asynthetic peptide, but does not include exactpeptide sequence, although the peptide isavailable for purchase for use as a blockingpeptide. The datasheet also cautions thatthis antibody “may” cross-react with correspondingly phosphorylated AMPK β2 .A moderate level of validation wasobserved for Companies 2–5. Thesecompanies also did not provide any in-depthdescriptions of antibody validation procedures. Datasheets all included backgroundon the target, as well as information on theimmunogen. Three out of four companiesincluded the complete sequence usedand the fourth identified the regionsurrounding the phosphorylation siteas the sequence used. These companiesalso provided recommended applicationswith starting dilutions, and all providedat least one example of the antibodysuccessfully identifying its target in oneof the recommended applications. WBs—either with transfected cells expressing thetarget or pre-incubation of the antibodywith blocking peptide—were the mostcommonly shown antibody validationexamples.The highest levels of validation wereseen for Companies 6 and 7. Company6 describes its validation procedures forphospho-specific antibodies to includeWB analysis in (i) multiple cell lines, (ii)peptide and phospho-peptide competition experiments, and (iii) analysis of204site-directed mutants. It also strived todemonstrate lot-to-lot consistency aidedby combination of two or more pre-qualified individual lots to create each batchto minimize batch-to-batch variability.Company 7 describes their stringentvalidation protocol for all antibodies toinclude testing of each antibody by WB,IP, IHC, IF, flow cytometry, and ELISA. Itverifies the specificity and reproducibilityof antibodies by using appropriate kinasespecific activators or inhibitors whenavailable; testing against a large panel ofcell lines with known target expression;phosphatase treatment for phospho-specificity; comparison to isotype control;verification in transfected cells, knockoutcells, and siRNA-treated cells; utilizingblocking peptides to eliminate all signal;verifying correct subcellular localizationor treatment-induced translocation;comparing new antibody lots to previouslots; providing optimal dilutions andbuffers, as well as specifying both positiveand negative control cell lines. For IHC,Company 7’s antibodies are tested onparaffin-embedded cell pellets includingcell pellets created after the cell lines aresubjected to treatments known to inducesignaling changes or treated with siRNAto block expression of the target. Tissue istreated with phosphatase to additionallytest phospho-specificity on FFPE tissues.Xenografts with cell lines of known targetexpression or treatments to modulateexpression are paraffin-embedded andthen stained.The datasheets for these companiesinclude everything seen with Companies2–5 plus additional examples of thesuccessful use of their antibody. Forexample, Company 6 includes representative data for all validated applicationswith recommended antibody concentrations and includes flow cytometry,immunocytochemistry on a positive controlcell line (including incubation with eitherthe phospho-peptide or the non–phosphopeptide demonstrating signal absenceonly with the phospho-peptide), IHCof a positive control tissue, and a WBof a positive control cell line lysate alsoincluding detection after pre-incubationwith the phospho- or non–phosphospecific peptides demonstrating a singleband of the expected molecular weightwith signal absent only after incubationwith the phospho-specific peptide.Antibodies purchased from Company1 (which provided the minimal amount ofinformation and no examples of successfuluse of the product) would require extensivevalidation by a researcher to demonstratethat the results describe only the targetwww.BioTechniques.com
Reviewof interest; the company provides little inthe way of assurances that it will work.Companies 2–5 all provide more information on their respective antibodies andinclude at least one example of the productsuccessfully being used for at least one oftheir recommended applications withcorresponding positive controls. Whilethis is clearly preferable to Company 1’sapproach, these antibodies would stillneed to be validated by the researcherfor target specificity in the application ofinterest and for lot-to-lot reproducibility.Company 6 describes the validation steps ituses to determine that its phospho-specificantibodies are both specific and reproducible.Furthermore, for each recommendedapplication, an example of successful useis provided with corresponding inhibitionby phospho-specific blocking peptides.Company 7 provides what we considerthe gold standard for antibody validation.The extensive in-house testing describedprovides a high level of confidence that theantibodies it provides will work for all theapplications that are recommended for theparticular antibody. It also provides a greaterlevel of confidence that results obtained willbe specific for the described target and willbe reproducible among antibody lots.Even though Companies 6 and 7 provideextensive validation, the researcher is stillobliged to confirm that the product givesspecific and reproducible results in the celllines or tissues of interest in the lab. Indeed,even the best companies cannot control whathappens after the product leaves their door.Issues during shipping, inappropriate storageon or after arrival in the laboratory, andantibody contamination during usage are allpotential sources of error in antibody-basedtesting. Thus vigilant and comprehensivecontrols should be done with each assay.The Rimm LabAlgorithm for antibodyvalidation for IHC/QIFThere are no uniform or enforceablestandards for antibody validation. Unlikedrugs—whose sale is prohibited withoutFDA approval—there is no federalagency governing what can be sold intothe antibody-based assay market. In thefuture, we may see further FDA clearanceof antibodies or more rigorous labelingand regulation of reagents to be used inclinical testing. However, to date, thereis no universal standard. We thereforepresent our lab’s approach (the Rimm LabAlgorithm) to the validation issue. Ourapproach is not sanctioned or approvedby any governing body or by any tradeVol. 48 No. 3 2010ACBFigure 5. ER-α antibody Clone 1D5 as an example of strong correlation between quantitative WB andIHC methods. (A) FFPE MCF7 cells stained with 1D5 (1:50 dilution) demonstrate expected nuclearlocalization for ER-α. (B) WB with 1D5 of a panel of breast cancer cell lines demonstrating varyingexpression of ER-a. Puro cells are MCF7 cells stably expressing an inducible ER-α. β-tubulin servesas a loading control. (C) ER-α expression by WB was quantified using ImageJ and correlated toAQUA scores corresponding to the cell lysates demonstrating a strong correlation.association, and thus we are not so bold asto call this a “recommendation.” Instead,we provide what we feel is a compromisebetween rigor and lab economics thatresults in a level of evidence sufficient fordata dissemination. Our algorithm forantibody validation (Figure 3) is especiallyfocused for the end u
flow cytometry) and anatomic pathology (IHC). In anatomic pathology, IHC serves as a diagnostic, prognostic, and predictive method and IHC readings directly influence the management of patients in the clinical setting. For example, the assessment of estrogen receptor α (E