Transcription
THE BRAIN INJURY BOOKA GUIDE FOR PATIENTS AND THEIR FAMILIESCreated by the Patient and Family Education Working Group, CalgaryBrain Injury Strategy, 2012A Very Special ThanksTo the Glenrose Rehabilitation Hospital in Edmonton, Albertafor their permission to adapt their booklet:―Coping with Brain Injury‖Also,To the survivors, family members and care providers, themembers of the ―Patient and Family Education‖ working groupof the Calgary Brain Injury Strategy, who put this book together.
COPING WITH BRAIN INJURY 2IntroductionKey Messages Brain injury affects virtually every area of a person‘slife. The relationships, roles, and responsibilities of friendsand family will experience a period of adjustment. It is crucial for family members and close ones tomaintain strong support for each other as well as forthe injured person throughout these changes. Adjustments are best made in small steps with theinstruction and guidance of health care team members.Brain injury is a life-altering event which affects every area ofa person‘s life — including his or her relationship with familymembers and others close to him or her. The phraseacquired brain injury refers to medical conditions that occurto the brain (usually after childhood), changing its function.These conditions include stroke, traumatic brain injury, tumorand other diseases of the brain.It is virtually impossible to give an early prediction of the finaloutcome after a significant brain injury. The after effects ofbrain injury can be cognitive, psychosocial (psychological,emotional, and social) and physical. Often there is no clearrelationship between how much disability is experienced by theinjured person and the visible, physical damage. This can leadto misunderstanding by the family members and friends.Sometimes there is the belief that if the injured person justtried harder, he or she could get better. Another common beliefis that because the person looks alright physically, everythingelse should be okay.Family members and others close to a person with braininjury may struggle to cope with behavioural changescaused by the brain injury. It is common for family membersto experience a number of feelings as a result of the injury —shock, numbness, fear, anger, anxiety, depression or guilt. Ifthe injury is serious and the injured person‘s disabilities lead toa significantly reduced quality of life, family members may findthemselves thinking that given the choice, the injured personmay have chosen not to survive the injury.As a result of the brain injury, roles and responsibilitiesoften change within the family. Family members and othersclose to the person may feel stressed, burdened, evendepressed by the major changes in activities,responsibilities, daily schedules, leisure and support thatare required to adjust to the consequences of acquiredbrain injury.Most people with brain injuries are able to go home afterrehabilitation. At this time, family members may find that theyhave to do many of the tasks that were once done by theinjured person. Long term dependence on family members islikely if there is prolonged social, vocational or cognitivedisability.This immense adjustment can‘t be done alone, so it becomesvery important to enlist the support of family, friends andcommunity resources. It is important for the family members tolook after themselves and their own needs by using personalsupport contacts, professional support, social service agenciesor help through a church affiliation. People need to have usefulsupport while developing new resources to cope with all thechanging circumstances in their lives.For any person who was independent, active in thecommunity, participated in sports or hobbies, held a job, or
COPING WITH BRAIN INJURY 3had frequent contact with friends - the loss of any of theseactivities due to the injury can be very difficult to accept. Oftenthe injured person feels useless and depressed. The familybecomes his greatest source of support. This support isparticularly important during the rehabilitation process.professionals. Chapter 1 lists these professionals with a briefdescription of what they do.For the injured person, it is sometimes hard to accept thatthere may be significant and lasting changes. The seriouslyinjured person may not have the insight to see himself ashaving any limitations. Because the outcome of significantbrain injury is often uncertain, the family may have unrealisticexpectations for recovery. Whatever the situation, adjusting tothe changes can be stressful.Understanding how the brain functions is one of the first stepsin putting brain injury into context. Chapter 3 specificallyexamines the structure, functions, and areas of the humanbrain.Often, major adjustments are best made in small steps. Simplechanges may help the person with brain injury, family andfriends to find more enjoyment in their relationships andactivities. By taking each stressful situation one step at a time,the person with brain injury and family may feel that life isbecoming a little more ―normal‖ again.Recovery from brain injury is a process that takes time. Inrecent years, brain rehabilitation as a specialty has advancedin its understanding of ways to encourage and maximizerecovery. Your team will use all available knowledge andtechniques while caring for your loved one. Consult anymember of the health care team to address your concerns andquestions.This book is dedicated to family members who are caring for aperson who has a brain injury. The Brain Injury ResourceBook clarifies and hopefully starts to answer some questionscaregivers must face.Throughout the rehabilitation process, the injured person andthe family will meet with a number of health careChapter 2 describes the recovery process and what the familyshould expect for treatment.Step- by- step, Chapters 4 to 8 walk the reader through all ofthe major problems and disabilities that can occur because ofa brain injury.Chapter 5 is devoted solely to studying various types ofseizures and how caregivers can watch for situations that cantrigger seizures.Chapter 9 addresses social and emotional issues.Life after brain injury can be a struggle for both the injuredperson and their family. Chapter 10 serves as a guide formaintaining and improving the injured person‘s quality of life.Please note the Resource section towards the end of thebook. Finding support, networking, and asking questions arenecessary tasks when one is caring for a person with a braininjury. Although there are few local services in some regions,this section does cover some critical resources that areavailable.For ease of writing and to avoid the awkwardness of he/she,we have used male pronouns throughout the book. This wasdone for ease, not to imply any gender bias.
COPING WITH BRAIN INJURY 42. A Team ApproachKey Messages The health care team is dedicated to helping aperson following brain injury and their family. Patients, families and friends are importantmembers of the team, because they are the trueexperts.The health care team is an important source of informationand support to the injured person and family. The team canrecommend a treatment plan and help to learn skills to meetspecific needs.Family, friends and the person with brain injury areimportant members of the health care team. Activeparticipation in treatment and rehabilitation is essential torecovery. The involvement of other family members,caregivers, friends and co-workers also can help the personwith brain injury successfully return home and to thecommunity.Health care team members may include: A primary care physicianThe doctor is responsible for medical care and treatment.The attending doctor may have residents, fellows, and clerksworking with him or her, making up your ―team‖ of doctors. Nurse practitionerA nurse practitioner (NP) is an advanced practice nurse whoworks with the physician team. They are able to assess andtreat, including ordering tests and investigations andprescribing medications. The NP works closely with thenurses and therapists and are often the ―eyes and ears‖ forthe physicians. PhysiatristThese are physicians who specialize in physical medicineand rehabilitation, including brain injury rehabilitation. NursesNurses have training and expertise in brain injury care,rehabilitation and discharge planning. The nurse monitors aperson‘s vital signs and neurological status and performsassessments and interventions. The nurse also assists withdaily care such as taking medications, bathing, dressing andusing the toilet. Through rehabilitation, they help a persondo the things learned in therapy, to increase theirindependence while in the hospital and prepare fordischarge and reintegration into the community. Psychologists and NeuropsychologistsThese are professionals with training and expertise inevaluating and treating thinking, behavioral and emotionalchanges caused by a brain injury. PhysiotherapistsThey are professionals who evaluate and treat changes inphysical abilities. Some activities may includestrengthening, conditioning, walking, and balance training.
COPING WITH BRAIN INJURY 5 Occupational therapistsThey are professionals who evaluate and treat thinking andperception problems, and help an injured person maintainor learn independent living skills (for example: eating,dressing, managing money and safety awareness). Recreation therapistsThese are professionals who help a person with brain injuryexplore and participate in leisure activities. They help tofind new leisure opportunities and learn new ways to dopreviously enjoyed activities. Brain injury coordinators and case managersThese are nurses and therapists who help coordinate careof patients with brain injury and support and educate theirfamilies about the injury and recovery process. Social workersThese are professionals in the hospital and outpatientsettings who help guide the adjustment to acquired braininjury. They provide information on discharge planning,assessment of financial resources, and community resourcereferrals. They may also assist in addressing stressmanagement and the development of effective coping andadjustment strategies.DieticianMakes sure nutritional needs are met. They provide nutritionteaching in the hospital and will also help make food choicesat home. Speech language pathologists or speechtherapistsThese are professionals who evaluate and treatcommunication and swallowing problems. They focus onimproving social skills as well, and look at cognition as itrelates to communication. Transition coordinator or home care coordinatorNurses who provide information about home care servicesand other options for supported living. Help may be availablefor activities of daily living, to assist with rehabilitation andgoals to maintain or increase independence and forsurveillance. A home care therapist may make a home visitprior to discharge from the hospital to identify and organizeany equipment or changes in the home that will make it saferand easier. The survivor, family and friendsThis is who makes decisions about a person‘s care andrehabilitation including their goals and plans. Family andfriends can speak for the survivor if they are not able tospeak for themselves about their goals and plans andfeelings and beliefs. Family and friends can give emotionalsupport and can help practice new skills and techniques tohelp meet the survivor‘s needs.The healthcare team meets regularly to discuss healing,progress and make ongoing plans. In addition to regular,informal updates, a family conference can be scheduled tobring everyone together. If you have concerns, speak withany member of the team.
COPING WITH BRAIN INJURY 62. The Recovery Processflow and chemical systems to recover will usually lead toimproved function.Key MessagesIn cases of traumatic brain injury, trauma often occurs toother parts of the body, with associated bleeding, swellingand changes in function. The effects of these other injuriescan prolong overall recovery and maybe even furtherdamage the brain. For instance, excessive bleeding maydeprive the brain of needed blood and oxygen. Prompttreatment of associated injuries may help limit braindamage. Recovery from a brain injury is a process that takestime. Various treatment options and coping strategies canhelp life gradually feel ―normal‖ again. The medical community is gradually realizing howa damaged brain recovers. Current treatmentmethods are based on a growing understanding ofthe brain‘s recovery processes Most adults with a brain injury progress throughcommon recovery stages. The length and outcome of each stage cannot bepredicted. During recovery, a person may shift back and forthbetween stages; Inconsistency is commonRecovery following a brain injury may be measured inweeks, months or years, and slows with the passage oftime. Some of the effects of brain injury can be long-lastingand recovery may be incomplete. Although some peoplewith severe brain injuries experience only mild long-termdifficulties, others may require care or special services forthe rest of their lives.In the days and weeks immediately following brain injury,the function of surviving brain tissue is often affected byswelling, bleeding and/or changes in the brain‘s complexchemistry. Sometimes blood accumulation must be removedsurgically to reduce swelling and pressure within the brain.Controlling swelling and allowing time for the brain‘s bloodIn the first few weeks after a brain injury, swelling, bleedingor changes in brain chemistry often affect the function ofhealthy brain tissue. The injured person‘s eyes may remainclosed, and the person may not show signs of awareness. Asswelling decreases and blood flow and brain chemistryimprove, brain function usually improves. With time, theperson‘s eyes may open, sleep-wake cycles may begin, andthe injured person may follow commands, respond to familymembers, and speak.A period of confusion and disorientation often follows,during which the person‘s ability to pay attention and learnstops and agitation, nervousness, restlessness or frustrationmay appear. Sleeping patterns may be disrupted.Overreaction to stimulation and physical aggression mayresult. This stage can be disturbing for family because theperson behaves so uncharacteristically.Inconsistent behaviour also is common. Some days arebetter than others. For example, a person may begin tofollow a command (lift your leg, squeeze my finger) andthen not demonstrate this behaviour again for a time. Thisstage of recovery may last days or even weeks for some.However, once demonstrated, behaviour usually appearsagain. In this stage of recovery, try not to become anxious
COPING WITH BRAIN INJURY 7about inconsistent signs of progress. Ups and downs arenormal. A broad range of therapy, testing, and othertreatment options are available to help people aftera brain injury.Family and friends can help by creating a calm, quietenvironment (for example, limiting the number of people inthe person‘s room, turning off the television and dimmingthe lights). In addition, ask questions of the nurses andothers on the health care team, who are responsible forkeeping you accurately informed. You are encouraged toask questions to stay abreast of your loved one‘s progress. Treatment for brain injury is tailored to meet individualneeds. Members of the health care team determine when therehabilitation process will begin.Exactly what happens in the brain during the later stages ofrecovery is not clear, but some parts in the process arebecoming clearer. New research is shedding light on braintissue and its capacity to repair itself. Many things canoccur that help restore surviving brain tissue to maximizefunction. For example, although the total number of braincells may not change, it is thought that surviving braintissue has the capacity gradually to learn how to performsome functions of destroyed cells.Later stages of recovery can bring increased brain function.The person‘s ability to respond may improve gradually. Newresearch is investigating the body‘s ability to replacedamaged brain tissue. Other parts of the brain, however,may slowly learn to assume functions of the damagedtissue.Factors such as age and the severity and location of a braininjury can affect, but do not entirely predict, the outcome ofrecovery. For example, some people with significant braininjuries experience only mild long-term difficulties, whileothers need lifelong, special care.Treatment of Brain InjuryKey MessagesDepending on the nature of the brain injury, somepeople begin treatment in an intensive care unit (ICU) ora general hospital unit, and may be transferred later to arehabilitation unit. After they leave the hospital, therapyas an outpatient may continue. Some need regularfollow-up appointments with a health care provider whilesome will receive therapy, tests and monitoring on anoutpatient basis.During the early weeks after injury, treatment focuses onstabilizing the person‘s physical condition, preventingcomplications such as pneumonia and blood clots, andaddressing medical issues that arise (for example,removing blood or other fluid build up to reduce swellingand pressure in the brain).When the health care team determines that the personwith brain injury is ready, the rehabilitation process canbegin. Rehabilitation encourages the body‘s naturalhealing process through: Stimulating and enhancing physical and thinkingabilities.Teaching new techniques to compensate for lostphysical, thinking (cognitive) and behaviouralskills.
COPING WITH BRAIN INJURY 8Early on, therapy strives to keep the person safe andincrease awareness of his or her surroundings. Forexample, the health care team may need to help theperson relearn date, time and location and understandwhat happened with the injury.As cognitive and physical abilities progress, the focusshifts to improving attention span and mobility, copingwith memory and thinking problems and increasingindependence in self-care skills. The person mayparticipate in stretching, strengthening, balance andrange of motion exercises. Community outings topractice skills learned in the hospital may be included.How much and what rehabilitation therapy the personwith brain injury receives depends on factors such aslevel of awareness, other injuries such as fractures, theneed for rest, and the ability to participate in therapy.If you have concerns about your loved one‘s thinking,behaviour or emotions, even years after a brain injury,contact a member of the brain rehabilitation teamThe family’s role in therapyWhat is the role of family and friends in the recovery of thebrain injury survivor? The key to relearning more normalmovement is practice. The injured person spends only a smallportion of their day in therapy. What happens during the rest ofthe day affects recovery. Therapists may have specific adviceabout exercises or activities that can be done with the injuredperson on the ward and at home. The safest and easiestmethods of doing transfers are a good example of this.―Transfers‖ refer to moving from a chair or wheelchair toanother seat, such as a bed, toilet, bathtub or car. Family andfriends can also learn to assist the person when he is walking,managing on stairs and mobilizing in his wheelchair. The goalis always to enable the person to be as independent aspossible while ensuring the safety of themselves and thehelper(s).There is no ―normal‖ or ―standard‖ way of moving. How we dothings depends on our age, body build, habits and pre- existingmedical and physical well-being. It is important to keep in mindthat each brain injury is unique and, therefore, expectedoutcomes are specific to the brain injury survivor.When friends and family members are aware of treatmentgoals and activities, they become partners with the patient andthe rehabilitation team in optimizing the rehabilitation process.
COPING WITH BRAIN INJURY 93. The BrainStructureThe brain is the body‘s control centre. It is made up of billions ofnerve cells, called neurons, which are arranged in patternsthat work together to control thought, emotion, behaviour,movement and sensation. For example, how we think, feel,see, taste, touch, move, control our breathing, heart rate andregulate blood pressure.Each neuron gives off chemicals that trigger an action in otherneurons. These chemicals are called neurotransmitters andare substances like epinephrine, norepinephrine, or dopamine.Each cell can send a message to other cells. The speed of themessage varies depending on the path to the cell and theconnections between them.How well the brain is working depends on:- How well each part of the brain is working- How well the connections are working- How quickly the messages are sent between theconnections of the cellsInformation goes through many nerves which connect tocertain parts of the brain. One major route from the brain tothe rest of your body is through the spinal cord. Messagessent to your brain tells it about things such as hot and cold,pressure, pain, and where arms and legs are positioned.Other nerves carry information from the eyes, ears, tongueand muscles on the face to the brain. These are called cranialnerves. The brain then sends messages to the musclesthrough a different set of nerves so a person can do things likemove, walk, talk and swallow.The brain is covered by three membranes (skin like layers).These are called the dura, arachnoid and pia mater. The brainand spinal cord sits in a clear fluid that bathes the brain andcirculates into the ventricles of the brain. This is called thecerebrospinal fluid or CSF.Several major arteries supply the brain with oxygen and othernutrients. The two vertebral arteries follow the spinal columnup into the brain. The two carotid arteries come up on eitherside of the throat. These four major arteries branch and join toform a network that carries oxygen, nutrients, and blood to theentire brain.The brain is divided into two halves that look nearly the samebut differ in many functions. The halves are called thecerebral hemispheres. For most people, the left half of thebrain controls verbal functions including language, thoughtand memory involving words. The right half controls nonverbalfunction like recognizing the differences in visual patterns anddesigns, reading maps and enjoying music. The righthemisphere also is involved in expressing and understandingemotions.Although each half of the brain has distinct functions, the twoparts actually work closely together to control the activity ofthe body. The left side of the brain controls movement andsensation in the right side of the body and the right side of thebrain controls movement and sensation in the left side. Thus,damage to the right side of the brain may cause movementproblems or weakness on the body‘s left side.
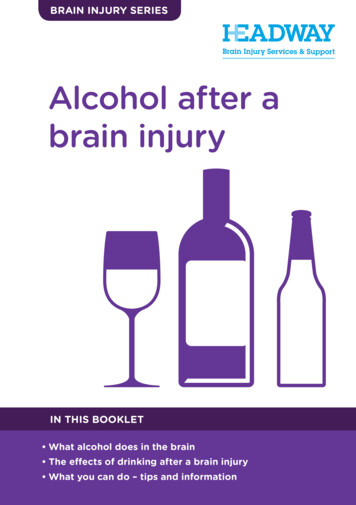
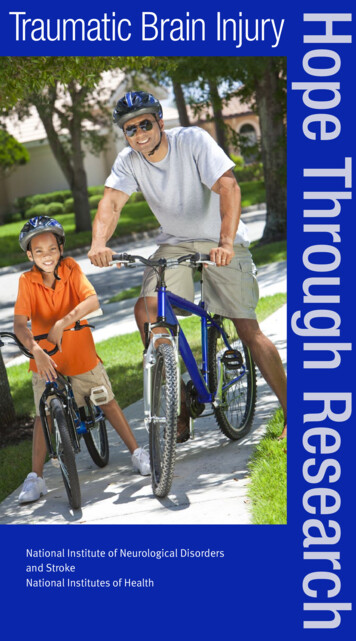
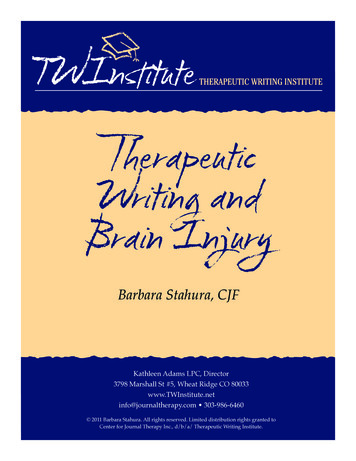
COPING WITH BRAIN INJURY 10Left SideListening, reading,speaking and writingMemory for spoken andwritten messagesDetailed analysis ofinformationControls the RIGHT side ofthe bodyReceives sensation signalsfrom the RIGHT side of thebody and spaceRight SideJudging the position of thingsin space and knowing bodyposition in spaceUnderstanding andremembering things we doand seePutting bits of informationtogether to make up an entirepictureControls the LEFT side of thebodyReceives sensation signalsfrom the LEFT side of thebody and spaceAreas of the brain and results of damageThe cerebral hemispheres are further divided into four separateareas called lobes. Each lobe has different functions. Damageto different parts of the brain can cause different problems. Thespecific nature of the problem or problems depends on whichpart of the brain is injured.Occipital LobeDamage to the left occipital lobe may cause problems in seeingthings on the right side of space. Damage to the right occipitallobe may cause problems seeing things on the left side ofspace.Parietal lobesDamage to the left parietal lobe may lead to problems inreading and arithmetic. As well, damage to this lobe may causea loss of sensation on the right side of the body. This meansthat the injured person has alterations of touch, pain, vision ortemperature changes on his right side. Damage to the rightparietal lobe may lead to problems with spatial tasks, likemaking sense out of pictures, diagrams and reading maps.Damage to the right lobe may cause alteration of sensation onthe left side.Frontal lobesDamage to either frontal lobe may lead to problems withemotional control, social skills, judgment, planning andorganization. Damage to the left frontal lobe may causeproblems in speech and in moving the right arm or leg.Damage to the right frontal lobe may cause problems in movingthe left arm or leg.Temporal LobesDamage to the left temporal lobe may cause problems inunderstanding and remembering language. Damage to theright temporal lobe may cause problems in understanding andremembering non-verbal information such as pictures,diagrams, body language cues, and other visual messages.Brain stemDamage to the brain stem may cause a wide variety of physicaland sensory problems. The brain stem is the control centre forbreathing and for the heart beat. It gives commands to themuscles of the face, eyes, mouth, and throat. Damage to thispart of the brain may also result in the injured person not beingable to swallow food.CerebellumDamage to the cerebellum may lead to problems incoordination, balance or muscle tone of various body parts.No two people will be affected in exactly the same way by abrain injury. This is partly because we are all unique andrespond differently. Another reason is our nervous system iscomplex and it‘s not yet possible to completely predict what will
COPING WITH BRAIN INJURY 11happen as a result of a brain injury, even when we know whatpart of the brain is damaged. ParietalLobeFrontalLobeOccipitalLobeTemporal LobeBrainStemCerebellumTypes of Acquired Brain InjuriesAcquired brain injury, or ABI, is an injury to the brain that doesnot occur at birth. It does not include disease processes that areprogressive. ABI can be a traumatic brain injury, by causessuch as a motor vehicle collision, fall or assault.ABI can also be non-traumatic, where the brain is injured froman anoxia and metabolic/toxic encephalopathy, infectionssuch as encephalitis or meningitis, brain tumors, oraneurysms, vascular malformations or stroke. Encephalitis: potentially life-threatening infection/inflammation of the brainMeningitis: an infection and inflammation of thecentral nervous system that affects the membranesand cerebrospinal fluid surrounding the brain andspinal cordMetabolic/toxic encephalopathy: encephalopathy, orabnormal brain function, is caused by abnormalities ofthe water, electrolytes and other chemicals thatadversely affect brain function. For example, inaddition to liver and kidney waste products, it may bebecause of abnormally high or low blood sugar levels.Toxic changes caused by poisons such as carbonmonoxide, alcohol or drugs can also cause braininjury.Just like if you hit your thumb with a hammer, it will swell up,swelling in your brain can happen as a normal response to aninjury (trauma) or irritation (non-trauma). This is called cerebraledema.There is a balance of brain, cerebrospinal fluid and blood withinthe vessels of the brain. The skull is a fixed compartment, soany increase in either brain size, or the amount of blood or CSFputs pressure inside the skull which can be dangerous.Pressure on the brain tissue reduces blood supply, andtherefore oxygen and causes damage to the cells.A brain tumor, an abnormal growth of cells within the braintissue can be either low-grade, meaning slow growing, or highgrade, or fast growing. These abnormal cells can originate inthe brain (primary) or come from other areas of the body(metastasis). As this growth gets larger, it occupies space inthe skull, pushes on the brain, causes swelling and interfereswith blood and oxygen supply to healthy brain tissue.
COPING WITH BRAIN INJURY 12Anything that hampers blood and oxygen from reaching thebrain for over 2 to 4 minutes can cause brain damage. Forexample, drowning, choking, cardiac arrest and hanging canrestrict blood and oxygen from travelling to the brain. This isreferred to as anoxia, or the state where brain cells aredeprived of oxygen.Strokes are the best known results of circulation problems andstrokes can cause brain damage. Strokes are caused by aninterruption of the blood supply to part of the brain. Forexample, an artery may be blocked by a floating blood clot(embolism), or may become too narrow for blood to flowthrough it (thrombosis, or hardening of the arteries).Occasionally an artery wall has a weak section (aneurysm)which balloons out under the pressure of blood flow. This weaksection may burst or leak, causing bleeding inside the brain(intracerebral hemorrhage). Surgery is often needed to clip offthe aneurysm and remove the blood. An abnormal tangle ofblood vessels (arterio-venous malformation) can causedamage similar to an aneurysm.Traumatic brain injuries that affect the brain but don‘tpenetrate the skull are called closed head injuries. The skullmay not seem damaged even when there is considerabledamage to the brain. This is usually the result of the headhitting an object, or vice versa. The brain may hit the skull atthe point of impact, then bounce against the other side of theskull, and rotate at a high speed.Whenever the brain is violently shaken or rotated there is ashearing or tearing of tissue. If blood vessels are broken,bleeding may continue until a pool of blood (hematoma) buildsup, causing pressure on the brain. An epidural hematoma isblood between the dura and the skull. A subdural hematomais bleeding below the dura layer. A subarachnoid hematomarefers to bleeding under the arachnoid layer of the brain. Anintracerebral hemmhorage refers to bleeding inside the brain.An intraventricular hemmhorage is bleeding within theventricles.When the brain move
changes may help the person with brain injury, family and friends to find more enjoyment in their relationships and activities. By taking each stressful situation one step at a time, the person with brain injury and family may feel that life is becoming a little more ―normal‖ again. Recovery from brain injury is a process that takes time. In