Transcription
Treating Substance Use Disordersin Brain Injury SurvivorsPresented by:Christine (Brenton) Boucher LPC, LADC, CBISJanuary 27, 2016
Treating Substance Use Disordersin Brain Injury SurvivorsPresented by:Christine (Brenton) Boucher LPC, LADC, CBISJanuary 27, 2016
Thomas Durham, PhDDirector of TrainingNAADAC, the Association for Addiction Professionalswww.naadac.orgtdurham@naadac.org
Produced ByNAADAC, the Association for Addiction Professionalswww.naadac.org/webinars
www.naadac.org/webinars
www.naadac.org/braininjurysurvivors
Cost to Watch:FreeCE HoursAvailable:1.5 CEsCE Certificate forNAADACMembers:FreeCE Certificate forNon-members: 20CE CertificateTo obtain a CE Certificate for the time you spentwatching this webinar:1.Watch this entire webinar.2.Pass the online CE quiz, which is posted atwww.naadac.org/braininjurysurvivors3.If applicable, submit payment for CE certificateor join NAADAC.4.A CE certificate will be emailed to you within 21days of submitting the quiz.
Using GoToWebinar – (Live Participants Only) Control Panel Asking Questions Audio (phone preferred) Polling Questions
Webinar PresenterChristine (Brenton) Boucher, LPC, LADC, CBIS(860) 965-2443cccschristine@gmail.comCultivating Change Counseling Services, LLCTolland, CTYour
Webinar Learning Objectives12Understand basicfunctions of the brainand how these arealtered during braininjuryUnderstand howsubstance usedisorders impact braininjury recovery3Learn ways to modifyaddiction treatment for braininjury survivors
The Merging of Two FieldsLimited education and understanding across fieldsBrain injury survivors are twice as likely to have abused alcohol/substance prior totheir injury and up to 20% of survivors will develop a substance use disorder afterinjuryHigher drop out rates in treatment after a TBI due to ineffective methods, lack ofunderstanding around TBI, premature discharge due to “non-compliance”, etc.Availability of treatment programs that address both substance abuse and braininjury are lackingIn order for treatment to be effective after brain injury, methods need to bemodified. This is not yet universally understood or accepted.We know the who and the what, but what about the how?
“Substance abuse is a risk factor for having atraumatic brain injury and traumatic brain injury is arisk factor for developing a substance abuseproblem.”– John Corrigan, PhD
Polling Question #1
Anatomy of the Brain
Prefrontal CortexSocial cognitionMoral cognitionInhibitionControlGoal-settingDelayed gratificationThe prefrontal cortex is the part of the brain often damaged byboth chronic substance abuse and brain injury
Frontal LobeProblem solving ation
Limbic SystemAmygdala – “fight or flight”response, emotions,emotional memoriesHippocampus – memoryfunction, highlysusceptible to loss ofoxygen
So What Happens inBrain Injury?
Brain Injury Defined – TBI vs. ABITraumatic Brain Injury(65% annually)Cause of InjuryMVA“an insult to the brain, not of adegenerative or congenital nature butcaused by an external physical force, thatmay produce a diminished or altered stateof consciousness, which results in animpairment of cognitive abilities and/orphysical functioning. It can also result inthe disturbance of behavioral or emotionalfunctioning. These impairments may beeither temporary or permanent and causepartial or total functional disability orpsychosocial maladjustment” - her
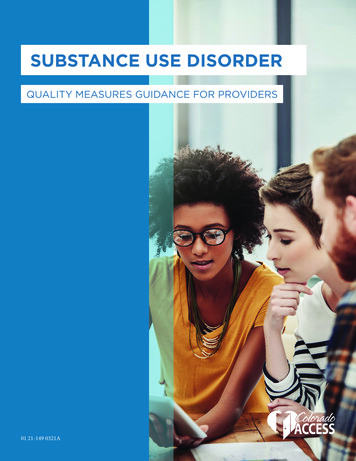
Brain Injury Defined – TBI vs. ABIAcquired Brain Injury(35% annually)“an injury to the brain that hasoccurred after birth and is nothereditary, congenital, ordegenerative. The injury commonlyresults in a change in neuronalactivity, which affects the physicalintegrity, the metabolic activity, or thefunctional ability of the cell. The termdoes not refer to the brain injuriesinduced by birth trauma.” - BIAACause of InjuryStroke7%6%Tumor87%Other,includingTBI
“ A Silent Epidemic”(‘looking good, but feeling strange’)Approx. 5.3 million people in the United States living with a disability due to braininjuryApprox. 1.4 million new brain injuries sustained every year in the United States1.1 million require a visit to the emergency room235,000 require hospitalization50,000 are fatal – of these almost 32% are due to MVA relatedinjuriesInjury is 1.5 times more likely in men than women, at any ageRisk of a second injury is 3x greater and risk of a third injury is 8x greaterThe estimated cost per year to society is 76.5 billion.
Types of InjuriesPrimary – original insult or injurySecondary – swelling, bruising, bleeding,or lack of oxygen resulting from theprimary insultOpen – brain has been exposed, skullhas been penetratedClosed – brain has been harmed, butskull remains intactFocal – damage to the brain remains inone primary locationDiffuse – connections throughout thebrain are stretched and/or broken dueto shaking, tearing, or stretchingthrough rotationCoup-Contrecoup – brain bounces backand forth or side to side upon impact
Measurement of InjuryInpatientGlascow Coma ScaleLoss of ConsciousnessPost-traumatic AmnesiaOther factors, tests, etc.MildModerateSevereOutpatientAcute RehabLong-term rehabResidentialEtc.
Signs, Symptoms, and EffectsPhysicalHeadachesDizzinessFatigueVisual impairmentBalance problemsSeizuresMotor impairmentsReduced mobilityMuscle stiffnessWeaknessCognitiveMemory lossPoor concentrationPoor attentionPoor judgmentPoor decision makingDisorientationLanguage difficultiesLack of awarenessConfabulationSlowed thought processSlowed speechConcrete thinkingEmotionalDepressionAnxietyMood swingsFlattened emotionIrritabilityAgitationInappropriate behaviorsIncreased frustrationIsolationLack of motivationImpulsivenessEgocentrism
The ‘Cycle of ustration
And What AboutSubstance UseDisorders?
Some Perspective40% - 60% of people with a substance use disorder have also had a previous traumatic brain injurythe cost of alcohol/substance abuse to our society is over 700 billion per yearHealth CareOverallTobacco 130 billion 295 billionAlcohol 25 billion 224 billionIllicit Drugs 11 billion 193 billion2008 National Survey on Drug Use and Health23.1 million people (ages 12 ) were in need of addiction-specific treatment20.8 million people did not receive treatment2.3 million people did receive treatment (10%)WHY?
Of that 20.8 million, 95.2% never soughttreatmentMost common reasons- won’t help- stigma attached to being an addict- no one else cares- would rather not live any longer- hope it will go away on its on- fear of being cut off from supply- fear of giving up their “high”- denial and control
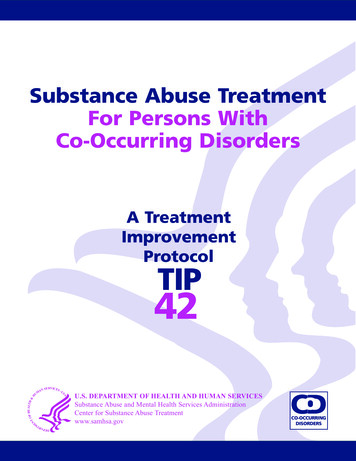
3.7% felt they needed treatment, but stilldid not seek itTreatment Needed, Not Sought11.812.9Not Ready38.8No Insurance/CostPossible Effect on Job12.3Not Sure Where32.1Possible Negative Opinion
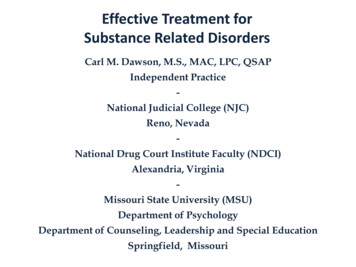
And 1.1% felt that needed treatment, sought itout, but still did not receive itTreatment Needed, Sought, but NotObtained7.4 7.7Cost/No insuranceNot Ready8.327.48.2No transportation29.38.110.5Self-treated13Unsure whereWrong timingLack of tx availability
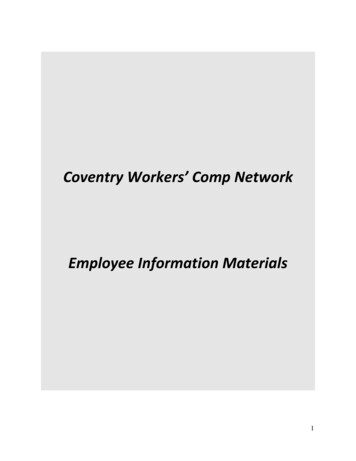
Data Obtained by The National Institute on DrugAbuse and The CDCDEATHS DUE TO ineBenzodiazepinesOpioidsIn all drug categories, men had a higher rate of overdose.Prescriptions
The Brain On Drugsdisrupted communication between different areas of the brainchanges in chemical structurenegative effect on one’s ability to have good impulse controlpoor decision makingmemory loss, mood swings
The Cycle of AddictionSober/HighwearsoffGuilt/Shamearound aviorsCravingsPoor High
Typical Components of Treatment forSubstance Use Disorders(and why they may not work for TBI)MedicationsStages of ChangeCBT, Motivational InterviewingMotivational Incentives / Contingency ManagementAbstinence Model vs. Harm Reduction ModelSelf Help / 12 Step GroupsInpatient / Residential SettingsGoals of treatmentReduce or eliminate useIdentify triggers to cravingsDesensitize client to their cravingsRebuild social network / Repair relationships
But what happens whenthey collide?
Polling Question #2
Some More Perspective.In adolescents and adults:20% of those hospitalized were intoxicated at the time of injury30% of those requiring rehab were intoxicated at the time of injury50% of those treated in acute rehab had a prior history of alcohol abuse35% of those treated in acute rehab had a prior history of substanceabuse60% of those treated in inpatient rehab had a history of a substance usedisorder44-66% of TBI survivors report alcohol abuse issues compared to 24% of non-TBIsurvivors21-37% of TBI survivors report use of illegal drugs compared to 15% of non-TBIsurvivors
Effects of Continued Useslower recoveryincreased damage to the brainincreased behavioral issuescontinued impact to cognitive functioningmore powerful effects from alcohol/drugsseizuresincreased depression, anxiety, etc.risk of additional head injuries
Additional Barriers to Treatmentscreening for brain injury is not doneghostinganosognosiahoneymoon period – 2-5 yearsmisdiagnosisnon-compliant or resistanttreatment may be unavailable or require an inpatient settingadditional transportation/financial concerns
“Ghosting”remembering who you were prior to your injury and striving to return to that lifecan be considered an identity disordercan create hostility with providers as client attempts to receive feedbackconsistent with their viewed selfALWAYS take this into consideration when treatment planning
Anosognosialack of awareness around physical or cognitive deficitsspecifically damage to the right parietal, right frontal areas of the braindoesn’t necessarily pertain to all deficitscan improve over timehow?do not use failure as a way to teachdo not point out deficitsutilize compensatory strategiesmain a supportive relationship
So how do we providetreatment?
Polling Question #3
What Doesn’t WorkClient attends an intake assessment. They mention they were in a car accident last year andhave felt different ever since. To cope with this, they have started drinking alcohol daily andoccasionally using cocaine. You complete your assessment and suggest they meet with apsychiatrist and attend a group therapy for people actively abusing alcohol/substances. Theyagree to try out your recommendations. Later that week they meet with a psychiatrist andstart group therapy weekly. The medications start making the client fatigued. Group consistsof sharing past use history, watching an educational film on addiction, and discussing triggers.Homework is assigned and at the second group homework is reviewed and the second part ofthe film is viewed. The client never did the assignment and appears lost when watching thefilm. The client misses group three and four so you call to check in. They apologize andrequest to meet with you individually to discuss some concerns. You’re unable toaccommodate this due to a high caseload and busy schedule so the client agrees to attendthe next group. The client again does not show up, so you discharge them due to treatmentnon-compliance and figure they are resistant to treatment or not ready to change.What went wrong?
A Community Based Model Suggested by JohnCorrigan, PhD and Colleaguescombination of education, intensive casemanagement, and inter-professionalconsultationsignificant differences in outcome foundwhen comparing untreated clients,premature discharge, and completionof treatment goalsmedian length of stay in order for client tobe discharged successfully was 2years
Early Intervention andScreening Tools“honeymoon periods” are common immediately after a brain injury due toincreased treatment and supervision – but treatment is still important!TBI Screening Form- HELPSMontreal Cognitive Assessment – MoCANeuropsychological Assessment
Additional Treatment Goalsnot necessarily changed, but possibly refocusedengagement – how?“success” is redefinedbuilding awareness around brain injury and resulting changes (insight)increasing independencemodifying behavior if neededde-escalation techniquesboundary settingsocialization
Behavior ModificationDo’sDont’sDe-escalation-Speak slowly/clearly/calmlyGentle/caringOffer a chance to calm downAvoid nervous behaviorTake a breakGive them space-Involve othersBe threatening or instill fearRespond in a hostile mannerRaise your voiceSpeak too fastRestrict movementSocialization-Create new social connectionsEncourage discussion amongpeersAssist in conflict resolution-Force itOverwhelmRely solely on peer interactionProvide tx with only non-TBIclientsSet and maintain consistentprofessional limitsExplain why a behavior may beinappropriateRemind clients of the boundarysetRedirect behaviorCreate group and/or programrulesEncourage boundary settingwith peers-Joke or laugh off inappropriatebehaviorAllow consistent breaking ofgroup rulesIgnore when a client showsgood boundary setting orfollowingGet frustratedBoundary Setting---
A Different Course of Treatment“wrap around” treatmenteducation, individual, group, family, self-help, case management, teamincreased frequency of treatmentshorter length of treatment sessionslonger duration of treatmentlocation of treatmentstructured, concrete, repetitivematerial is presented in a variety of formatsencourage note taking during sessionsmodified treatment planningfeedback provided
Compensatory StrategiesMemoryFriends/FamilyCalendarListsCell Phones/TabletsClocks/AlarmsAttentionRoutineGiving yourself extra timeTalk through tasksChecklistsOrganizationFile FoldersNote-takingListsEmotionsWalk awayCount to 10Take a deep breathAvoid unpleasant situationsLanguageNote cardsCue to slow downAsk others to slow downSocial SkillsModeling by othersRole playingPraise
Modified Treatment ToolsThe 12 Steps for Traumatic Brain Injuryie. AA Step One – “We admitted we were powerless over alcohol;that our lives had become unmanageable”ie. Modified for TBI – “Admit that if you drink and/or use drugs yourlife will be out of control. Admit that the use of substances afterhaving had a TBI will make your life unmanageable.”Substance Use/Brain Injury (SUBI) Bridging Project – Client WorkbookThe Brown Schools Rehabilitation Center – 12 Step WorkbookThe Mask Exercise
Important Additions to Treatment(it’s not just about the substances)Nutrition counselingFamily ts/MedicationYogaSocial trainingBasic mental health educationAnger managementStress managementSupport systems
15 Tips for Treating SUD in TBI Survivors1)When being assigned a new client make sure to read the summary of the neuropsychological evaluationto better understand the client’s cognitive strengths and weaknesses. Be sure to accommodate these asyou provide services.2)Use concrete examples to explain your points. Use visual aids to show what you mean, don’t describe it.3)If someone is hearing or visually impaired, make sure they sit close to the information being presented4)Requiring complete abstinence is not usually helpful and may only increase resistance. Instead,encourage the client to decrease their use and assist them in developing a plan to reduce the harm oftheir use.5)Introduce new information slowly and in small increments. Repeat frequently.6)Encourage clients to take notes or complete worksheets to aid in later recall.7)Keep sessions very structured – check in, review previous session, present material, activity/discussion,review, homework (if applicable).8)Be sure to redirect any monopolizing behavior by asking others to offer their suggestions or opinions.
15 Tips for Treating SUD in TBI SurvivorsContinued.9)If any client tends to fall behind, suggest that another client offer them assistance or offer moreindividual time10) Clients will be late and will miss sessions. Allow room for this and try to understand the reason behind it.Don’t jump to discharge.11) Some clients may not be comfortable sitting in an unfamiliar group or even coming in for individualsessions. Be willing to go where the client is more comfortable in order to being the engagementprocess.12) Be attentive to mood shifts and non-verbal communication. If you notice a client becoming agitated orbeginning to escalate, encourage them to talk about what is upsetting them. If they become fullyescalated allow them to take a moment away. Do not engage them in further conversation.13) Make sure to keep clients on the topic being discussed. If a client begins to stray, redirect by remindingthe client what was being talked about.14) If it is difficult to follow a client’s thought process, ask questions to clarify. This will also make it easier forothers to understand.15) Remind clients to take turns speaking. If someone is interrupted, redirect and let the client finish whatthey were saying.
Back To Our Client.Why was treatment ineffective for this client?treatment was never offered at the time of injuryeducation about brain injury was never providedneuropsychological evaluation was never requestedonly group therapy was assigned, individual time was unavailableunable to relate to other group memberssessions were only weeklya lot of information was provided in group therapy, some of it being based on previoussessionsno assistance was provided to help client remember appointmentsit was assumed that client was resistant when in actuality they were set up to fail
And Remember.every brain is different, so every brain injury is different and the resulting effectsare different“time does not heal a brain injury, it reveals it”“While the rest of the world is trying to get ahead of the ball, the brain injuredperson is trying to determine what the ball is, where the ball is, and perhaps evenwhy the ball is.” - Survivor
ResourcesBrainline.orgBrain Injury Association of AmericaState/Local Brain Injury AssociationsTBI Model Systems National DatabaseOSU Suboptimal Outcomes StudyOhio Valley Center for Brain Injury Prevention and RehabDrugAbuse.govVinland National Center
Thank You!Christine (Brenton) Boucher, LPC, LADC, CBIS(860) 965-2443cccschristine@gmail.comCultivating Change Counseling Services, LLCTolland, CTYour
www.naadac.org/eatingdisorders
Cost to Watch:FreeCE HoursAvailable:1.5 CEsCE Certificate forNAADACMembers:FreeCE Certificate forNon-members: 20CE CertificateTo obtain a CE Certificate for the time you spentwatching this webinar:1.Watch this entire webinar.2.Pass the online CE quiz, which is posted atwww.naadac.org/braininjurysurvivors3.If applicable, submit payment for CE certificateor join NAADAC.4.A CE certificate will be emailed to you within 21days of submitting the quiz.
Upcoming WebinarsFebruary 10, 2016March 9, 2016The Neurocognitive Effects of MaternalPrenatal Alcohol Consumption on the Fetusand Postnatal Developing Childby Paulette PrittBuild Your Business with the DOT/SAPQualificationby Wanda McMichaelFebruary 24, 2016The Spirituality of Addictionby Nina Marie CaronaMarch 23, 2016E-Cigarettes: A Cessation Device orAlternative Vice? The Good, the Bad, theUglyby VJ Sleightwww.naadac.org/webinars
www.naadac.org/webinarsFree CEs aadac.org/join
WEBINAR SERIESOver 75 CEs of free educationalwebinars are available. Educationcredits are FREE for NAADACmembers.MAGAZINE ARTICLESIn each issue of Advances inAddiction & Recovery, NAADAC'smagazine, one article is eligible forCEs.FACE-TO-FACE SEMINARSNAADAC offers face-to-faceseminars of varying lengths in theU.S. and abroad.INDEPENDENT STUDYCOURSESEarn CEs at home and at your ownpace (includes study guide andonline examination).CONFERENCESNAADAC Annual Conference inMinneapolis, MinnesotaOctober 7-11, 2016.CERTIFICATE PROGRAMSDemonstrate advanced educationin diverse topics with the NAADACCertificate Programs.
Contact Us!NAADACorgNAADAC1001 N. Fairfax Street, Suite 201Alexandria, VA 22314phone: 703.741.7686 / 800.548.0497fax: 703.741.7698 / AADAC
Acquired Brain Injury (35% annually) Brain Injury Defined -TBI vs. ABI "an injury to the brain that has occurred after birth and is not hereditary, congenital, or degenerative. The injury commonly results in a change in neuronal activity, which affects the physical integrity, the metabolic activity, or the functional ability of the cell .