Transcription
Rural Hospital Mergers andAcquisitions: 2005-2016Dunc Williams, Jr.1-3 and George H. Pink, PhD1,21 Universityof North Carolina Chapel Hill, Gillings School of Global Public Health, Department of Health Policyand Management2University of North Carolina Chapel Hill, Sheps Center for Health Services Research, North Carolina RuralHealth Research and Policy Analysis Center3Medical University of South Carolina, College of Health Professions, Department of Health Care Leadershipand ManagementGateway Webinar, November 1, 2018This work is funded by federal Office of Rural Health Policy, Award #U1GRH07633Disclaimer: The views and opinions expressed in this presentation are those of theauthors and do not necessarily reflect the official policy or position of any funderor employer.Agenda§ The current wave of mergers and acquisitions inhealthcare§ Why hospitals are merging: an example§ Rural hospitals as targets§ The volume of rural hospital mergers§ What types of rural hospitals have merged?§ Mergers have the attention of law makers§ Conclusion21
Key Takeaways1.The number of rural hospital mergers increased steadily from 2009through 2014, and then dropped in 2015 and 2016.2.Over half of all rural hospitals that merged (n 173) were in 11 states, mostfrequently in Oklahoma (n 22), Texas (n 22), and Wisconsin (n 19).3.Compared to rural hospitals that did not merge during the sample period,rural hospitals that merged are more likely to:- Report lower total margins and capital financing constraints- Be closer to the nearest large hospital, bigger, and serve larger markets4.Mergers may provide an opportunity for rural hospitals to access muchneeded capital and continue providing some level of care in thecommunity. However, changes in services provided at those hospitalscould hinder access to care and further widen the gap between rural andurban health disparities.3The current wave of mergersand acquisitions in healthcare42
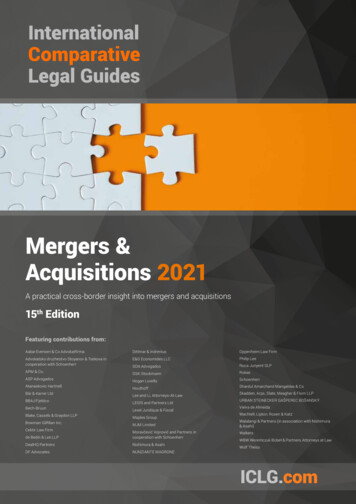
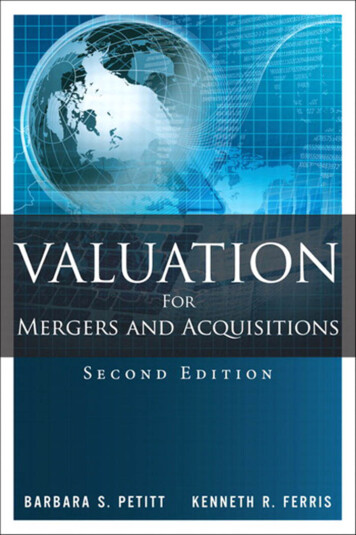
Defining a Hospital MergerAcquirerTarget5Health Care Services Mergers are Increasing 200 180 160Billions of Dollars 140 120 100 80 60 40 20 020132014201520162017Dollar ValueSource: Irving Levin Associates63
Health Care Services Mergers Continue to Increase in 2018“Healthcare companies have announcedtransactions totaling about 156 billion inthe first three months of 2018, makingthis the biggest first quarter forhealthcare mergers and acquisitions inmore than 10 years, according to datacompiled by Bloomberg.”10/31/187Why Hospitals are Merging§ Risk-bearingcapabilities§ Care continuum§ Network§ Capital resources§ Diversified operations§ Clinical and businessintelligenceinfrastructure§ Brand and presenceKaufman Hall. 2017 in Review: The year M&A shook the healthcare landscape, 2018.Available at: 7-review-yearma-shook-healthcare-landscape.84
What Happens Afterwards at Merged Hospitals?§ Prices increase§ In a report to the Committee on Ways and Means Health Subcommittee(2013), Martin Gaynor summarized eight merger studies and found pricesincrease 10-44% at merged hospitals.§ Capital expenditures increase§ Costs decrease§ Services provided decrease§ Staff levels decrease9Why hospitals are merging:An example105
§ The Acquirer: Hospital Corporation of America§ Based in Nashville TN§ 177 hospitals§ Largest hospital operator in the U.S.§ For-profit§ The Target: Mission Health§ Based in Asheville NC§ 6-hospital system§ Serves western North Carolina§ Not-for-profit11HCA acquisition of Mission Health The board of Mission Health has signed a definitive agreementto be acquired by HCA Healthcare. HCA currently does notoperate any hospitals in North Carolina. Under the proposedtransaction, HCA would use Mission Health as its platform forgrowth and expansion across the state. "HCA brings a unique scale relative to back office efficienciesthat have been a challenge for us," Mission Health Presidentand CEO Ronald A. Paulus, MD, told Becker's Hospital Review."While other potential not-for-profit partners would also haveadded to Mission Health's capabilities, no one can reallycompete on the scale platform for back office, administrativeoverhead and supply chain efficiencies."10/31/18126
HCA acquisition of Mission Health Dr. Paulus also emphasized the unique clinical capabilitiesHCA has to offer and HCA's experience in negotiating withmanaged care organizations across the country. "They havethe balance sheet and staying power to really make sure thecontracts they achieve are fair and appropriate," he says. Mission and HCA intend to create a healthcare innovationfund that will be based in Asheville and dedicated tofostering innovations and companies dedicated toimproving health. Mission and HCA will each contribute 25 million to the fund. Mission Health, which is currently atax-exempt organization, is also expected to generatemillions of dollars in tax revenues as part of HCA.10/31/1813HCA acquisition of Mission Health The innovation fund is in addition to the establishment of alarge new foundation that would provide tens of millions ofdollars in annual investments dedicated to improving thehealth and wellbeing of western North Carolina's 18-countyregion. Because of the growth potential HCA sees lookingacross the Carolinas, the company intends to set up Missionas an independent division within HCA. Mission Health Board Member Tom Oreck told Becker'sthere couldn't be a better time for Mission to pursue thistype of partnership.10/31/18147
HCA acquisition of Mission Health "Ron and his team have done an amazing job of buildingthis system up from a quality perspective that is recognizednationally as well as creating efficiencies within theoperation that make it competitive in a very, very toughenvironment. It is actually the perfect time for this type of apartnership to be created because it's when we're at ourstrongest," he says. "The environment is going to gettougher and tougher, and it's going to require the kind ofresources HCA has to maintain and improve quality whilebeing able to manage costs.“ The deal is currently on the desk of NC Attorney GeneralJosh Stein who is expected to approve or amend the dealnear the end of health.html10/31/1815Rural Hospitals as Targets168
Rural Hospitals are a Common Acquisition Target1. To meet value-based-purchasing requirements,hospitals must make capital investments thatmany rural hospitals cannot afford independentof a merger2. Financially distressed rural hospitals merge toimprove finances and survive3. Acquirers target rural hospitals in a merger toincrease market share and control costs17Why Mergers May be Good for Rural Hospitals§ Access to capital§ Joint purchasing and§ ACO and value-basedshared services§ Split-billing§ Provider recruitment§ Clinical integration andpayment participationand access tospecialists§ Negotiating powerstandardization§ Survival!189
Why Mergers May be Bad for Rural Hospitals Loss of local control Centralizedadministration Outsourcing of supportservices Greater use of agency Relocation of specialist orclinical services tomother ship Loss of local employment Increased travel time toaccess specific servicesversus full-time localnurses19Key Takeaways1. Mergers may provide an opportunity for ruralhospitals to access much-needed capital andcontinue providing some level of care in thecommunity.2. However, changes in services provided at thosehospitals could hinder access to care and furtherwiden the gap between rural and urban healthdisparities.2010
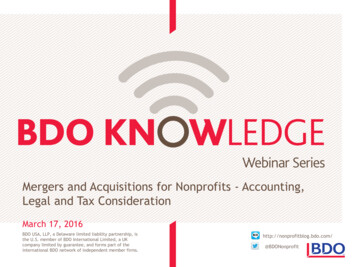
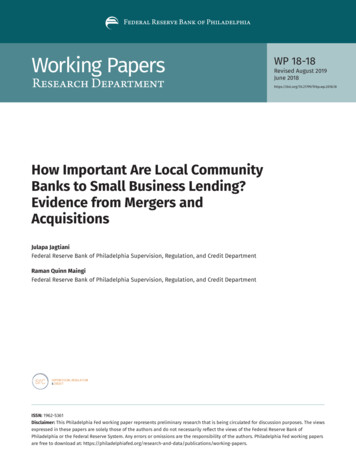
The volume of rural hospitalmergers21Number of Rural Hospital Mergers by 01220132014201520162211
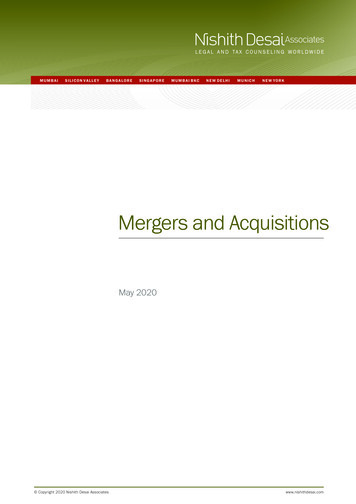
Multiple Mergers35Number of rural hospitals302520151050TwoThreeFourFiveNumber of times a rural hospital merged from 2005 through 201623Number of Unique Rural Hospitals that Merged by State2412
Rural Hospital Mergers by State, w sconsin19Kentucky10South Dakota3North Carolina18Minnesota10North rida9Montana2Georgia16Louisiana7New Mexico2South Carolina15Oregon7Washington2Alabama14Maine6New Hampshire1Illinois13Iowa5Hawaii1Michigan13West ornia3MassachuseWs1*Table includes the number of 2005-2016 rural hospital mergers (380) inwhich 326 unique rural hospitals were involved.25Key Takeaways1. The number of rural hospital mergers increasedsteadily from 2009 through 2014, and thendropped in 2015 and 2016.2. Over half of all rural hospitals that merged(n 173) were in 11 states, most frequently inOklahoma (n 22), Texas (n 22), and Wisconsin(n 19).2613
What types of rural hospitalshave merged?27Hospital Characteristics, 2002-2016Non-MergedRural HospitalsMerged Rural Hospitals2,646326Rural PPS, Non-CAH (%)53.32%69.73%For Profit (%)6.64%20.14%27.19%10.69%Largest QuartileDriving Distance from Hospital toNearest Large Hospital ( 100 beds,miles) (median)Medicare Outpatient Payer Mix e Obstetrics (%)56.67%59.48%Number of HospitalsSize (Revenue, %)Smallest QuartileAll reported differences are statistically significant at p .001.2814
Market Characteristics, 2002-2016Population (median)Unemployment Rate (%, median)Non-MergedRural HospitalsMerged Rural 30.07%35.70%54.77%18.52%4.43%Region (%, mean)NortheastMidwestSouthWestAll reported differences are statistically significant at p .001.29Revenue and Efficiency Characteristics, 2002-2016Total Margin (%, median)Medicare Outpatient Cost to Charge(%, median)FTEs per Bed (median)Non-MergedRural HospitalsMerged Rural Hospitals2.68%1.67%40.85%30.08%5.504.59All reported differences are statistically significant at p .001.3015
Capital Characteristics, 2002-2016Ability to Cover Debt PaymentsNon-MergedRural HospitalsMerged Rural Hospitals61.69%51.09%23.21%36.26%25.63%20.78% 10.5m 12.2mPlant Age (%)Newest QuartileOldest QuartileTotal Capital Expenditures (mean)All reported differences are statistically significant at p .001.31Key TakeawaysCompared to rural hospitals that did notmerge during the sample period, ruralhospitals that merged are more likely to:-Be PPS hospitalsBe for-profitHave greater net patient revenueBe closer to the nearest large hospitalServe larger marketsBe located in the SouthReport lower total marginHave newer plant age3216
Mergers have the attention oflawmakers33Rural hospital mergers and lab revenue§ Merging with a rural target hospital to increaselaboratory revenue for services renderedelsewhere.§ The acquirer is often a private entity.§ Increases can be substantial: Stamford MemorialHospital in Stamford Texas increased hospitaloutpatient lab charges 10,926% in one year – from 632,000 in 2015 to nearly 70 million in 2016.§ This issue is now the subject of multiple lawsuitsand a congressional inquiry.Source: Tara Bannow. Hospital lab charge spikes found at rural hospitals. Modern Healthcare, 2018.Available at: EWS/1806299803417
Rural hospital mergers and Medicare§ “Bipartisan concern over the degree to which Medicarepayment policy may be accelerating hospital consolidationand negatively impacting the Medicare program has beenpresent in Congress for some time,” wrote Reps. GregWalden, R-Ore., Michael C. Burgess, M.D., R-Texas, andGregg Harper, R-Miss., in the letter to MedPAC.§ “Through its public hearings, the Committee has hearddiffering views from experts on the extent to whichconsolidation is a cost driver in the Medicare program andthe degree to which payment policies of the Medicareprogram encourage such nclusion§ Fundamental changes to the health care system havespurred growth in the M&A market§ Hospitals and other providers are exploring partnershipoptions to strategically position themselves as best aspossible for the future§ M&As are financial and legal events that have manynon-financial consequences§ These findings support the need for further researchinvestigating why so many rural hospitals are merging,the financial impact of merging, and the impact onaccess to care within rural communities.3618
North Carolina Rural Health Research ProgramLocation:Cecil G. Sheps Center for Health Services ResearchUniversity of North Carolina at Chapel HillWebsite: ural-health/Email: ncrural@unc.eduColleagues:Mark Holmes, PhDGeorge Pink, PhDKristin Reiter, PhDDenise Kirk, MSJulie PerryRandy Randolph, MRPSharita Thomas, MPPKristie Thompson, MA37ResourcesNorth Carolina Rural Health Research jects/rural-health/Rural Health Research Gatewaywww.ruralhealthresearch.orgRural Health Information Hubwww.ruralhealthinfo.org/National Rural Health Associationwww.ruralhealthweb.orgNational Organization of State Offices of Rural Healthwww.nosorh.org3819
Rural HealthResearch GatewayThe Rural Health Research Gateway provides access to all publications and projectsfrom seven different research centers. Visit our website for more information.www.ruralhealthresearch.orgSign up for our email or RSS alerts!www.ruralhealthresearch.org/alertsShawnda Schroeder, PhDPrincipal Investigator701-777-0787 shawnda.schroeder@med.und.eduCenter for Rural HealthUniversity of North Dakota501 N. Columbia Road Stop 9037Grand Forks, ND 58202For 30 years, the Rural Health Research Centers have beenconducting policy-relevant research on healthcare in rural areas andproviding a voice for rural communities in the policy process.The Rural Health Research Gateway ensures this research lands in thehands of our rural leaders.www.ruralhealthresearch.orgThe Rural Health Research Center Program and Gateway are funded by theFederal Office of Rural Health Policy, Health Resources & Services Administration20
1 Rural Hospital Mergers and Acquisitions: 2005-2016 Dunc Williams, Jr.1-3 and George H. Pink, PhD1,2 1 University of North Carolina Chapel Hill, GillingsSchool of Global Public Health, Department of Health Policy and Management 2 University of North Carolina Chapel Hill, Sheps Center for Health Services Research, North Carolina Rural Health Research and Policy Analysis Center