Transcription
SubstanceAbuse Issuesafter TraumaticBrain InjuryLiving with Brain Injury
This brochure wasdeveloped forfriends, familymembers, andcaregivers ofpersons with braininjury. It also maybe used indiscussions withhealth careprofessionals andothers about theproblems one mayface when livingwith brain injury.Alcohol, Other Drugs and Brain InjuryJohn D. Corrigan, PhD, andGary L. Lamb-Hart, MDivThe Ohio Valley Center for Brain InjuryPrevention and RehabilitationDepartment of Physical Medicineand RehabilitationThe Ohio State University
Contents:1How much alcohol or other drugsis safe after brain injury?2How does alcohol or other drugsaffect a person who has had abrain injury?57How is the brain affected?8Are there treatmentapproaches that have beenproven effective for peoplewith brain injury?What about treatment forsubstance abuse after braininjury?11How can substance abuseservices be adapted forpeople with brain injury?16What about AA or otherself-help approaches?1718Internet ResourcesAdditional Information18 Suggestions for SubstanceAbuse Treatment ProvidersWorking With Clients Who HaveHad a Brain Injury21 The Nuts and Bolts of12-Step Self Help Groups26About the Author’s
How much alcohol or otherdrugs is safe after brain injury?The answer to this question iscomplicated because some drugs areillegal and others are not; some drugs maybe prescribed by a physician.Alcohol - because it is a legalsubstance for adults and is not prescribedby a physician - presents a more complexquestion. Our starting point is that certainlyno one should consume more alcohol afterbrain injury than would be considered safefor an adult who had not had an injury.Many people do not realize that adult menunder age 65 should not have more thantwo alcoholic drinks each day. For menover age 65 and for adult women, therecommended maximum is one drink perday.So the question becomes afterbrain injury should an individual drink eventhese amounts? Based on informationabout how alcohol and brain injury addtogether to affect the brain and how itworks, we have concluded that there is nosafe amount to drink. We suspect thatespecially during the early period ofrecovery - the first several years when thebrain is attempting to spontaneously healand otherwise accommodate the injury alcohol can inhibit these natural processes.There are many reasons why it isnot safe to consume drugs that are illegal.There is a great risk for illegal drugs tointeract with prescribed medications tocreate additional medical problems. Illegaldrugs may cause complications of othermedical conditions. There is also thepotential for being arrested, and greatervulnerability to injury by being the victim ofviolence. And last (but certainly not least)there is the potential for additional brain1
damage from use of these uncontrolledsubstances.Taking prescription drugs in greaterquantities than they are prescribed isanother form of drug abuse, and it too isnot advisable. Prescribed medications canbe as dangerous as illegal drugs when aperson takes more than the prescribedamount, or takes the prescribed amountmore frequently than indicated. Medicalcomplications and additional brain damagecan result from this kind of substanceabuse.If you have had a brain injury youshould not drink alcohol,you shouldnot use illegal drugs, and youshould not take prescriptionmedications in greater quantity thanprescribed.How does alcohol or other drugsaffect a person who has had a braininjury?There are multiple reasons whyalcohol and other drug use after braininjury is not recommended. The "User'sManual for Faster, More Reliable Operationof a Brain after Injury" (Ohio Valley Center,1994; www.ohiovalley.org ) describes 8reasons:1. People who use alcohol or otherdrugs after they have a brain injurydon't recover as much.Some brain cells (neurons) are killed andothers are disconnected at the time of abrain injury. Recovery means re-learningby making new connections betweenneurons. Using alcohol and other drugs2
after brain injury gets in the way of yourrecovery by interfering with newconnections between neurons.2. Brain injuries cause problems inbalance, walking or talking that getworse when a person uses alcohol orother drugs.For people whose brain injury causedproblems with balance, walking, or talking,alcohol and other drugs make the problemseven worse. Without brain injury, alcoholand other drugs can make people lose theirbalance or fall down. People who havebeen drinking or using other drugs may slurtheir speech. Problems walking and talkingcaused by your brain injury will beincreased by alcohol and other drugs.3. People who have had a brain injuryoften say or do things without thinkingfirst, a problem that is made worse byusing alcohol and other drugs.Every brain has a program called, "GoodIdea/Bad Idea." The program tells us whatis appropriate and what is not. Forexample, we may think to ourselves thatsomeone's sweater is really ugly, but"Good Idea/Bad Idea" keeps us fromsaying this out loud. For some people, abrain injury takes away the fine linebetween good ideas and bad ideas and"lets it all hang out." Alcohol can alsocause a person to say whatever comes tomind, no matter who it hurts. Alcoholtogether with a brain injury shuts off the"Good Idea/Bad Idea" program, and that'sa bad idea.4. Brain injuries cause problems withthinking, like concentration or memory,3
and using alcohol or other drugs makesthese problems worse.Many people have to learn new skills, orre-learn old ones, following a brain injury.People have trouble with concentration,memory, word finding, problem-solving andother thinking skills, depending on wherethe brain is injured. Alcohol and otherdrugs also interfere with the ability to thinkand learn new things. Adding alcohol andother drugs with your brain injury justmakes thinking that much harder.5. After brain injury, alcohol and otherdrugs have a more powerful effect.The brain is more sensitive to alcohol andother drugs after an injury. There are notas many neurons to absorb the alcohol orother drugs. No matter how much alcoholor other drugs a person was able to usebefore, it's less now. Also, alcoholinterferes with prescribed medications. Youget drunk faster and lose the good effect ofthe medicine.6. People who have had a brain injuryare more likely to have times that theyfeel low or depressed and drinkingalcohol and getting high on other drugsmakes this worse.Being depressed is fairly common after abrain injury. Sometimes it is the injury tothe brain that causes depression. It is alsothe change in a person's life that leads todepression. Everything is different-thereare financial worries, and there is boredom.Many people turn to using alcohol andother drugs to try to make this depressiongo away. They say it makes them lessworried, more relaxed and happier. That4
may be true, for a while, but it quicklymakes things worse. Alcohol depressesthe brain and that depresses you.7. After a brain injury, drinking alcoholor using other drugs can cause aseizure.Seizures are a problem for about 5% ofpeople who have a brain injury. Eventhough that is a low number, seizures areserious and steps need to be taken toavoid them. Some people require antiseizure medication. Mixing alcohol andother drugs with these medications is verydangerous and can INCREASE the chanceof seizure. Taking yourself off medicationsto drink is DANGEROUS. Doubling up onanti-seizure medications to drink isDANGEROUS. Get the facts from yourdoctor, and then use your brain.8. People who drink alcohol or useother drugs after a brain injury are morelikely to have another brain injury.Among people who have had one braininjury, the chance of a second injury isthree times greater. Brain injuries maycause problems with balance, coordination,vision and judgment that lead to otherinjuries. By drinking alcohol or using otherdrugs after a brain injury, you are morelikely to have another injury. Also, witheach brain injury it takes less force tocause greater harm.How is the brain affected?There is mounting researchevidence about the bad effects of alcoholand other drug use after brain injury.5
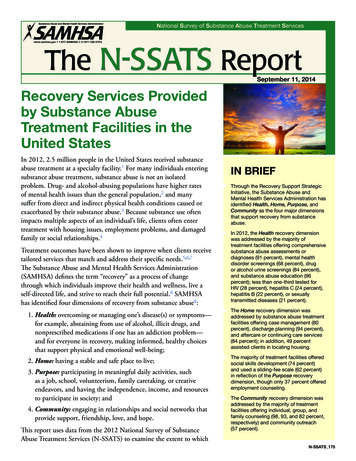
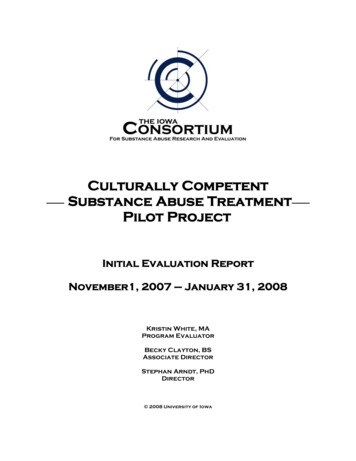
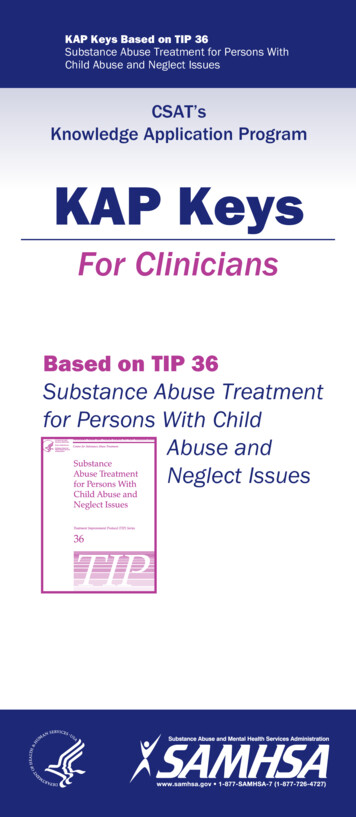
Several studies have found use andassociated with such unwanted outcomesas unemployment, living alone and feelingisolated, criminal activity, and lower lifesatisfaction. While these studies haveobserved associations between substanceuse and negative outcomes, cause andeffect is not fully understood.Brain injury does damage to yourbrain; abuse of alcohol or other drugs doestoo. There is research showing that whenbrain injury and substance abuse arecombined they have a worse effect on thebrain than either one has alone.As an example, Ian Baguley andcolleagues from Australia (see graphbelow) studied the P300 wave in eventrelated evoked potentials--an indication ofhow fast the brain detects new information.Their research showed that either heavysocial drinking or previous traumatic braininjury requiring hospitalization slowed brainfunctioning, and when combined they hadan "additive effect." An additive effectmeans that both together (heavy socialdrinking and previous brain injury) wereworse than either one alone.P300 Amplitude1614121086420ControlsAlcoholTBITBI AlcoholFrom Baguley, I. J., Felmingham, K. L., Lahz,S., Gordan, E., Lazzaro, I., & Schotte, D. E.(1997). Alcohol abuse and traumatic braininjury: Effect on event-related potentials.Archives of Physical Medicine andRehabilitation, 78 (11), 1248-1253.6
In this graph based on Baguely andcolleagues study, the higher the bar, thefaster the research participants respondedto new information. Those subjects whowere either heavy social drinkers or hadbeen hospitalized for a traumatic braininjury were slower responding then peoplewith neither; and those with both wereslower than those who had just one of theconditions.The effects of alcohol and otherdrugs are different for people who havehad a brain injury. It is important to get thefacts about how alcohol and other drugsaffect the brain. When your review the datait becomes clear that there is no amount ofalcohol or other drugs that is safe forpeople who have had brain injuries.What about treatment forsubstance abuse after brain injury?Many people benefit fromprofessional help when their drinking orother drug use is too much and is creatingproblems for them. One sign that a personcould use some assistance is when theyhave tried to cut down on their own, butsomehow the problem continues. Anothersign is when people who care about aperson begin worrying that he or she isdrinking to much. Finally, if a persons isfacing legal or medical problems-includinghaving another injury- it is advisable toseek help.In substance abuse treatment,perhaps the most well known andfrequently used theory is the Stages ofChange model developed by JamesProchaska and Carlos DiClemente. Thismodel describes how ready a person is toaddress problems related to their alcohol or7
other drug use. Stages start withprecontemplation (a person sees noproblem when there is one), and includecontemplation (weighing the pros and consof changing), determination (deciding tochange), action (making a specific plan forchange), and maintenance (sustainingsuccessful change despite urges to useagain). Substance abuse counselorsusually tailor treatment to a person's Stageof Change. Regardless a person'sreadiness to address an alcohol or otherdrug use problem, there is alwayssomething a professional substanceabuse counselor or treatment programcan provide.Are there treatment approachesthat have been proven effective forpeople with brain injury?There has not been very muchresearch about what substance abusetreatment methods do or do not work forpeople who have had brain injuries. Mostclinicians feel that techniques foundeffective for people in general can also beeffective for people who have had braininjuries; however, sometimes specialconsiderations or accommodations may beneeded to make the treatment useful andeffective. Following are brief descriptionsof common treatment approaches foralcohol and other drug abuse.Motivational Interventions havebeen used to help individuals becomeready to participate in treatment. Researchin the substance abuse field hasdemonstrated that motivationalenhancement techniques are associatedwith greater participation in substanceabuse treatment and positive treatment8
outcomes. Motivational enhancementtechniques must be matched to a person'sStages of Change. Motivationalinterventions seem like a promisingapproach to facilitating positive change forpeople with substance abuse problems andbrain injuries, though like most therapeuticapproaches it needs to be adapted to theindividual's ability for insight and selfmanagement.Cognitive-Behavioral Therapyuses cognitive and/or behavioral strategiesto identify and replace an individual'sirrational beliefs that arise from substanceabuse (e.g., "the only time I feelcomfortable is when I'm high") with rationalbeliefs (e.g., "it's hard to learn to becomfortable socially without doing drugsbut people do it all the time"). CognitiveBehavioral Therapy can be conducted aspart of individual or group treatment.Whether or not someone has had a braininjury, Cognitive-Behavioral Therapies needto be adapted to a person's capability forunderstanding the connections betweenbeliefs and feelings.Sometimes substance abusetreatment needs to take place in anenvironment where there is 24-hour perday supervision and treatment. One of themost common residential treatmentapproaches is the TherapeuticCommunity, or "TC". TC has been usedto address the needs of people withsubstance use disorders for more than 30years and its methods and effectivenesshave been well-documented. TC viewssubstance abuse as a problem of conduct,attitudes, moods, values, and emotionalmanagement. The approach focuses oncreating a community, including otherpeople addressing these problems, thatpromotes self-evaluation and recovery. For9
persons who have had brain injuries, theTC approach may need to be adapted toallow increased flexibility, decreasedintensity, and greater individualization.When it comes to the use ofprescription medications for the treatmentof substance abuse, there are not a lot ofchoices. Foremost among addictionrelated medications is methadone for thetreatment of heroin and other opioidaddiction. Methadone cannot be dispensedoutside designated methadone treatmentprograms. A new drug, buprenorphine, isavailable for the treatment of opioid abuseand dependence when prescribed andmonitored by a certified physician. In ourclinical work we have seen that prescriptionmedications for depression or anxietyare sometimes important for getting startedon changing alcohol or other drug abuse.Another medication, disulfiram or antibuse,is a well-established medication used todiscourage alcohol consumption. However,its use by individuals with brain injuries isgenerally discouraged. Naltrexone hasbeen used to reduce a person's cravingsfor alcohol, but there is no research on itseffectiveness for people who have hadbrain injuries.Substance abuse treatment oftenincludes both the individual and family orfriends. The greater a person's cognitiveimpairments after brain injury, the moreimportant it becomes that people in his orher surroundings are willing to be involvedin the treatment process. Similarly, forpeople who do not see themselves ashaving a problem (those who areprecontemplative), it is more important thatfamily and friends be willing to joinprofessionals to get a person startedaddressing their substance use.10
How can substance abuse servicesbe adapted for people with braininjury?There should be a very high priorityplaced on research about the effectivenessof current substance abuse treatments forpersons with brain injury. However, untilmore is known, current treatments andservices need to be adapted toaccommodate disability arising from braininjury.When a person with a brain injuryseeks help for a substance abuse problem,significant barriers to treatment may beencountered. The individual, family orfriends may need to advocate for the rightto appropriate treatment: Too many publicly fundedsubstance abuse programs stillhave physical facilities that preventor limit accessibility for individualswho use a wheelchair. This isagainst the law for publicly fundedagencies. They should be asked tomake services accessible in thesame way everyone else receivesthem. Admission criteria maydiscriminate against individuals withbrain injuries, out right or indirectly.For instance, requiring abstinencefrom all mood-altering substancesincluding prescribed medicationsprevents some individuals fromreceiving services. This is notappropriate.If a person with a brain injury is ableto get through the front door, literally andfiguratively, a new set of barriers often arisethat come from the cognitive impairmentsand unique learning styles common after11
brain injury. Professionals at the OhioValley Center for Brain Injury Preventionand Rehabilitation at Ohio State Universityhave made a number of recommendationsfor working collaboratively with substanceabuse treatment professionals. Theserecommendations assume that acollaborative relationship can be developedwith the individual provider that allows forexchange of ideas and information withoutanyone becoming defensive. Establishingsuch a relationship is by no means a given,but it is the cornerstone for long-termsuccess in treatment.Below are recommendations that anindividual, family member or friend mightmake to a substance abuse treatmentprovider who is inexperienced in workingwith people with brain injuries. Theserecommendations cover identification ofunique issues, adaptive or compensatorystrategies based on the individual's ownlearning style, provision of feedbackregarding inappropriate behavior, andcautions regarding jumping to a conclusionabout a person's motivation. Theserecommendations are also summarized atthe end of this brochure in "Suggestions forSubstance Abuse Treatment ProvidersWorking With Clients Who Have Had aBrain Injury."The substance abuse providershould determine a person's uniquecommunication and learning styles.A substance abuse provider'ssuccess in working with an individual withunique cognitive abilities will rely heavily ontheir ability to identify strengths andweaknesses. We have had our greatestsuccess by avoiding neuropsychologicaljargon and focusing the provider's attention12
on basic issues of communication andlearning. Understanding that a particularindividual learns better with written, oral orvisual input. When expression is an issue,often it is a simple matter of givingproviders permission to ask questions sothat they can learn to work more effectivelywith an augmented communication deviceor understand dysarthric speech.With regard to learning style,simplifying the concepts of attention andlearning can be very useful. In particularwe find it important that the providerunderstand the issues of shortenedattention span (including the interactionwith fatigue), as well as the impact ofenvironmental stimuli on attention(particularly how noisy or busy locationscan affect attention). With regard to newlearning, distinctions between languageand non-language styles are important, asis understanding memory impairmentswhen the exist. It is important tounderstand how attention affects both initialcomprehension and later recall.The substance abuse providershould assist the individual tocompensate for a unique learningstyle.Substance abuse treatmentprograms have come to rely heavily on theuse of groups for educational, not justexperiential, purposes. Manycompensatory strategies applicable toclassroom settings are appropriate insubstance abuse treatment, as well.Simple strategies like using writtenreminders for cueing recall, or schedules tostructure time are not standard in manyprograms (though all clients would probably13
benefit). The use of groups also reducesindividual attention, which may limit oneon-one opportunities to mediate thetreatment experience. In programs that usean Alcoholics Anonymous (AA) treatmentapproach, materials that have beenmodified to include greater visual cues aswell as less abstract reasoning areavailable.The substance abuse providershould provide direct feedbackregarding inappropriate behaviors.For some individuals with cognitiveimpairments there also may be problemswith inappropriate social behavior. In ourexperience, this behavior can be the mostchallenging for substance abuse treatmentprograms. Providers are often caught offguard by impulsive behavior, disinhibitedexpression of emotions, or intrusion onpersonal space. Consequently, they areusually ineffective in dealing with thesebehaviors, as well. Again, a minimalamount of instruction and permission tointervene can go a long way toward makingthe substance abuse treatment providermore comfortable with sociallyinappropriate behavior. We have alsofound that advanced structuring so thatsomething has been said about thebehavior before its first occurrence buildsboth trust and confidence.The substance abuse providershould be cautious when makinginferences about motivation basedon observed behaviors.Perhaps the most destructive factorundermining access to treatment forpersons with brain injury is a tendency for14
substance abuse treatment providers toconclude a person is not motivated whenthe behaviors are really a result ofcognitive impairments. For instance, theleader of a group asks a question to whicheach member is to respond. When it is theopportunity for individuals with memoryproblems to respond, they have nothing toadd. Group leaders think this is resistance;however, upon inquiry, individuals reportthat what they wanted to say when thequestion was first posed had beenforgotten by the time it comes their turn tospeak. Perhaps most frequent is thetendency for substance abuse providers toinfer that missed appointments or latearrival are signs of resistance to treatmentor denial of one's substance abuseproblem. There can be many reasons whyan individual with a brain injury might missan appointment or be late, includingresistance to treatment and denial. Poorplanning, poor memory, difficultiesarranging or handling transportation needto be considered as alternative hypothesesbefore the counselor jumps to theconclusion that the missed appointment issomehow related to motivation.The relationship that is establishedbetween a client and a substance abusecounselor is the single most importantfactor for successful treatment of alcoholand other drug problems. This relationshipis often called the therapeutic alliance. Youwill know you are developing a therapeuticalliance if after meeting with your counselora few times you feel like he or she listensand understands you, has confidence inyou and your ability to change, and issomeone you can trust. The need for apositive therapeutic alliance is especiallycritical for individuals with both a traumatic15
brain injury and a substance abuseproblem.What about AA or otherself-help approaches?Professional treatment sometimeshas natural limits and continuing carebeyond formal treatment is critical toachieving a long-term, satisfactory outcomefor individuals affected by substance usedisorders. Self-help or peer supportprograms can be an important interventionand an easily available source ofcontinuing care. Self-help approachesbegan with Alcoholics Anonymous, or"AA", and have grown to address a widevariety of addictions. Rational Recoveryand Moderation Management are twoother self-help approaches for alcoholproblems. Narcotics Anonymous (NA)and Cocaine Anonymous (CA), bothbased on AA, are two of the largest selfhelp organizations addressing illegal druguse.AA, NA and CA use the "12-step"method, with its focus on developingpersonal responsibility within the context ofpeer support. AA, NA, or CA groups arenot for everyone at all stages of recovery.For those still at a point that they areresistant to exploring their use ofsubstances as problematic, the introductionof AA/NA/CA may be too early andcounterproductive. Forcing a self-helpgroup on a person who is precontemplativemay create greater resistance later in theprocess of recovery when AA/NA/CA couldbe very helpful. A person may find supportin other areas of their life that are asproductive as AA/NA/CA, and it may bebetter to cultivate these natural supports.16
However, we have always found thatpeople who participated in self-help groupsbefore their injury can be more open toinvolvement after.When attendance at AA, NA or CAgroups are being considered there is acertain amount of planning that needs totake place. We think it is important toaccompany a person who has had braininjury and has never attended self-helpgroups to the first few meetings. Havingsomeone to share the initial experiencewith, and talk about it afterward, can makethe difference between dropping out orstaying with the group. We have alsofound that it is very useful to becomefamiliar with the nuts and bolts of self-helpgroups before attending. It is useful to beable to anticipate what will happen at ameeting. Included at the end of thisbrochure is a description of the "Nuts andBolts of Using Self-Help Groups." Wesuggest looking this over before attendinga meeting.Internet ResourcesGeneral Substance Abuse and Mental HealthServices Administration www.samhsa.gov National Institute on Alcohol Abuse andAlcoholism www.niaaa.nih.gov National Institute on Drug Abuse www.nida.nih.gov Alcohol Screening www.alcoholscreening.org Treatment Approaches Cognitive Behavior Therapy www.nacbt.org Motivational Interviewing17
ml Therapeutic Communities of America www.tcanet.org TBI and Substance Abuse Ohio Valley Center for Brain InjuryPrevention and Rehabilitation www.ohiovalley.org SynapShots (section on SubstanceAbuse) www.SynapShots.org Self-Help Groups Alcoholics Anonymous www.alcoholicsanonymous.org Cocaine Anonymous www.ca.org Moderation Management www.moderation.org Narcotics Anonymous www.na.org Rational Recovery www.rational.org Additional InformationSuggestions for Substance AbuseTreatment Providers WorkingWith Clients Who Have Had a BrainInjuryThe substance abuse treatment providershould determine a person's uniquecommunication and learning styles. Ask how well the person readsand writes; or evaluate via samples. Evaluate whether the individual isable to comprehend both writtenand spoken language. If someone is not able to speak(or speak easily), inquire as toalternate methods of expression(e.g., writing or gestures).18
Both ask about and observe aperson's attention span; be attunedto whether attention seems tochange in busy versus quietenvironments. Both ask about and observe aperson's capacity for new learning;inquire as to strengths andweaknesses or seek consultation todetermine optimum approaches.The substance abuse treatmentprovider should assist the individual tocompensate for a unique learning style. Modify written material to make itconcise and to the point. Paraphrase concepts, useconcrete examples, incorporatevisual aids, or otherwise present anidea in more than one way. If it helps, allow the individual totake notes or at least write downkey points for later review andrecall. Encourage the use of a calendaror planner; if the treatment programincludes a daily schedule, makesure a "pocket version" is kept foreasy reference. Make sure homeworkassignments are written down. After group sessions, meetindividually to review main points. Provide assistance with homeworkor worksheets; allow more time andtake into account reading or writingabilities. Enlist family, friends or otherservice providers to reinforce goals. Do not take for granted thatsomething learned in one situationwill be generalized to another.19
Repeat, review, rehearse, repeat,review, rehearse.The substance abuse providertreatment should provide directfeedback regarding inappropriatebehaviors. Let a person know a behavior isinappropriate; do not assume theindividual knows and is choosing todo so anyway. Provide straightforward feedbackabout when and where behaviorsare appropriate. Redirect tangential or excessivespeech, including a predeterminedmethod of signals for use in groups.The substance abuse treatment providershould be cautious when makinginferences about motivation based onobserved behaviors. Do not presume thatnon-compliance arises from lack ofmotivation or resistance, check itout. Be aware that unawareness ofdeficits can arise as a result ofspecific damage to the brain andmay not always be due to denial. Confrontation shuts down thinkingand elicits rigidity; roll withresistance. Do not just discharge fornon-compliance; follow-up and findout why someone has no-showedor otherwise not followed through.If information about a person's cognitiveabilities or neurobehavioral problems areavailable from a medical rehabilitation20
professional (physiatrist, rehabilitationpsychologist, neuropsychologist, speechlanguage pathologist or occupationaltherapist), substance abuse treatmentproviders would be well-advised to gainpermission to consult with thatprofessional.The Nuts and Bolts of12-Step Self Help GroupsFinding a meetingMost phone books will list a numberfor the closest AA/NA/CA central office,which can provide you with a list ofmeetings. Your local substance abusetreatment agency can also direct you tomeetings. Or you can go to www.alcoholics-anonymous.org and lookup you regional group's website to findcontact numbers.Kinds of MeetingsThere are four basic types ofmeetings based on whether they are"Open" or "Closed", and whether they usea "Lead" or "Discussion" format. Openmeans that the meeting is just that- open toanyone that would like to attend regardlessof admitting a problem with alcohol or otherdrugs. A closed meeting is only for thosewilling
alcohol and getting high on other drugs makes this worse. Being depressed is fairly common after a brain injury. Sometimes it is the injury to the brain that causes depression. It is also . had a brain injury. It is important to get the facts about how alcohol and other drugs affect the brain. When your review the data