Transcription
Patient-Driven Payment Model (PDPM): At-a-GlanceThe proposed PDPM establishes a rate on the 5-day MDS for the entire stay by combiningfive different case-mix components (PT, OT, SLP, Nursing, and Non-Therapy Ancillary) withthe non-case-mix component. The rate may be changed during the Medicare Part A stay bycompleting the Interim Payment Assessment (IPA) for substantial changes.Use the following at-a-glance tools to identify the case-mix group for each component andimprove your understanding of the proposed Patient-Driven Payment E: This document is intended to aid members in their review of the Patient-Driven Payment Model.Resources: FY 2019 SNF PPS Proposed Rulemaking and CMS draft PDPM Calculation Worksheet forSNFs. All information regarding PDPM is subject to change pending final rulemaking. AANAC has madeevery attempt to ensure the accuracy and reliability of the information provided. AANAC does notaccept any responsibility or liability for the accuracy, content, and completeness of the information.Copyright 2018, American Association of Post-Acute Care Nursing, d/b/a American Association of Nurse Assessment Coordination. All Rights Reserved. AANAC.org1
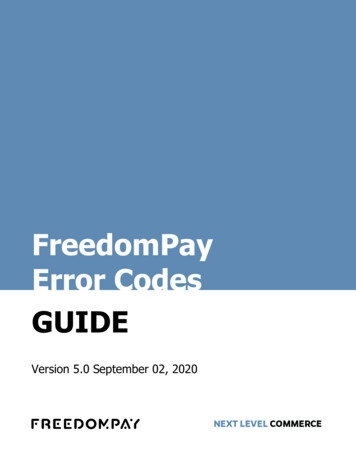
Proposed Patient-Driven Payment Model: At-a-GlancePT Component and OT Component*ClinicalCategoryMajor JointReplacement orSpinal dicSurgery andAcute NeurologicGG FunctionScorePT and OTCase-Mix Group0–5TA6–9TB10–23TC01, 07,09, 8824TD0–5TEGG0130A1 Self-care: ty: Lying to sitting onGG0170C1side of bed0–5TIGG0170D1 Mobility: Sit to stand6–9TJGG0170E1Mobility: Chair/bed-tochair transfer10–23TKGG0170F1Mobility: Toilet transfer24TLGG0170J1Mobility: Walk 50 feet with2 turns0–5TMGG0170K1 Mobility: Walk 150 feet6–9TN10–23TO24TPScoring Response for Section GG Items05, 06ScoreSet-up assistance, independent404Supervision or touching assistance303Partial/moderate assistance202Substantial/maximal assistance1Dependent, refused, not attempted0Section GG itemsSelf-care: Oral hygieneGG0130C1 Self-care: Toileting hygieneGG0170B1Mobility: Sit to lyingScore0–40–4(avg. of 2 bedmobility items)0–4(avg. of 3transfer items)0–4(avg. of 2walking items)PT Component and OT Component:PT and OT components will always result in thesame case-mix group; however, the PT and OTcase-mix indices/payment levels differ.NOTE: This document is intended to aid members in their review of the Patient-Driven Payment Model.Resources: FY 2019 SNF PPS Proposed Rulemaking and CMS draft PDPM Calculation Worksheet for SNFs. Allinformation regarding PDPM is subject to change pending final rulemaking. AANAC has made every attempt toensure the accuracy and reliability of the information provided. AANAC does not accept any responsibility orliability for the accuracy, content, and completeness of the information.Copyright 2018, American Association of Post-Acute Care Nursing, d/b/a American Association of Nurse Assessment Coordination. All Rights Reserved. AANAC.org2
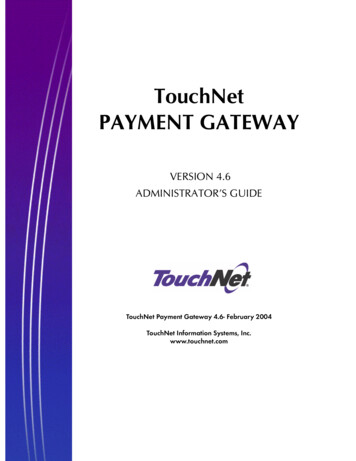
Proposed Patient-Driven Payment Model: At-a-GlanceSLP ComponentPresence of Acute Neurologic Condition,SLP-Related Comorbidity*,or Cognitive Impairment**NoneAny oneAny twoAll threePresence of:Swallowing Disorder (K0100A–D) ORMechanically Altered Diet (K0510C2)SLP othSLSLP-Related Comorbidities:Aphasia (I4300); CVA, TIA, or Stroke (I4500);Hemiplegia or Hemiparesis (I4900); TBI(I5500); Tracheostomy (O0100E2); Ventilator(I0100F2); Laryngeal Cancer, Apraxia,Dysphagia, ALS, Oral Cancers, Speech andLanguage Deficits (I8000)Cognitive Impairment:The PDPM cognitive level is based on theBrief Interview for Mental Status (BIMS) orstaff assessment. See the PDPM calculationworksheet provided by CMS for details.NOTE: This document is intended to aid members in their review of the Patient-Driven Payment Model.Resources: FY 2019 SNF PPS Proposed Rulemaking and CMS draft PDPM Calculation Worksheet for SNFs. Allinformation regarding PDPM is subject to change pending final rulemaking. AANAC has made every attempt toensure the accuracy and reliability of the information provided. AANAC does not accept any responsibility orliability for the accuracy, content, and completeness of the information.Copyright 2018, American Association of Post-Acute Care Nursing, d/b/a American Association of Nurse Assessment Coordination. All Rights Reserved. AANAC.org3
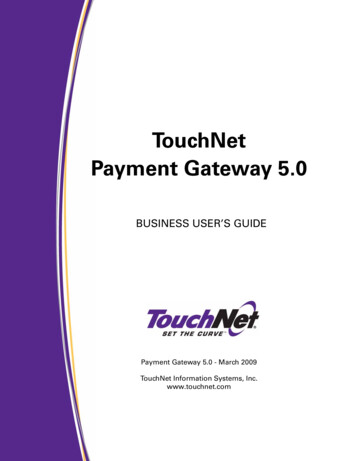
Proposed Patient-Driven Payment Model: At-a-GlanceNOTE: This document is intended to aid members in their review of the Patient-DrivenPayment Model. Resources: FY 2019 SNF PPS Proposed Rulemaking and CMS draftPDPM Calculation Worksheet for SNFs. All information regarding PDPM is subjectto change pending final rulemaking. AANAC has made every attempt to ensure theaccuracy and reliability of the information provided. AANAC does not accept anyresponsibility or liability for the accuracy, content, and completeness of the information.Nursing Component*RESIDENTGG-basedFunction ScoreEXTENSIVESERVICESYESES33 TRACHEOSTOMY & VENTILATOR 0-142 TRACHEOSTOMY OR VENTILATOR 0-141 INFECTION ISOLATION0-14ES2ES1NOSPECIALCARE 160-56-1415-16CDE22 NURSING REHAB 2 11-16BAB21 NURSING REHAB 0-111-16BAB10-56-1415-160-56-1415-16PDE2ADL2 DEPRESSEDYES1 NOTDEPRESSEDADL2 DEPRESSEDADLHDE1HBC2HBC1NOSPECIALCARE LOWYES1 NOTDEPRESSEDADL2 DEPRESSEDADLLDE1LBC2LBC1NOCLINICALLYCOMPLEXYES1 NOTDEPRESSEDADLCBC2CDE1CA2CBC1CA1NOBEHAVIOR SXCOGNITIONYESNOREDUCEDPHYSICALFUNCTION2 NURSINGREHAB 2 YES1 NURSINGREHAB 0-1Scoring Response for Section GG Items05, 06ADLADLScorePDE1PBC2PA2PBC1PA1Section GG itemsScoreSet-up assistance, independent4GG0130A1 Self-care: Eating0–404Supervision or touching assistance3GG0130C1 Self-care: Toileting hygiene0–403Partial/moderate assistance2GG0170B102Substantial/maximal assistance1Dependent, refused, not attempted0Mobility: Lying to sitting onGG0170C1side of bed01, 07,09, 88Nursing Component:See the CMS PDPM calculation worksheet forinclusion criteria for each nursing classification.Mobility: Sit to lyingGG0170D1 Mobility: Sit to standGG0170E1Mobility: Chair/bed-tochair transferGG0170F1Mobility: Toilet transfer0–4(avg. of 2 bedmobility items)0–4(avg. of 3transfer items)Copyright 2018, American Association of Post-Acute Care Nursing, d/b/a American Association of Nurse Assessment Coordination. All Rights Reserved. AANAC.org4
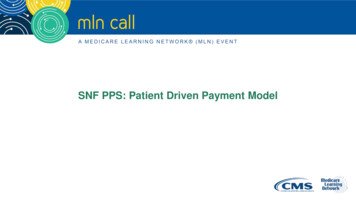
Proposed Patient-Driven Payment Model: At-a-GlanceNon-Therapy Ancillary (NTA) ComponentCondition/Extensive ServiceHIV/AIDSSourcePointsSNF Claim8MDS Item K0510A2, K0710A27Special Treatments/Programs: Intravenous Medication Post-admit CodeMDS Item O0100H25Special Treatments/Programs: Ventilator or Respirator Post-admit CodeMDS Item O0100F24Parenteral IV Feeding: Level LowMDS Item K0510A2,K0710A2, K0710B23Parenteral IV Feeding: Level HighLung Transplant StatusMDS Item I80003MDS Item O0100I22Major Organ Transplant Status, Except LungMDS Item I80002Active Diagnoses: Multiple Sclerosis CodeMDS Item I52002Opportunistic InfectionsMDS Item I80002Active Diagnoses: Asthma COPD Chronic Lung Disease CodeMDS Item I62002Bone/Joint/Muscle Infections/Necrosis—Except Aseptic Necrosis of BoneMDS Item I80002Chronic Myeloid LeukemiaMDS Item I80002Wound Infection CodeMDS Item I25002Active Diagnoses: Diabetes Mellitus (DM) CodeMDS Item I29002EndocarditisMDS Item I80001Immune DisordersMDS Item I80001End-Stage Liver DiseaseMDS Item I80001Special Treatments/Programs: Transfusion Post-admit CodeOther Foot Skin Problems: Diabetic Foot Ulcer CodeMDS Item M1040B1Narcolepsy and CataplexyMDS Item I80001Cystic FibrosisMDS Item I80001MDS Item O0100E21MDS Item I17001Special Treatments/Programs: Tracheostomy Care Post-admit CodeActive Diagnoses: Multi-Drug Resistant Organism (MDRO) CodeSpecial Treatments/Programs: Isolation Post-admit CodeMDS Item O0100M21Specified Hereditary Metabolic/Immune DisordersMDS Item I80001Morbid ObesityMDS Item I80001ContinuedNTA Score RangeNTA Case-Mix Group12 NA9–11NB6–8NC3–5ND1–2NE0NF** High level: K0710A2 3. 51% or more (while a resident)** Low level: K0710A2 2. 26–50% (while a resident) andK0710B2 2. 501cc/day or more (while a resident)NOTE: This document is intended to aid members in their review of the Patient-Driven Payment Model.Resources: FY 2019 SNF PPS Proposed Rulemaking and CMS draft PDPM Calculation Worksheet for SNFs. Allinformation regarding PDPM is subject to change pending final rulemaking. AANAC has made every attempt toensure the accuracy and reliability of the information provided. AANAC does not accept any responsibility orliability for the accuracy, content, and completeness of the information.Copyright 2018, American Association of Post-Acute Care Nursing, d/b/a American Association of Nurse Assessment Coordination. All Rights Reserved. AANAC.org5
Proposed Patient-Driven Payment Model: At-a-GlanceNon-Therapy Ancillary (NTA) Component (Continued)Condition/Extensive ServiceSourcePointsSpecial Treatments/Programs: Radiation Post-admit CodeMDS Item O0100B21Highest Stage of Unhealed Pressure Ulcer—Stage 4MDS Item M0300D11Psoriatic Arthropathy and Systemic SclerosisMDS Item I80001Chronic PancreatitisMDS Item I80001Proliferative Diabetic Retinopathy and Vitreous HemorrhageMDS Item I80001MDS Item M1040A,M1040C1MDS Item I80001MDS Item H0100D1MDS Item I80001Other Foot Skin Problems: Foot Infection Code, Other Open Lesion on FootCode, Except Diabetic Foot Ulcer Code (M1040B)Complications of Specified Implanted Device or GraftBladder and Bowel Appliances: Intermittent CatheterizationInflammatory Bowel DiseaseAseptic Necrosis of BoneMDS Item I80001MDS Item O0100D21Cardio-Respiratory Failure and ShockMDS Item I80001Myelodysplastic Syndromes and MyelofibrosisMDS Item I80001Systemic Lupus Erythematosus, Other Connective Tissue Disorders, andInflammatory SpondylopathiesMDS Item I80001Diabetic Retinopathy—Except Proliferative Diabetic Retinopathy andVitreous HemorrhageMDS Item I80001MDS Item K0510B21Severe Skin Burn or ConditionMDS Item I80001Intractable EpilepsyMDS Item I80001Active Diagnoses: Malnutrition CodeMDS Item I56001Disorders of Immunity—Except: RxCC97: Immune DisordersMDS Item I80001Cirrhosis of LiverMDS Item I80001MDS Item H0100C1Respiratory ArrestMDS Item I80001Pulmonary Fibrosis and Other Chronic Lung DisordersMDS Item I80001Special Treatments/Programs: Suctioning Post-admit CodeNutritional Approaches While a Resident: Feeding TubeBladder and Bowel Appliances: OstomyNTA Score RangeNTA Case-Mix Group12 NA9–11NB6–8NC3–5ND1–2NE0NFNOTE: This document is intended to aid members in their review of the Patient-Driven Payment Model.Resources: FY 2019 SNF PPS Proposed Rulemaking and CMS draft PDPM Calculation Worksheet for SNFs. Allinformation regarding PDPM is subject to change pending final rulemaking. AANAC has made every attempt toensure the accuracy and reliability of the information provided. AANAC does not accept any responsibility orliability for the accuracy, content, and completeness of the information.Copyright 2018, American Association of Post-Acute Care Nursing, d/b/a American Association of Nurse Assessment Coordination. All Rights Reserved. AANAC.org6
!INITIAL REVIEWOF THE PROPOSED PATIENT DRIVEN PAYMENT MODELPrepared by: Mark McDavid, OTR, RAC-CTModel’s Release Date: April 27, 2018 Initial Review Release Date: April 30, 2018Payment Model Background and Purpose of this Initial ReviewAs you may be aware, the Center for Medicare and Medicaid Services (CMS) publishedthe 266-page Prospective Payment System and Consolidated Billing for Skilled NursingFacilities (SNF) Proposed Rule for FY 2019 on Friday, April 27th. Included in the Ruleis the annual payment update for SNF PPS rates, updates to the SNF Value-BasedPurchasing Program and the SNF Quality Reporting Program, and the introduction ofthe Patient Driven Payment Model (PDPM). This document (the Proposed Rule) will bereferred to as CMS-1696-P. You can find the full version of the Proposed Rule ralregister.gov/2018-09015.pdf?utm campaign pi%20subscription%20mailing%20list&utm source federalregister.gov&utm medium email.In 2017, CMS published the Advanced Notice of Proposed Rule Making (ANPRM)which introduced the Resident Classification System – Version I (RCS-I) to theindustry. The RCS-I was developed as a result of the combined efforts of Acumen, aconsulting group hired by CMS, and an interdisciplinary technical expert panel.Following publication, CMS began accepting comments. RCS-I would fundamentallychange the way long-term care providers are reimbursed for the Part A post-acutecare skilled services. For that reason, many different entities had varying opinions onRCS-I. As recently as the February 2018 SNF Open Door Forum (ODF), CMS wascontinuing to solicit comments on RCS-I even though the comment period was closed.This signaled to many of us that CMS was not happy with RCS-I in its proposedpublished form. In that ODF, John Kane, SNF Team Lead at CMS, said that there wasno timeline for RCS-I. This, it turns out, foreshadowed RCS-I’s fate, which is that it hasbeen scrapped (at least in part) for a new model by a different name. Seagrove Rehab Partners, Initial Review PDPM 2018.Page 1 of 21
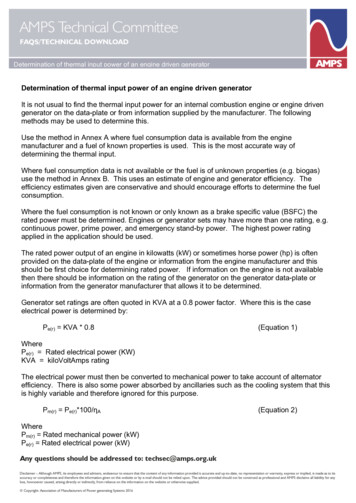
!This new proposed model, PDPM, was introduced Friday afternoon as part of thisyear’s SNF PPS Proposed Rule. This Initial Review was created after spending the lastseveral days reading through and studying this release. The purpose of this InitialReview document is to discuss the important components of the new PDPM in orderto educate readers on how SNFs will be reimbursed for Part A service if/when thisnew model goes from proposed to final rule.The New StructureOver the years, Medicare, MedPac, Congress, and various other stakeholders havebeen pushing to move the payment system away from counting therapy minutes toinstead reimbursing SNFs based on patient characteristics and/or patient outcomes.The new PDPM will pay for SNF PPS-care based on patient characteristics and not avolume of services provided. The current RUGs-IV system is a case-mix indexmaximizing system. In this system, as patients qualify for various RUGs (of the 66RUGs available), then the system automatically assigns the highest paying RUG foreach patient’s reimbursement. This is almost always a Rehab RUG (over 90 percent ofSNF PPS days were reimbursed via one of the Rehab RUGs per CMS-1696-P). In thenew PDPM, case-mix indexing will still play a role, but there are several differentcomponents that will contribute to the reimbursement that will ultimately equal thepatient’s daily rate, or per diem. They are: PT component, OT component, SLPcomponent, Nursing component, Non-Therapy Ancillary component, and the NonCase-Mix component. The first five of which will be case-mix adjusted based onpatient characteristics, and the last will be a flat rate.Components 1 and 2: Physical and Occupational Therapy Case-mixClassificationWhile Physical Therapy (PT) and Occupational Therapy (OT) will be separatecomponents, their case-mix adjustment will be calculated together. There will be twopatient characteristics used to determine the PT and OT case-mix classification. Theyare Clinical Category and Function Score. This process starts by using the clinicalreason for the patient’s skilled stay to then place that patient into one of ten clinicalcategories. PDPM outlines 10 clinical categories based on ICD-10-CM diagnoses codedat I8000 on the MDS. Table 14 from CMS-1696-P outlines those 10 categories: Seagrove Rehab Partners, Initial Review PDPM 2018.Page 2 of 21
!In the ANPRM document that outlined RCS-I last year, this was decreased to 5categories for figuring the PT/OT component. However, based on comments to lastyear’s publication, CMS has now further pared down the PT and OT components to 4categories in Table 15 of CMS-1696-P. These will be the 4 Clinical Categories drivingthe PT and OT case-mix classification:This clinical category would be determined by the ICD-10-CM code reported on thefirst item of I8000 from the MDS 3.0. A review of ICD-10-CM mapping to clinicalcategories vice-Payment/ Seagrove Rehab Partners, Initial Review PDPM 2018.Page 3 of 21
!SNFPPS/therapyresearch.html) will show that in some cases one ICD-10-CM will mapto more than one clinical category. The multiple categories are due, in part, to the factthat resident needs will differ depending on whether or not the resident receivedsurgical intervention while in the hospital immediately preceding this SNF stay.Typically, patients who have had surgery in the immediately preceding hospital staywill require extensive post-surgical nursing or rehabilitation care in the SNF. If thepatient did not receive a surgical procedure in the immediately preceding hospitalstay, then the resulting clinical category will be a non-surgical one. Here is theexample given in CMS-1696-P (pages 81-82):For example, certain wedge compression fractures that were treated with aninvasive surgical procedure such as a fusion during the prior inpatient staywould be categorized as Major Joint Replacement or Spinal Surgery, but if thesecases were not treated with a surgical procedure they would be categorized asNon-Surgical Orthopedic/Musculoskeletal. For residents who received a relatedsurgical procedure during the prior inpatient stay, a provider would need toindicate the type of surgical procedure performed for the resident to beappropriately classified under PDPM.In order to capture the inpatient surgical procedure, CMS is requiring providers touse an ICD-10-PCS code corresponding to the surgical procedure in the second line onI8000. If this proposal is finalized, then CMS will provide an ICD-10-PCS map ofprocedures to PDPM clinical categories.The next step in determining the PT and OT component case-mix score is todetermine the patient’s Function Score. Currently in the RUGs system (and previouslyproposed in RCS-I), CMS uses Section G: Functional Status (or the ADL score section ofthe MDS) to determine the patient’s functional score. In the new PDPM, CMS isproposing to use Section GG: Functional Abilities and Goals data to determine theFunction Score. Thus, the Functional Score will be determined by four late loss ADLsand two early loss ADLs. Specifically, that includes two bed mobility items, threetransfer items, one eating item, one toileting item, one oral hygiene item, and twowalking items. These were chosen as they are highly predictive of PT and OT costs Seagrove Rehab Partners, Initial Review PDPM 2018.Page 4 of 21
!per day. Tables 16, 17, and 18 of CMS-1696-P graphically show how these items willhelp produce the Function Score:The scores for each of the Section GG items above will be added together to get aTotal Function Score. This score will be used in Table 21 to further place the patientinto the appropriate Case-mix Classification Group. Seagrove Rehab Partners, Initial Review PDPM 2018.Page 5 of 21
!As you may recall, the RCS-I proposal included cognitive status as a determinant forthe PT/OT case-mix classification. Due to comments in response to ANPRM, CMS hassince removed cognitive status as a determinant of the PT and OT case-mixclassification. CMS uses a Classification and Regression Trees (CART) algorithm tohelp determine the resident groups and cognition was included as an independentvariable in the CART analysis. For more information on the CART analysis refer topage 93 of the CMS-1696-P document.Taking 1) Primary clinical reason for SNF stay and 2) Function Score into account, wecan now classify a patient into a PT and OT Case-Mix Classification Group. Table 21graphically shows the breakdown of each PT and OT Case-mix Classification Group: Seagrove Rehab Partners, Initial Review PDPM 2018.Page 6 of 21
!Component 3: SLP Case-mix ClassificationSpeech Language Pathology case-mix classification will follow the same methodologyas the PT and OT classification. Initially, it will be determined if the primary clinicalreason for the SNF stay is either “Acute Neurologic” or “Non-Neurologic”. A quickreview of Table 14 above shows that “Acute Neurologic” has its own category and“Non-Neurologic” would be comprised of the 9 remaining categories.The second characteristic to be identified for the SLP Case-mix Classification is thepresence of a swallowing disorder or mechanically altered diet. It is noted that thereis increased provider cost for residents with either a mechanically altered diet or aswallowing disorder. And a further increase in cost if the resident has both.Therefore, “both”, “either”, or “neither” are used as it relates to swallowing disorderand mechanically altered diet when determining the SLP Case-mix Classification.These would be identified by responses to K0100Z (swallowing disorder) and K0510C2(mechanically-altered diet) on the MDS.The third characteristic to be identified for the SLP Case-mix Classification is cognitivestatus or whether or not the resident had a SLP-related comorbidity present. Table 22shows the SLP-related Comorbidities:As with the RCS-I ANPRM proposal, CMS is proposing to use the Cognitive FunctionalScale which is a combination of the Brief Interview for Mental Status (BIMS) andCognitive Performance Scale (CPS) to identify cognitive status for the SLP Case-mixClassification. Due to comments to the ANPRM proposal, CMS has moved a score of“0” on the CPS to equal “Cognitively Intact” vs. “Mildly Impaired”. Table 20graphically shows how cognition level is chosen using these two tools: Seagrove Rehab Partners, Initial Review PDPM 2018.Page 7 of 21
!Finally, CMS was able to decrease the number of SLP Case-mix Classification Groupsfrom 18 (in the ANPRM proposal) to 12 for PDPM purposes. Table 23 shows thebreakdown of how SLP Case-mix Classification Groups will be assigned:Component 4: Nursing Case-Mix ClassificationCMS is proposing to identify the Nursing Case-Mix Classification based on a modifiedtraditional RUG-IV methodology and decreasing the possible RUGs from 43 to 25. Inthe traditional RUG-IV nursing RUG methodology, the ADL score was derived from Seagrove Rehab Partners, Initial Review PDPM 2018.Page 8 of 21
!Section G of the MDS. Under PDPM, CMS is proposing to use Section GG to determine aFunction Score as outlined below in tables 24 and 25:Decreasing the number of RUG options from 43 to 25 was accomplished by collapsingcase-mix groups that had contiguous ADL scores when those RUGs were defined bysimilar clinical traits. Table 26 outlines which RUGs were collapsed and identifies theNursing case-mix index score: Seagrove Rehab Partners, Initial Review PDPM 2018.Page 9 of 21
! Seagrove Rehab Partners, Initial Review PDPM 2018.Page 10 of 21
!HIV/AIDS add-onCMS explained that there was a significant increase in nursing cost to provide carefor residents with HIV/AIDS. To compensate facilities for caring for these residents,CMS proposes an 18% increase in the nursing component. This increase would beapplied based on the presence of ICD-10-CM code B20 on the SNF claim.Component 5: Non-Therapy AncillaryNon-Therapy Ancillary (NTA) scoring is fairly straight forward. Using Table 27 as areference, if the resident has the condition/extensive service on the left column fromthe noted source location, then sum the points identified on the right together to getthe total NTA score: Seagrove Rehab Partners, Initial Review PDPM 2018.Page 11 of 21
!Based on the NTA scores summed from the conditions/extensive services on Table 27,Table 28 reflects the NTA Case-Mix Classification Groups: Seagrove Rehab Partners, Initial Review PDPM 2018.Page 12 of 21
!Component 6: Non Case-Mix ComponentThe final piece of the total per diem is the non case-mix component. This flat-ratecomponent (that is not case-mix adjusted) is for covering room and board, capitalexpenses, and administrative overhead.Combining all 6 components above (PT, OT, SLP, Nursing, NTA, Non Case-Mix) willresult in the base daily rate for that patient. Multiplying each component’s base rateby its respective case-mix index will return the facility’s daily rate for that specificresident upon admission. As will be discussed below, the Variable Per DiemAdjustment Factor comes in play with PT, OT and the NTA components. Thesecomponents will be decreased at various intervals during the resident’s stay.Variable Per Diem Adjustment FactorsDiscussed in both the ANPRM and CSM-1696-P documents, is Medicare’s discovery ofdecreasing costs of PT, OT, and NTA the longer the resident stays in the facility. Thisdiscussion can be found throughout the CMS-1696-P document. Due to the decreasingcosts during a resident stay, CMS proposes the Variable Per Diem Adjustment Factor.For PT and OT, the PDPM proposes that the facility be reimbursed the full base ratemultiplied by the the case-mix index, for each resident for PPS days 1-20. Then,starting on day 21, a decreasing adjustment factor of 2% every 7 PPS days would beapplied. Days 1-20: PT base rate x CMI x 1.00 (the adjustment factor) PT portion ofthe per diem Days 21-27: PT base rate x CMI x .98 (the initial adjustment factor) PTportion of the per diem.This decrease would continue for both PT and OT every 7 days as outlined in Table 30until the patient is discharged. It is worth noting that if the resident stayed all 100days, the PT and OT components would be reimbursed at 76% of their initial rate fordays 98-100. Seagrove Rehab Partners, Initial Review PDPM 2018.Page 13 of 21
!For the NTA, the proposed adjustment factor starts at a multiple of 3 and is reduced toa multiple of 1 on day 4 as outlined below:Resident Assessment Instrument: MDS, Version 3 Proposed ChangesAs CMS is no longer using therapy minutes to determine reimbursement, any changesin a resident’s therapy minutes will no longer impact reimbursement, therefore, CMSis proposing a new MDS Assessment schedule. The new PPS MDS schedule isrepresented in Table 33: Seagrove Rehab Partners, Initial Review PDPM 2018.Page 14 of 21
!Interim Payment Assessment (IPA)An IPA would be required to be completed where the following two criteria are met(page 140):(1) There is a change in the resident’s classification in at least one of the first tierclassification criteria for any of the components under the proposed PDPM(which are those clinical or nursing payment criteria identified in the firstcolumn in Tables 21, 23, 26, and 27) such that the resident would be classifiedinto a classification group for that component that differs from that provided bythe 5-day scheduled PPS assessment, and the change in classification groupresults in a change in payment either in one particular payment component orin the overall payment for the resident; and(2) The change(s) are such that the resident would not be expected to return tohis or her original clinical status within a 14-day period.In addition, we propose that the Assessment Reference Date (ARD) for the IPAwould be no later than 14 days after a change in a resident’s first tierclassification criteria is identified. The IPA is meant to capture substantialchanges to a resident’s clinical condition and not every day, frequent changes.We believe 14 days gives the facility an adequate amount of time to determinewhether the changes identified are in fact routine or substantial.In last year’s ANPRM document, CMS proposed keeping the Significant Changeassessment and is now proposing that the Significant Change assessment be replacedby the IPA.CMS has also proposed a change in the rules governing when a PPS DischargeAssessment is to be completed and the Assessment’s Item Set. Currently, the PPSDischarge Assessment is completed when a patient is discharged from Part A andcontinues to stay in the facility. CMS is proposing the completion of the PPS DischargeAssessment for all residents who are discharged from PPS; whether they are actuallydischarged from the facility or stay long term. Additionally, CMS is proposing tochange the Discharge Assessment Item Set to include a modified Section O. Seagrove Rehab Partners, Initial Review PDPM 2018.Page 15 of 21
!In CMS-1696-P, CMS discusses the comments received in response to the ANPRMpublication where stakeholders are concerned about the lack of oversight andmonitoring of therapy provisions throughout the stay of the resident. Therefore, CMSnow proposes to monitor therapy provisions throughout the stay by adding Table 35to Section O on the SNF PPS Discharge Assessment:It appears that the added “Total” items (total individual minutes, total concurrentminutes, total group minutes, total days) may be referring to totals throughout theresident’s stay and not just in the 7-day look-back period. As of this writing, this hasnot been confirmed and the CMS-1696-P document is not explicitly clear on this issue. Seagrove Rehab Partners, Initial Review PDPM 2018.Page 16 of 21
!Grace DaysNote: In the current MDS 3.0, RUGs-IV Model the 5-day assessment window is days 1-5with allowable grace days 6-8. CMS is proposing the removal of the label “Grace Days”from the 5-day assessment window. The scheduled assessment window for the 5-dayassessment will now be identified as days 1-8 of the PPS stay.Therapy Provision Policy ChangesEven though we will no longer be using therapy days, modes, and minutes todetermine payment, CMS will continue to track these items and will be placingadditional constraints on therapy providers. It is expected that the majority oftherapy provided will be in the individual mode. To that end, CMS is expanding thegroup limitation to include concurrent therapy as well. That is, CMS is proposinglimiting group and c
Apr 27, 2018 · Active Diagnoses: Asthma COPD Chronic Lung Disease Code MDS Item I6200 2 Bone/Joint/Muscle Infections/Necrosis—Except Aseptic Necrosis of Bone MDS Item I8000 2 Chronic Myeloid Leukemia MDS Item I8000 2 Wound Infection Code MDS Item I2500 2 Active Diagnoses: Diabetes Mellitus