Transcription
Obstructive Pulmonary PhysiologyFrom the Imaging Perspective:Balloons, Airway Inflammation orDynamic CollapseMarc V. Gosselin, MDVision RadiologyOHSU School of Medicine
DisclosuresLecture for Genentech on Interstitial lungdisease imaging for Education onlyNo drug promotion or researchinvolvement
Lecture ObjectivesIntroduce the differential of ‘COPD’Use of imaging to demonstrate theunderlying pathology and help explain theclinical manifestationClinical ‘Red Flags’ to alert the possiblepresence of other common, but often notclinically diagnosed cause of ‘COPD’“Where all think alike, no one thinksvery much” Walter Lippmann
68 yo female with Worsening dyspnea over 12months: 3 “COPD” admissions
Dyspnea: Started 8 Years Ago - Diagnosedwith COPD/Emphysema, then lost Insurance coverage
Normal Thin Section CT
Normal Thin Section CT: Cardiac Motion
Normal Inspiration and Expiration
‘COPD’ Algorithm “Thinking”Chronic obstructive pulmonary disease (COPD)is a general term lumping emphysema, chronicbronchitis and asthma togetherCOPD leads to reflexive treatment algorithmsDisadvantages of using the term COPD: Other obstructive conditions are often over-looked.Pathologic and physiologic mechanisms of thesediseases are different.Prognosis and treatment are disease specific.
White Zinfandel is NOT a wine!
Misconceptions about ‘COPD’ arevery common:‘Hyperinflation of lungs with smokinghistory means emphysema’(Pulmonologist)‘Lungs that extend below 10th ribs is hyperinflated and represents COPD’((Pulmonologist & Radiologist)‘Emphysema is not diagnosed withimaging, it is a PFT diagnosis!’(Pulmonologist)
Misconceptions about ‘COPD’ areoften taught with confidence:‘Patient has emphysema, she was exposedto second hand smoke’ The response by apulmonologist when I mentioned the patient likely hasanother cause for their obstructive lung disease given herrecurrent admissions and not improving on treatment.‘Hyperinflated lungs consistent withEmphysema’ – Radiology report and agreement byphysician in a patient without any smoking history. Losttheir insurance ‘For lying about smoking’“We can be Absolutely Certain Only aboutThings We Do Not Understand.” Eric Hoffer
“The Greatest Obstacleto Discovery is notIgnorance, but theIllusion of Knowledge.”Daniel J. Boorstin
35 yo non-smokingfemale withpersistent dyspnea& some wheezingfor 2 years –Clinical Diagnosis:‘Poorly ResponsiveAsthma’
“COPD”: What You Should Be Considering6 different pathologies can manifestwith severe obstructive disease:-Emphysema (‘Balloons’)-Chronic Bronchitis-Asthma-Tracheobronchomalcia (‘Dynamic’)-Constrictive Bronchiolitis (‘Balloons’)-Bronchiectasis (via Constrictive bronchiolitis)The persistence or recurrence of symptoms shouldalert you that a diagnosis is being missed
Obstructive Pulmonary DiseaseInflammatory: Chronic bronchitis(Hypoxic), bronchiectasis and asthma(post viral or antigenic) (Shunt-like)Balloons: Space occupying diseases:(Increase in ‘Dead Space’) Emphysemaand Constrictive bronchiolitisDynamic collapse:Tracheobronchomalacia and/or Dynamicredundant posterior wall collapse ( 70%)
What is the V/Q abnormality withShunt Physiology?Persistent perfusion with decreased orabsent ventilation ShuntThis induces hypoxiaChronic Bronchitis is an example - Hencethe term ‘Blue Bloater’Also why Pulmonary Hypertension (ChronicHypoxia induced) occurs so commonly withChronic Bronchitis
What is Dead Space Physiology?Persistent ventilation with decreased/absentperfusionNo to mild hypoxiaPulmonary embolus is a perfect example of aDead Space PhysiologyEmphysema (‘Pink Puffer’), ConstrictiveBronchiolitis and Tracheobronchomalaciaoften maintain a relatively balanced V/Q ratioat the alveolar levelsQuinn & Rizzo. Anatomy, Anatomic 2016/ Dec 2018
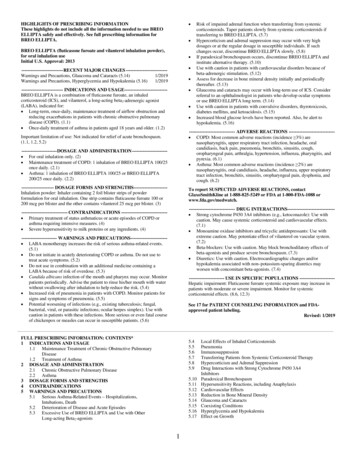
Radiographic Signs of HyperinflationFlat diaphragm (Increased trapped RV)Sterno-diaphragmatic angle approaches90 degrees on lateralIncreased width of retrosternal air spaceIncreased AP diameterNote: Lungs extending below 10th rib isNOT a reliable criteria – ‘People are likeSnowflakes’
Normal LungsHyperinflation
Is There Hyperinflation?
Emphysema: Radiographic ImagingVascular attenuation and depletion withincreasing branch angles approaching 90degreesHilum are ‘pushed’ inferior and medialVascular crowding along the medial andlower lobesCheck pulmonary artery size if advanced(Pulmonary hypertension)Cachexia may be present (Reason?)
Radiograph Characteristic forAdvanced Emphysema
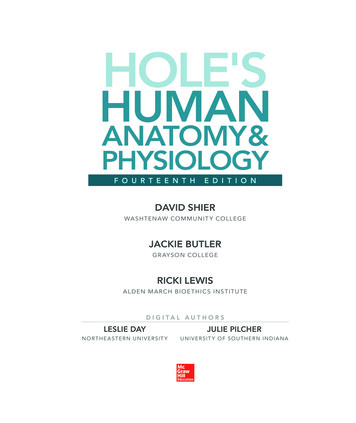
Emphysema: CT ImagingDifferent types such as Centrilobular (mostcommon), Panlobular, Bullous andParaseptalNo visible wall and has acentral/peripheral ‘Dot’ representing theresidual Central bronchovascular bundleCysts have no central/peripheral ‘Dot’ andoften have walls
LAM (Cysts)Emphysema
Hypothetical mechanism onhow the expansion occursWhen filled It is Non-dynamic
Peripheral Bullous Emphysema
Minimal Dynamic Changes:Increase in End-Tidal Residual Volume
When a lung withemphysema isremoved at autopsy,the lung collapses,but not theemphysema
Consolidation & GroundGlass looks heterogeneouswith Emphysema
Why these ‘holes’ withedema or pneumonia?
Nothing gets in orout like Non-dynamicBalloons
Increase in End-Tidal Residual VolumeWhat is The Surgical Therapy Called?
Why Cachexia?
Where all think alike, noone thinks very much.Littermann
68 yo female with Worsening dyspnea over 12months: 3 “COPD” admissions
68 year old femalewith AdvancedRheumatoidArthritis:Worsening dyspneaand hypoxia over 2years with recurrentadmissions for“COPD”exacerbations
InspirationIs There Emphysema?ExpirationIs this RA-associatedConstrictive Bronchiolitis?
Follicular Bronchiolitis AND TracheobronchomalaciaHow Well Does the‘COPD’ StandardTherapy Work?
The patient states thatSteroids did not seem tohelp with her breathing.Albuterol had no effect.She did mention that thelittle plastic FEV1 portabledevice seemed to help themost. Blows into it againstresistance A form ofPEEP. Much like breathingthrough her pursed lips
TracheobronchomalaciaCollapsing ( 70%) of the Trachea and/orBronchi with global air trappingCartilage weaknessExcessive Dynamic Tracheal collapse (EDTC)Pursed lip breathingVocal cord dysfunctionChronic cough, often ‘difficulty clearingsecretions’, Dyspnea, Exercise intolerance,wheezing
Diagnosis: Slowly ResolvingMultifocal Pneumonia and “COPD”30 Pack Year Smoking HistoryMore Generalized Lung/Lobar Obstruction
Tracheobronchomalacia‘Poorly responsive’ Asthma/COPDRecurrent ‘COPD’ exacerbations (Nottreating the correct diagnosis)Associations:Chronic Steroids (Autoimmune diseases)Constrictive Bronchiolitis Tracheobronchiomalacia(Often secondary to Chronic Steroids)Sleep Apnea
From: Husta, B et al. Tracheobaronchopathy From InhaledCorticosteroids. Chest 2017; 152(6):1296-1305Inhaled corticosteroids – ‘ICS’
CTA Shortness of Breath(Pursed lip Breathing)
Incidence of TracheobronchomalaciaTracheobronchomalacia Incidence on ALLPulmonary CTA’s is about 1 out of 10Red Flag Indications: Shortness of Breath,Persistent cough, unable to clear secretions,‘COPD’, Severe ‘Asthma’Need expiratory imaging or Respiratory motionduring exam2 out of 10 with ‘COPD’ diagnosis7 out of 10 with ‘Severe Asthma’ diagnosisHasegawa et al: AJR December 2003;181:1505–1509
CTA for Shortness of Breath:Tracheobronchomalacia isthe problem – Improvedquickly with BiPap(Also: Patient complained couldnot cough up secretions)
“Education is theprogression from acocky ignorance to amiserable uncertainty.”Mark Twain
Dyspnea: Started 8 Years AgoDiagnosed with COPD/Emphysema & Lost InsuranceIs This Emphysema?
58 year oldLDS womenIs thereEmphysema?
InspirationExpiration
Constrictive Bronchiolitis(AKA: Bronchiolitis Obliterans)Injury occurred after her RespiratoryInfection 8 Years Ago
‘BO’ is CommonBut NOTcommonlydiagnosed!
41 year old female with persistent dyspnea,difficulty with exercise and weight loss overa 2 year period.14 pack/year smoking history.9/20171/2019
Dyspnea started in late 2017 after wakingup in a house fire accident. Diagnosis?
Constrictive BronchiolitisPathology: It is a Permanent Scar of theRespiratory or Terminal bronchiolesEtiology: Whatever induces injury withnecrosis to the bronchial mucosaCommon Causes: Airway infections(Especially typical viral and mycoplasma),Bronchiectasis, Smoke inhalation, Drugtoxicity, Transplant rejection & Autoimmunediseases Krishna R, Bhimji SS. Bronchiolitis Obliterans (ConstrictiveBronchiolitis) [Updated 2018 Oct 27]. In: StatPearls [Internet].Available from: https://www.ncbi.nlm.nih.gov/books/NBK441865/
Mosaic Lung Attenuation: Look at thevessels - Patchy Perfusion Small AirwaysDisease vs. Pulmonary Hypertension
Constrictive Bronchiolitis: SimilarPhysiology to Emphysema, Often with Less Hypoxia
Constrictive BronchiolitisSymptoms: Persistent Dyspnea/cough notresponsive to steroids/albuterolNot episodic (Asthma)Clue: OFTEN a patient can tell you WHEN theirbreathing difficulties beganExample: Post RSV infection 2 yo – ‘Increaserisk of Asthma, but often grows out of it’ – Is itAsthma? Why do they improve with age?What if the child was a 15 yo with mycoplasma?
Constrictive BronchiolitisImaging: Patchy areas of air trapping onexpiration thin section CT imagingContrast with Tracheobronchomalacia whichhas more global areas of air trapping since theobstruction is more centralConfounding: Bronchomalacia involving themore segmental bronchi can be more difficult todistinguishNote: Constrictive Bronchiolitis andTracheobronchomalacia can coexist (Especially if onChronic Steroids for misdiagnosed Constrictive Bronchiolitis)
Right Transplanted Lung: ConstrictiveBronchiolitis (Left Native Lung: Emphysema)
Bronchiectasis with air-trapping isoften secondary to Constrictivebronchiolitis
Cystic Fibrosis: 40 yo withprogressive worsening dyspnea
Cystic Fibrosis and Constrictive BronchiolitisConstrictive Bronchiolitis is an expectedcomplication of CF patientsEvolving as a common cause of mortalityTry to mention its presence and/or extentin your reportsLook for it on all other chronic airway diseases,especially with bronchiectasisHarris et al. Constrictive Bronchiolitis in Cystic Fibrosis Adolescent withrefectory pulmonary decline. Ann Am thorac Soc. 2016 Dec; 13(12) 2174-2183
42 yo Male WithRecurrent “Bronchitis”Localized versusWidespread Distributionof Bronchiectasis
75 yo Female:Chronic CoughDiagnosis?Why are the vesselsattenuated within areasof bronchiectasis?
“Signet” or“Solitaire” Ring SignOr ACabochonRing?
Clinical ‘Red Flags’Persistence or Recurrence of symptoms &signs – i.e. Multiple ‘COPD’ admissionsPatient can identify time period or eventwhen the breathing difficulties beganBreathing through pursed lips or aconcurrent diagnosis of “vocal corddysfunction”Do not fully respond to steroid/albuteroltherapy
Truth pass through 3 stages:First, It is ridiculed. Second, It isviolently opposed. Third, It iseventually accepted as being SelfEvident.Arthur Schopenhauer
Thank You – mgosselin@visionradiology.comor Gosselin@OHSU.edu
Question 1: When you see severetracheobronchomalacia with global airtrapping in a patient with shortness of breath,what recommendation may be a useful?A. More steroids would helpB. Antibiotics should be givenC. A trial of Bipap should be givenD. Bronchodilators are often usefulE. No suggestion since they know how totreat ‘COPD’
Question 1: When you see severetracheobronchomalacia with global air-trapping in apatient with shortness of breath, what recommendationmay be a useful?Answer is D. A trial of Bipap should begivenThe dynamic collapse of tracheobronchomalaciaoften responds quickly to positive pressure. Apatient’s shortness of breath will often improvewhen this is the issueMore steroids won’t help and will very likely haveadverse consequences with tracheobronchomalacia.Best to try and wean them off all steroids. Antibotics ifinfected only. Bronchodilators do not help with thecollapse. The vast majority of doctors do not even knowabout tracheomalacia, inform them about it.
Question 2: Which process is an exampleof Shunt Physiology and often Hypoxic?A. Chronic BronchitisB. EmphysemaC. Constrictive bronchiolitisD. Pulmonary embolusE. Tracheobronchomalacia
Question 2: Which process is an exampleof Shunt Physiology and often Hypoxic?Answer is A: Chronic Bronchitis.Persistent perfusion with altered/decreasedventilation Shunt. This induces hypoxia(Hence the term ‘Blue Bloater’)Pulmonary embolus is an example of a DeadSpace Physiology: Persistent ventilation withdecreased/absent perfusion (Not hypoxic)Emphysema, Tracheobronchomalacia andConstrictive Bronchiolitis often maintain the V/Qratio at the alveolar levels
Question 3: What is a strong clinical cluethat a patient’s Obstructive PulmonaryPhysiology is from Constrictive Bronchiolitis?A. Long smoking historyB. There is an identifiable point in timewhen the breathing difficulties developedC. Chronic steroid useD. Pursed lip breathingE. There are no good clinical clues, that iswhy there is imaging
Question 3: What is a strong clinical cluethat a patient’s Obstructive PulmonaryPhysiology is from Constrictive Bronchiolitis?Answer is B - There is an identifiable pointin time when the breathing difficultiesdevelopedThis clue in the history is a strong predictor of constrictivebronchiolitis, an injury occurred with resultant scarring downof large areas of bronchioles.Pursed lip breathing favors a dynamic collapse of the centralairways. Smoking favors emphysema/chronic bronchitis.Chronic steroids are associated with Constrictive Bronchiolitis,because it is misdiagnosed as ‘Resistant Asthma’ or ‘COPD’Krishna R, Bhimji SS. Bronchiolitis Obliterans 2018 Oct 27] 1865/
Question 4: Which Imaging finding, in apatient with an obstructive pulmonary process,suggests it may NOT be due to Emphysema?A. CT shows widespread 10mm lucencies with acentral/peripheral ‘Dot’B. Radiograph shows the Hilum displaced inferiorlyand mediallyC. Radiographic vascular crowding medially andlower lobesD. Uniform Pulmonary Vessels showing most branchangles of 50 degrees throughout the lungsE. Flattening of the diaphragm
Question 4: Which Imaging finding, in a patientwith an obstructive pulmonary process,suggests it may NOT be due to Emphysema?Answer is D – Uniform PulmonaryVessels showing most branch angles 50 degrees throughout the lungsVascular attenuation & depletion causeswidening branch angles, especially inupper lobes. This is associated withEmphysema much more than the otheretiologies.Takahashi et al: Imaging of Pulmonary Emphysema. International Journal of COPD2008:3(2) 193-204
Question 5: Incidence ofTracheobronchomalacia on AllCTA’s for PE is approximately A. 1 out of 200B. 1 out of 100C. 1 out of 50D. 1 out of 10E. 1 out of 2
Question 5: Incidence ofTracheobronchomalacia on All CTA’s for PE isapproximately Answer D: 1 out of 10There is not a lot of data on the trueincidence, but important to recognize that itis a common finding, especially with SOB.Make it a routine part of your CTAevaluation (Much more likely to find thisthan a PE!)Red Flags: SHORTNESS OF BREATH, persistentcough, unable to clear secretions, pursed lip breathing,‘COPD’, Persistent or Severe ‘Asthma’Hasegawa et al: AJR December 2003;181:1505–1509
Enjoy Some Fine Non-WhiteZinfandel Wine Tonight!
Obstructive Pulmonary Physiology From the Imaging Perspective: Balloons, Airway Inflammation