Transcription
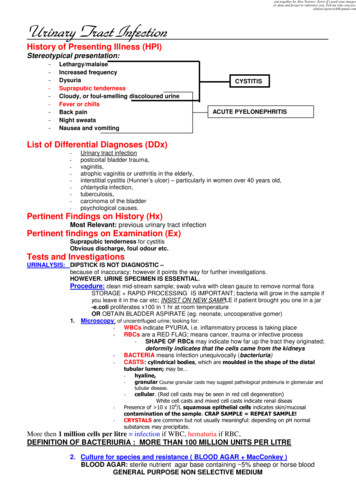
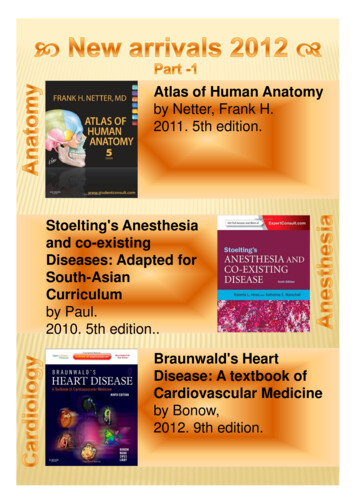
Chapter 7Anatomy and Physiology.Chapter 7: Anatomy and PhysiologyA thorough understanding of dental and oralanatomy and physiology is essential for allmembers of the veterinary dental team. Youmust know what is normal and be able to quicklyrecognize the abnormal. Often, an unsedatedanimal will allow you only a brief look in themouth and so you must be able to take a mentalsnap-shot and notice subtle indicators of disease.Much of this ability will come with practice, butit starts here, by studying comparative dentalanatomy and becoming familiar with thelanguage of dentistry. This is but a briefintroduction.In multi-rooted teeth there is a place where theroots come together to join the rest of the tooth.This crotch-like area is called the furcation.Each tooth has its own name, and there areseveral systems that have been used. TheAmerican Veterinary Dental College, AmericanVeterinary Dental Society and Academy ofVeterinary Dentistry have all agreed to recognizetwo systems.In the Anatomical System, I, C, P and M denotepermanent incisor, canine, premolar and molarrespectively. Primary teeth are denoted by lowercase letters (i, c, p, and m). The specific tooth isindicated by an Arabic numeral and the quadrantby the location of the numeral with respect to theletter. Therefore, the right upper third permanentpremolar is referred to as P3; P for permanentpremolar, 3 for third and placed superscript tothe right of the letter to indicate the rightmaxillary quadrant. Supernumerary teeth areidentified by an S or s preceding the appropriateupper or lower case letter. So, s2i would be asupernumerary left mandibular second primaryincisor.I had wanted to write this as two separatechapters, but the two subjects are so intimatelyintertwined that I could not discuss one withoutdiscussing the other.TerminologyIn dentistry, attention to detail is essential.Nowhere more so than in charting. We must allkeep accurate records of findings and treatmentsif we are to communicate with other staffmembers and the owners and to assess theprogress of any condition. To make this taskeasier, there are a number of terms to describeparts of the mouth and teeth as well as todescribe which tooth is being discussed.The anatomic system works well visually but is abit clumsy for verbal communication and doesnot lend itself easily to computerized records. Inthese instances, the Modified Triadan System isEach tooth has a crown and a root. The tip of theroot is the apex so moving toward the tip of theroot is to move apically. Around the apex is theperi-apical region. Where the root and the crownmeet is the neck or cervical region of the tooth. Itis in this area that the enamel covering of thecrown ends at the cemento-enamel junction. Thecrown of the tooth is that portion covered byenamel. As you travel from the neck to the tip orcusp of the crown, you are traveling coronally.The face of the tooth towards the lips or cheek isthe labial or buccal aspect. 'Labial' is usuallyreserved for incisors and canines and 'buccal' isused for the 'cheek teeth'. The surfaces facing thetongue and palate are the lingual and palatalaspects respectively.The surface of the tooth closest to the toothbehind it is the distal aspect and the surfaceclosest to the tooth in front is the mesial aspect.With the incisors, being arranged more mediolateral than rostro-distal, call the surface closestto the facial mid-line mesial and the surfacefurthest from the mid-line distal.Figure #7.1. The names of the faces of the teeth.24
Chapter 7Anatomy and Physiology.The Toothuseful. It refers to each tooth by a three-digitnumber. The first numeral indicates the quadrantand the next two tell which tooth in the quadrantas counted from the midline to distal.The tooth is the basic unit of concern indentistry. Therefore, any study of dentistry muststart with an understanding of the anatomy andphysiology of the tooth. In veterinary dentistry,there is a wide range of tooth types andmorphologies, but this discussion will focus on asimple, single rooted tooth as might be found inhumans, dogs and cats.The number sequence of the quadrants is;permanent upper right 1, permanent upper left 2, permanent lower left 3, permanent lowerright 4, primary upper right 5, primary upperleft 6, primary lower left 7, and primarylower right 8. In each quadrant the first incisoris always 01, the second is 02 and so on. So theright upper fourth permanent premolar is 108,the left mandibular third primary premolar is 707and the right lower permanent third molar is 411.Upper Right Permanent 1Upper left permanent 2Upper Right Primary 5Upper left primary 6Lower Right Permanent 4Lower Left Permanent 3Lower Right Primary 8Lower Left Primary 7Each tooth has a crown (the portion above thenormal gingival margin) and a root (the portionbelow the normal gingival margin). The bulk ofa mature tooth is composed of dentin. The dentinof the crown is covered by enamel and the dentinof the root is covered by cementum. Thecementoenamel junction marks the transitionfrom root to crown and is known as the neck,cervix or cervical region of the tooth. Inside thedentin of the root and the crown is a hollowchamber filled with the soft tissue known aspulp. This chamber is referred to as the pulpchamber in the crown and the root canal withinthe root of the tooth.When it comes to the cat, things are not asstraight forward. The cat is missing the upperfirst and the lower first and second premolarteeth and so have second, third and fourth upperand third and fourth lower premolars only. Eachquadrant has only one molar. When counting theteeth in the right upper quadrant, with tooth 105absent, the sequence would go 101, 102, 103,104, 106, 107, 108, 109. For the lower leftquadrant, with the first and second premolarmissing, the sequence goes 301, 302, 303, 304,307, 308, 309. The sample dental in Appendix Dshow the full adult dentition of the dog and catand the primary dentition for the dog, with eachtooth numbered for reference. Interestingly, mostfelines, from domestic cats up to lions and tigershave the same dental formula.In a multi-rooted tooth, the crotch-like areawhere the roots diverge from the crown is knownas the furcation. This is a very importantlandmark with respect to periodontal disease.Once gingival recession, bone loss or pocketformation expose the furcation, getting andkeeping the tooth thoroughly clean becomesmuch more challenging.The roots of the teeth reside in depressions in themaxillary, incisive and mandibular bones, knownas the alveoli. The walls of the alveolus arecomposed of dense, cortical bone known as thelamina dura or alveolar bone proper. Betweenthe cementum of the root and the lamina dura isthe periodontal ligament space, occupies by theperiodontal ligament. This ligament holds thetooth in place while affording some movement,thus acting as a shock absorber.The Rule of 4 and 9 states that every toothending in 04 is a canine tooth and every toothending in 09 is the first molar. The rule of 9 and4 makes it easy to remember the numbers of eachtooth without having to go back to the firstincisor and count around to the tooth in question.For example, tooth 107 has to be a premolarbecause it is greater than 104 (the canine) andless than 109 (the first molar). When identifyinga tooth, you can start to count from the midline(at 01), at the canine (at 04) or at the first molar(at 09), so you have three known landmarks fororientation. This rule and the modified Triadansystem work perfectly for every quadrupedmammal, so long as teeth that are absent get leftout of the counting sequence.EnamelEnamel is the hardest tissue in the mammalianbody. It is composed of crystals ofhydroxyapatite arranged in prisms roughlyperpendicular to the junction with the underlyingdentin. The closely packed crystals occupy 88%of the volume of the enamel, the remaining 12%being water and organic material. By weight,enamel is 96% mineral. It is acellular andconsidered non-living.25
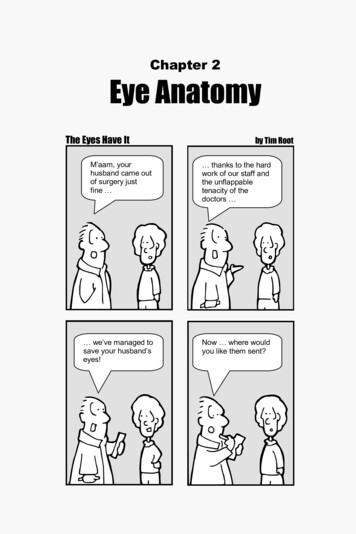
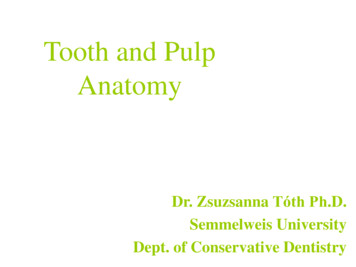
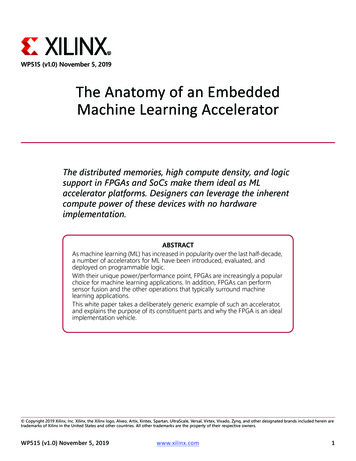
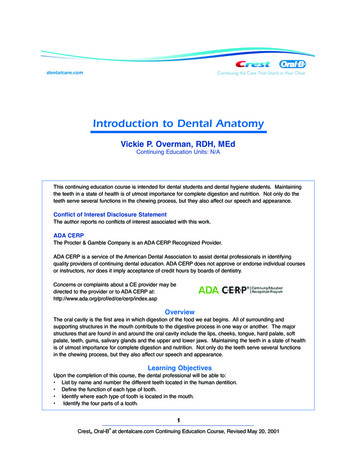
Chapter 7Anatomy and Physiology.Figure #7.2. Line drawing of the right mandibular first molar (tooth 409) in a dog. Note how the shape ofthe pulp chamber mimics the shape of the crown, such that an innocent looking chip fracture of a cuspmay still cause a pulp exposure or a near exposure.oral cavity, enamel is lost gradually (or rapidly ifthe animal has a chewing vice) to chemical andmechanical forces.Anything that disrupts the delicate ameloblastsduring enamel production will result in defectiveenamel, which may be very weak and brittle.This defective enamel may be present at eruptionbut will soon be lost to abrasive forces. Thisleaves an area of exposed dentin and roughmargins to the surrounding enamel. This enamelhypocalcification may affect a spot on a singletooth if the insult is localized (e.g., infectionfrom a fractured deciduous tooth, iatrogenic fromcareless deciduous tooth extraction, bruisingfrom local facial trauma). Many systemicconditions, such as hypoproteinemia, pyrexia,epitheliotrophic virus infection can causewidespread enamel hypocalcification on theareas of the teeth that are undergoingamelogenesis during the time of the illness. Thisoften appears as a band of abnormal enamelencircling the teeth with the enamel producedbefore the illness and that produced after theillness looking perfectly normal.Figure #7.3. This radiograph of the maxillary incisorsof a young dog shows abnormal root development.Clinically, the dog had enamel hypocalcification andthe teeth were loose.Enamel is formed by ameloblasts during toothdevelopment. Amelogenesis (enamel production)stops prior to tooth eruption and no more enamelis produced. Once the tooth has erupted into theSerious systemic illnesses may also causehypoplasia of the root structure of the permanentteeth and so affected animals require26
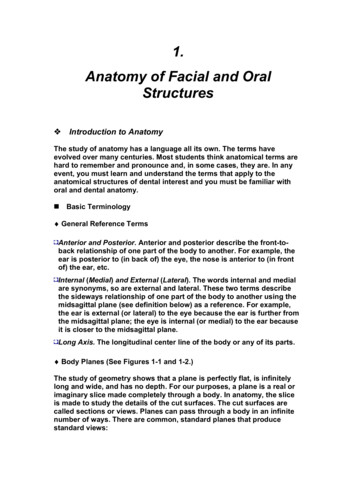
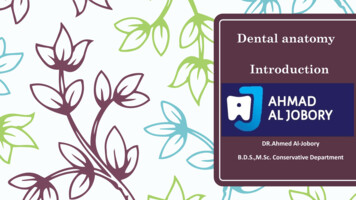
Chapter 7Anatomy and Physiology.radiographic assessment. Genetic abnormalitiessuch as dentinogenesis imperfecta also result inabnormal root structure development.colour, compared to the stark white of normalenamel. Dentin is roughly 72% mineral, 18%organic matter (mostly collagen) and 10% waterby weight.Enamel hypoplasia is a different condition inwhich the enamel produced is properlymineralized and is shiny and hard like normalenamel, but it is thinner. Often, there is aterracing effect as one proceeds from the normalenamel, down the stairs to the bottom of thelesion and then back up the stairs to the normalenamel on the other side.Dentin is arranged as a collection of tubulesrunning from the pulp towards the enamel. Thetubules are roughly 4µm in diameter near thepulp and narrow to 1µm near the enamel.Lining the inner aspect of the dentin wall is alayer of cells known as odontoblasts. These cellshave cytoplasmic extensions going into thelumens of the tubules running all the way to theenamel of the crown and the cementum of theroot. Therefore, dentin is considered a livingtissue. In some of the tubules, unmyelinatedDogs and cats have a relatively thin layer ofenamel compared to humans. A study (CrosselyDA. Tooth enamel thickness in the maturedentition of domestic dogs and cats - preliminarystudy. J Vet Dent. 12(3): 111 - 113, 1995) foundthat the enamel of most cat teeth ranges from 0.1 to 0.3 mm. In dogs, the range for most teethwas 0.1 to 0.6 mm whereas in humans, theenamel on occlusal tables is usually 1 to 2 mmthick.Enamel is relatively non-porous, impervious andsmooth and therefore relatively easy to clean andslow to stain. It acts as an effective barrier toprevent bacteria in the oral cavity from reachingthe pulp tissues. Enamel has no sensory capacityand so it protects the underlying tissues frommechanical and chemical irritation.Enamel, though hard, is brittle, tending to shearalong the planes of the prisms. A toothcomposed entirely of enamel would fractureeasily as it has no elasticity or flexibility. It iscommon to see fine dark brown lines along thedistal surfaces of the canine teeth of large dogs.These represent superficial cracks in the enamelindicating that the tooth has been bent ordistorted enough to cause cracks in the enamelbut not enough to fracture the more flexibleunderlying dentin. These lines, though unsightlyare of no clinical significance. They do,however, indicate that the patient is puttinghis/her teeth under some strain and may havehabits that put the tooth at risk of crown fracture.A discussion with the owner would be in order toidentify and remove the causes of the stress.Common causes include playing tug-of-war andother activities that see the dog grab firmly withthe canine teeth and pull back such as Shutzhundtraining.Figure #7.4. Odontoblasts with odontoblasticprocesses extending into the dentin tubules toreach the dentinoenamel junction. Note also thenerve fibers extending into the tubules. Anyfracture that involves dentin will involve damage tothe odontoblasts. Tooth survivability depends onmany factors.DentinDentin, which makes up the bulk of canine,feline and human teeth is about as hard as bonebut much softer than enamel. It is pale yellow in27
Chapter 7Anatomy and Physiology.Figure #7.5. Electronphotomicrograph of a freshlycut dentin surface showing the exposed lumensof the dentin tubules. In a healthy tooth, each ofthese pores would contain an odontoblasticprocess and so any dentin exposure constitutespulp exposure at the microscopic level. In somecases, the pulp can deal with this, in others, itcannot.Figure #7.6. Development of darker tertiary dentinwithin a tooth undergoing gradual wear. As long asthe rate of wear is slower than the rate of tertiarydentin production, the tooth may survive. If the rateof wear exceeds the rate of tertiary dentinproduction, the pulp will die, necessitating extractionor root canal treatment.dentin can be distorted and return to its normalshape.nerve fibers lie alongside the odontoblasticprocesses and so dentin is a sensitive tissue thatcan detect heat, cold, touch and variations inosmotic pressure (this is what causes teeth withexposed dentin to be sensitive to sweets). Allstimuli detected by these nerve endings areregistered as pain.A fresh chip-fracture of the crown of a tooth willexpose dentin with open tubules and may tear orexpose odontoblastic processes and nerve fibers.Therefore, the exposed dentin is sensitive to heat,cold, touch and chemical irritation. The opentubules will quickly become colonized with oralbacteria, which may propagate through thetubules to infect and kill the pulp. If there is 2 ormore millimeters of dentin between the pulp andthe fracture site, the odontoblasts under thefracture may have time to produce sufficienttertiary dentin to protect the pulp and prevent anirreversible pulpitis. If there is less than 2millimeters of dentin covering the pulp, anirreversible pulpitis with pulp necrosis is likely.If you can see a pink hue (known as a pulpalblush) through the exposed dentin of a recentlyfractured tooth, the tooth requires treatment toeither protect or remove the pulp.Dentin is produced by cells known asodontoblasts on the inside of the tooththroughout the life of the tooth. Primary dentinis that dentin which is formed prior to and duringtooth eruption. Normal secondary dentin isformed continuously thereafter, causing agradual reduction in the size of the pulp chamberand is structurally similar to primary dentin. Therate of secondary dentin production is fastest justafter eruption of the tooth and declines as theanimal ages. Therefore, the difference in pulpchamber size between one and two years of ageis very dramatic whereas the change betweennine and ten years of age may be imperceptibleradiographically.If a tooth wears gradually, due to a chewinghabit for example, as the level of wear breechesthe enamel and starts to approach the pulpchamber, tertiary dentin is produced as the pulpretreats from potential exposure. If the wear isgradual enough the teeth can be worn down tothe gum line without ever exposing the pulp (seefigure #7.6). On the other hand, if the rate ofwear exceeds the rate of tertiary dentinproduction, the pulp will die and further wearwill expose the pulp chamber. The exposedtertiary dentin of worn teeth is often brown inIrregular secondary, reparative or tertiarydentin is formed in areas exposed to injury orirritation. It has a distorted collagen pattern,fewer tubules, no nerve fibers and a darkercolour than normal dentin.The collagen component gives dentin someflexibility and allows teeth to withstandconsiderable forces without fracturing. Theoverlying enamel may crack and craze, but the28
Chapter 7Anatomy and Physiology.Figure #7.7. The developing tooth at various stages. The tooth on the left is immature (still erupting) with a wideopen apex, very thin hard-tissue wall and a massive pulp chamber. The tooth at centre might be found in a oneand a half-year-old dog. The apex has formed and the apical delta is present. The tooth wall is still relatively thinwith a large pulp chamber. The tooth at right might be found in a five-year-old dog. The pulp chamber and rootcanal are quite narrow but the pulp extends almost as far coronally as in the immature tooth.colour but is smooth and shiny (wet or dry) andhard. Debris packed in an open pulp chamber isusually dark brown to black, dull when dry andwill yield under probing with a dental explorer.myelinated fibers, which register pain via thetrigeminal nerve.If pulp is exposed through fracture, abrasion ordecay, it quickly becomes contaminated,inflamed and then necrotic. To salvage the tooth,root canal treatment is indicated. Pulps may alsobe damaged by blunt trauma with no crownfracture. As the bruised pulp dies, blood leaksfrom the vessels and seeps into the dentinaltubules, causing a discolouration of the crown.Pink, purple or gray discolouration of a crown isanother indication for root canal treatment.During mechanical abrasion, organic debrisbecomes impacted into the dentinal tubules,effectively sealing them from the outside world.Therefore, dentin exposed due to mechanicalwear will not be as sensitive as dentin exposedby an acute fracture.The Endodontic SystemThe endodontic system of the tooth consists ofthe pulp chamber (in the crown) and one or moreroot canals (within the roots). The pulp chamberhas pulp horns, which correspond to the shape ofthe overlying tooth cusp (see figure #7.2). Withtime, the pulp chamber and canals becomesmaller as secondary dentin is produced (see 7.#7). The endodontic system contains the pulp,which is composed of odontoblasts, fibroblasts,various other cells, blood vessels, lymphatics,nerve fibers and ground substance. In the maturedog or cat tooth, the pulp enters the tooththrough many tiny openings in the root apexknown collectively as the apical delta. Theremay also be accessory lateral canals further upthe root.Figure #7.8. A photomicrograph of the apicaldelta of the canine tooth of a dog. There isperiapical inflammation evident.The pulp contains unmyelinated fibers, whichcontrol vasoconstriction in the pulp, and29
Chapter 7Anatomy and Physiology.Any tooth with irreversible pulp disease (pulpnecrosis), regardless of the cause, is a candidatefor treatment. Very simply, the tooth needs to beextracted or it requires root canal therapy. Whichtreatment is chosen depends on several factorsbeyond the scope of this chapter (see Chapter 15:Endodontics). Leaving an endodonticallydiseased tooth in place may never cause anyexternally visible signs, but you can be assuredthat such teeth are sources of chronic pain andinfection and need to be dealt with. Whenextracting these teeth, it is vital that they becompletely removed. I have seen numerous casesof recurrent infra-orbital swelling in which theoffending tooth has been previously extracted.On radiographic examination, the cause ofrecurrence is invariably a retained root tip actingas a contaminated foreign body.More detail on cementum can be found in thesection on Periodontal Morphology andPhysiology.CementumCementum
Chapter 7 Anatomy and Physiology. 24 Chapter 7: Anatomy and Physiology A thorough understanding of dental and oral anatomy and physiology is essential for all members of the veterinary dental team. You must know what is normal and be able to quickly recognize the abnormal. Often, an