Transcription
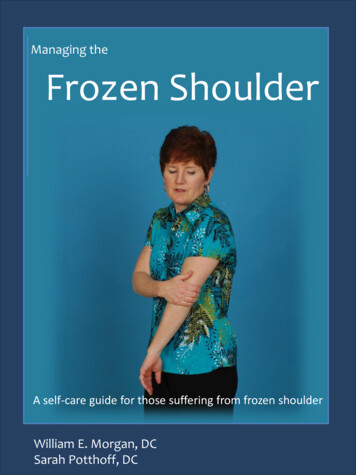
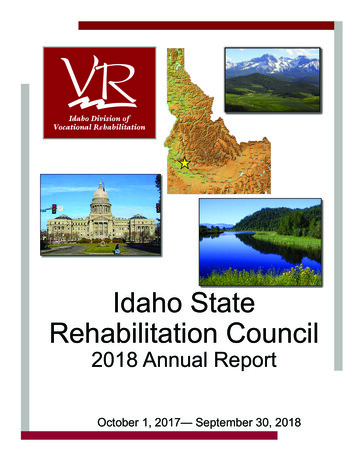
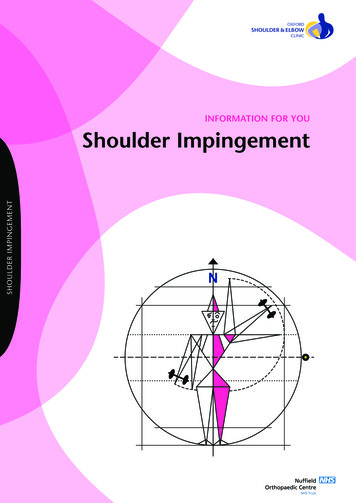
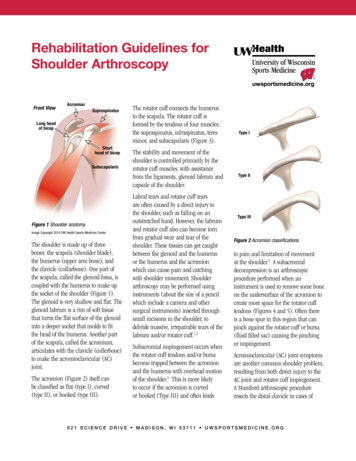
Rehabilitation Guidelines forShoulder ArthroscopyFront ViewAcromionSupraspinatusLong headof bicepShorthead of bicepSubscapularisFigure 1 Shoulder anatomyImage Copyright 2010 UW Health Sports Medicine Center.The shoulder is made up of threebones: the scapula (shoulder blade),the humerus (upper arm bone), andthe clavicle (collarbone). One part ofthe scapula, called the glenoid fossa, iscoupled with the humerus to make upthe socket of the shoulder (Figure 1).The glenoid is very shallow and flat. Theglenoid labrum is a rim of soft tissuethat turns the flat surface of the glenoidinto a deeper socket that molds to fitthe head of the humerus. Another partof the scapula, called the acromium,articulates with the clavicle (collerbone)to make the acromioclavicular (AC)joint.The acromion (Figure 2) itself canbe classified as flat (type I), curved(type II), or hooked (type III).The rotator cuff connects the humerusto the scapula. The rotator cuff isformed by the tendons of four muscles:the supraspinatus, infraspinatus, teresminor, and subscapularis (Figure 3).The stability and movement of theshoulder is controlled primarily by therotator cuff muscles, with assistancefrom the ligaments, glenoid labrum andcapsule of the shoulder.Labral tears and rotator cuff tearsare often caused by a direct injury tothe shoulder, such as falling on anoutstretched hand. However, the labrumand rotator cuff also can become tornfrom gradual wear and tear of theshoulder. These tissues can get caughtbetween the glenoid and the humerusor the humerus and the acromionwhich can cause pain and catchingwith shoulder movement. Shoulderarthroscopy may be performed usinginstruments (about the size of a pencilwhich include a camera and othersurgical instruments) inserted throughsmall incisions in the shoulder, todebride massive, irrepairable tears of thelabrum and/or rotator cuff.1,2Subacromial impingement occurs whenthe rotator cuff tendons and/or bursabecome trapped between the acromionand the humerus with overhead motionof the shoulder.3 This is more likelyto occur if the acromion is curvedor hooked (Type III) and often leadsType IType IIType IIIFigure 2 Acromion classificationsto pain and limitation of movementat the shoulder.3 A subacromialdecompression is an arthroscopicprocedure performed when aninstrument is used to remove some boneon the undersurface of the acromion tocreate more space for the rotator cufftendons (Figures 4 and 5). Often thereis a bone spur in this region that canpinch against the rotator cuff or bursa(fluid filled sac) causing the pinchingor impingement.Acromioclavicular (AC) joint symptomsare another common shoulder problem,resulting from both direct injury to theAC joint and rotator cuff impingement.A Mumford arthroscopic procedureresects the distal clavicle in cases of6 2 1 S c i e n c e D r i v e M a d i s o n , W I 5 3 7 1 1 u ws p o r t sm e d i c i n e . o r g
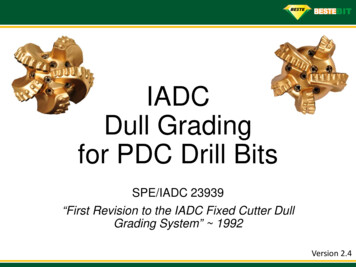
Rehabilitation Guidelines for Shoulder Arthroscopyposttraumatic degenerative disease ofthe AC joint and shoulder impingementsyndrome.4tension, thus eliminating the pain. Thisis called a biceps tenotomy and can alsobe done arthroscopically.Chronic impingement and/orinflammation of the long head of thebiceps (Figure 1) can also be a paingenerator in the shoulder. The tendoncan often become frayed or partially torn.In some cases the surgeon may “release”or cut the long head of the bicep nearits attachment site to relieve stress andRehabilitation is vital to regainingmotion, strength and function of theshoulder after arthroscopic surgery.Initially patients may use a sling forcomfort. During this time, range ofmotion exercises are started to preventthe shoulder from getting stiff and losingmobility. The rehabilitation program willBack Viewgradually progress to more strengtheningand control type exercises. General timeframes are given for reference to theaverage, but individual patients willprogress at different rates depending ontheir age, associated injuries, pre-injuryhealth status, rehabilitation complianceand injury severity. Restrictions orprecautions may also be given to rFront ViewSubscapularisFigure 4 Pre-operative radiograph of a patientwith shoulder impingement. The arrowindicates the area of the Type III acromion.Figure 5 Post-operative radiograph of the samepatient in Figure 3. Notice how the Type IIIacomion (hook) has been shaved off during thesubacromial decompression.Figure 3 Rotator cuff anatomyImage property of Primal Pictures, Ltd., primalpictures.com. Useof this image without authorization from Primal Pictures, Ltd. isprohibited.26 2 1 S c i e n c e D r i v e M a d i s o n , W I 5 3 7 1 1 u ws p o r t sm e d i c i n e . o r g
Rehabilitation Guidelines for Shoulder ArthroscopyPHASE I (usually surgery to 3 weeks after surgery)3Appointments Rehabilitation appointments begin 7 days after surgeryRehabilitation Goals Reduce pain and swelling in the post-surgical shoulder Regain full passive range of motion (PROM) and active assistive range ofmotion (AAROM) Activation of the stabilizing muscles of the gleno-humeral and scapulo-thoracicjointsPrecautions Avoid activities that may impinge on the denuded bone of the acromion Use sling as needed for comfort Relative rest to reduce inflammationSuggested TherapeuticExercise Begin 7 days after surgery, sub-maximal shoulder isometrics forinternal rotation/external rotation, flexion/extention and abduction/adduction Shoulder AAROM/PROM: Codman’s, pulleys, cane exercises in all planes of motionexcept horizontal adduction (these should stay relatively pain free) Gentle shoulder mobilizations as needed Hand gripping Elbow, forearm, and wrist active range of motion (AROM) Cervical spine and scapular AROM Postural exercisesCardiovascular Fitness Walking, stationary bike Avoid running and jumping due to the forces that can occur at landingProgression Criteria The patient can progress to Phase II when they have achieved full PROM andnormal (5/5) strength for internal rotation/external rotation with arm at side6 2 1 S c i e n c e D r i v e M a d i s o n , W I 5 3 7 1 1 u ws p o r t sm e d i c i n e . o r g
Rehabilitation Guidelines for Shoulder ArthroscopyPHASE II (begin after meeting Phase I criteria, usually 4-5 weeks after surgery)4Appointments Rehabilitation appointments are once every 1-2 weeksRehabilitation Goals Controlled restoration of AROM Strengthen shoulder and scapular stabilizers in protected position(0 - 45 abduction) Begin proprioceptive and dynamic neuromuscular control retraining Correct postural dysfunctionsPrecautions Avoid repetitive overhead activities Post-rehababilitation soreness should alleviate within 12 hours of the activitiesSuggested TherapeuticExercise AROM in all cardinal planes--assessing scapular rhythm Gentle shoulder mobilizations as needed Rotator cuff strengthening in non-provocative positions(0 - 45 abduction) Scapular strengthening and dynamic neuromuscular control Cervical spine and scapular AROM Postural exercises Core strengtheningCardiovascular Fitness Walking, stationary bike, Stairmaster Avoid running and jumping until athlete has full rotator cuff strength in a neutralposition due to forces that can occur at landingProgression Criteria The patient can progress to Phase III when they have achieved full AROM(equal to uninvolved side) and normal (5/5) strength for internal rotation/externalrotation with shoulder at 45 abduction6 2 1 S c i e n c e D r i v e M a d i s o n , W I 5 3 7 1 1 u ws p o r t sm e d i c i n e . o r g
Rehabilitation Guidelines for Shoulder ArthroscopyPHASE III (begin after meeting Phase II criteria, usually 7-8 weeks after surgery)5Appointments Rehabilitation appointments are once every 2-3 weeksRehabilitation Goals Precautions Post-rehabilitation soreness should alleviate within 12 hours of the activitiesSuggested TherapeuticExercise Multi-plane AROM with gradual increase in velocity of movement - assessingscapular rhythm Gentle shoulder mobilizations as needed Rotator cuff strengthening at 90 abduction, provocative positions and work/sportspecific positions Scapular strengthening and dynamic neuromuscular control in overhead positionsand work/sport specific positions Cervical spine and scapular AROM Postural exercises Core strengthening Begin education in sport specific biomechanics with very initial program forthrowing, swimming or overhead racquet sportsCardiovascular Fitness Walking, stationary bike, Stairmaster, running Avoid swimming until athlete has normal (5/5) rotator cuff strength at 90 abduction and negative impingement signsProgression Criteria The patient can progress to phase IV when they have achieved full multi-planeAROM (equal to uninvolved side) and normal (5/5) strength for internal rotation/external rotation with the shoulder at 90 abduction and full supraspinatus strengthNormal (5/5) rotator cuff strength at 90 abduction and with supraspinatus testingFull multi-planar AROMAdvance proprioceptive and dynamic neuromuscular control retrainingCorrect postural dysfunctions with work and sport specific tasks6 2 1 S c i e n c e D r i v e M a d i s o n , W I 5 3 7 1 1 u ws p o r t sm e d i c i n e . o r g
Rehabilitation Guidelines for Shoulder ArthroscopyPHASE IV (begin after meeting phase III criteria, usually 10-12 weeks after surgery)Appointments Rehabilitation appointments are once every 2-3 weeksRehabilitation Goals Precautions Post-rehabilitation soreness should alleviate within 12 hours of the activitiesSuggested TherapeuticExercise Multi-plane AROM with gradual increase in velocity of movement - assessingscapular rhythm Shoulder mobilizations as needed Rotator cuff strengthening in at 90 abduction, provocative positions and work/sport specific positions - including eccentric strengthening, endurance and velocityspecific exercises Scapular strengthening and dynamic neuromuscular control in overhead positionsand work/sport specific positions Work and sport specific strengthening Core and lower body strengthening Throwing program, swimming program or overhead racquet program as neededCardiovascular Fitness Design to use work or sport specific energy systemsProgression Criteria The patient may return to sport after receiving clearance from the orthopedicsurgeon and rehabilitation therapist. This will be based on meeting the goals ofPhase IIINormal rotator cuff strength at 90 abduction and with supraspinatus testingAdvance proprioceptive and dynamic neuromuscular control retrainingCorrect postural dysfunctions with work and sport specific tasksDevelop strength and control for movements required for work or sportThese rehabilitation guidelines were developed collaboratively by Marc Sherry, PT, DPT, LAT, CSCS (msherry@uwhealth.org) andthe UW Health Sports Medicine physician group.Updated 3/2011References1. Liem, D, et al. Arthroscopic Debridementof Massive Irreparable Rotator Cuff Tears.Arthroscopy. 2008 July; (24)7:743-748.2. Martin DR, Garth WP Jr. Results ofArthroscopic Debridement of GlenoidLabral Tears. Am Jour Sports Med. 1995;23 (4):447 -451.3. Attiq-ur-Rehman, Wajid MA, AhmadT. Shoulder impingment syndrome:outcome of arthroscopic subacromialdecompression. J Coll Physicians SurgPak. 2009 Oct;19(10):636-639.4. Lesko, PD. Arthroscopic MumfordProcedure Variation of Technique. IowaOrthop J. 1999; 19: 93–98.Copyright 2011 UW Health Sports Medicine Center66 2 1 S c i e n c e D r i v e M a d i s o n , W I 5 3 7 1 1 u ws p o r t sm e d i c i n e . o r gSM-27278-11At UW Health, patients may have advanced diagnostic and /or treatment options, or may receive educational materials that vary from this information. Please be aware that this information is not intended to replacethe care or advice given by your physician or health care provider. It is neither intended nor implied to be a substitute for professional advice. Call your health provider immediately if you think you may have a medicalemergency. Always seek the advice of your physician or other qualified health provider prior to starting any new treatment or with any question you may have regarding a medical condition.
5 621 Science Drive MaDiSon, Wi 53711 uWSportSMeDicine.org rehabilitation guidelines for Shoulder arthroscopy PHASE III (begin after meeting Phase II criteria, usually 7-8 weeks after surgery) Appointments Rehabilitation appointments are once every 2-3 weeks Rehabilitation Goals Normal (5/5) rotator cuff strength at 90 abduction and with supraspinatus testing