Transcription
Evolving Treatment of Paravisceral &Thoracoabdominal Aortic DiseaseRichard P. Cambria, M.D.Systems Chief Vascular Services, and Chief of Vascular and Endovascular Surgery,Steward Health Care System and St. Elizabeth’s Medical Center, Boston MA.Robert R. Linton MD Professor of Vascular & Endovascular Surgery,Harvard Medical School (Emeritus)1OUTLINE The Boston origins and evolution of surgery of theDTA/TAAA (Paravisceral vs Type IV TAA vs Type IIII TAA) Evolution of operative strategies and adjunctsSCI The impact and evolution of TEVAR andEVARRelevant? Role of Open Surgery 2019 and beyond21
Historical PerspectiveLINTON – INTRASACCULAR WIRING - 195250 YEAR FOLLOW-UP !342
BOSTON ORIGINS OF DTA SURGERY Robert Gross, M.D. @ The Children’s Hospital 1945 firstdirect repair coarc. At MGH Dr. Linton’s coarc. repairs and the short livedhomograft era5LINTON BEGINS THORACOABDOMINALAORTIC SURGERY - 195663
Prior to 1985 TAA repair @ MGH 50% mortality! Initial experience after 1986 in 30patients 8% mortality Impact of elective operation, op time,blood loss, x-clamp timesArch Surg 1989; 124:6207Pararenal AneurysmsDEFINITIONS Juxtarenal/pararenal infrarenal neck 1cm implies clamp placement needs to besuprarenal/supraceliac (EVAR IFU Relevant)84
9DEFINITIONS Suprarenal aneurysm one or both renalsoriginate from AAA separatereconstruction105
11Complex AneurysmsDEFINITIONS Type IV TAA graft carried proximal to celiac126
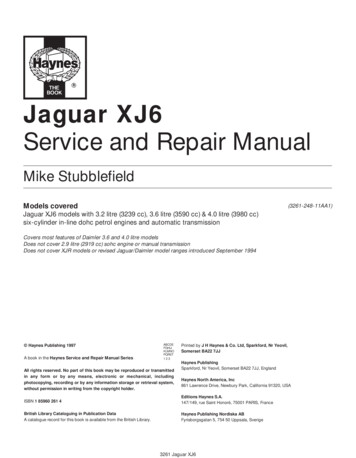
THORACOABDOMINAL ANEURYSMSType I(27%)Type II(15%)Type III(36%)Type IV(22%)42% WITH STRICT CRAWFORD DESIGNATION13DESCENDING THORACIC AND TAAA SIZECRITERIA FOR SURGERYCirculation 2015;132:1620-29147
Distinguishing TAA CharacteristicsPrior Aortic Resection (32.7%)AAADescending or TAAAAscending/ArchClinical PresentationElectiveUrgent non-rupturedRupturedX20 % of casen 149 (%)88 (59)30 (20)31 (21)347 (76.3)51 (11.2)52 (11.4)chronic dissection15Suprarenal AAA168
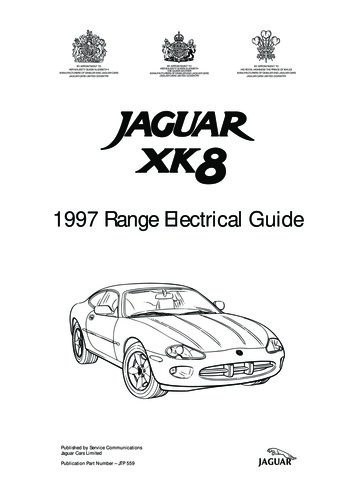
AAA SURGERYSELECTIVE USE OF SURGICALAPPROACHES FOR AAATransperitoneal Right renal graftRoutine Right iliac or complexInfrarenalpelvic repairAortic Prior left colectomy AAA neck turns to right SurgeryRetroperitoneal Multiple priorlaparotomies Obesity Selected ABD stoma Graft above renals Horseshoe kidney,inflammatory AAAEVAR17Retroperitoneal ApproachFor Aneurysms LT Kidney Up189
Total Exposure of Visceral SegmentCeliacSMARenal VeinR RenalLeftKidneyIMA19Retroperitoneal Approach2010
Thoracoabdominal IncisionTranspleural / Transabdominal212211
TA APPROACH FOR PARA/SUPRARENALAAA AND TYPE IV TAAPartial lateral division ofdiaphragm232412
Suprarenal Type IV TAA Repair25Current ResultsOpen Juxta/Para Renal Aneurysm RepairAuthorChong et.al.Landry et.alKnott et.alChiesa et.alNathan et.alTsai 821268597199Op Mortality1.8%6.1%0.8%3.5%3.4%2.5%760mean 3 %Rutherford 9th ed. 20192613
JVASC Surg 2012; 56: 2-727Stent Graft Repair Juxtarenal AAA SLOWRegulatoryEvolution Oct 2001 first ZFEN (RG) 20181,600implanted inUSA2814
JVASC Surg 2014; 60: 142029Current ResultsEVAR for Complex AAA (only) 16 Publications (2004-12) detailing 1,187patients with mean F/U 19 months Technical Success nearly uniform Branch patency 95 % range 30 day Mortality (range 0-3.5 %) mean 1.8 % GLOBALSTAR Registry (n 318) 3.5 %Source: Endovascular Aortic Repair ed. Oderich: Springer 20173015
J VASC Surg 2015; 61: 242-5531 NEARLY 10K PATIENTS! POOLED OP MORTALITY 11% COMMENTARY: MORE THAN HALFSERIES 15 YEARS OLD!JJ Vasc Surg 2018: 68:634-4513216
CURRENT RESULTSWITH OPEN AND ENDOVASCULAR REPAIRType IType IIType III Type IVOutcomes and operative strategiesvary with TAA extent for Open and Endovascular Repair33Type IV TAAAConduct and mode of Operation Risk of SCI in Type IV ? Higher withTEVAR Adjuncts not utilized in Type IV repair:Atrial-femoral bypassCSF drainMotor evoked potential monitoringPermissive hypothermia Type IV ? Open ? Endo ? hybrid3417
Current Results Open Type IV TAA RepairAuthorYearCoselli et.al2002, 073293.6 %Chiesa et.al2006342.9 %Kieffer et.al200817113.4 %Richards et.al2010536.0 %Nathan et.al2011835.6 %Patel et.al20111792.8 %8495.7 %TOTALS#PatientsOp MortalitySource: Rutherford 9th ed. 201935TYPE IV RESULTSJ Vasc Surg 2011;53:1492-83618
STANDARDIZED CLAMP/SEWOPERATIONPreserve diaphramCold renal perfusionBeveled prox.suture lineRoutine lt. renal sidearm37Clinical features in 178 Type IV pts Age:73 8 HTN: Smoker: CRI ( 1.8mg/dl):153 (86%)147 (83%)32 (18%) Symptomatic:32 (18%)3819
Clinical OutcomesN 178 Mortality:5 (2.8%)SCI:4 (2.2%)HD / renal failure:5 (2.8%) Any complication: 45 (25%)39Predictors of Mortality/ComplicationsComposite outcome: death any complicationVariableOR95% CIp valueCRInsuff3.4[1.4 – 8]0.0164020
Multi-center French ExperienceOp mortality 14.3%SCI 4.8%Ann of Surgery 2014;00:1-1041OPEN TAA REPAIR BACKGROUND Mortality 10% Total Spinal Cord Ischemia 16%half (8%) devastating paraplegiaJ Vasc Surg 1993; 17:357-704221
IMPACT OF SPINAL CORD ISCHEMIAAdjuncts to prevent paraplegia operative conduct43SUMMARY OF OPERATIVE TECHNIQUE1986- 2005 Emphasis on expediency and simplicity-clamp/sew without external bypass/perfusion In-line mesenteric shunt to decrease visceralischemia Cold renal perfusion Epidural cooling for spinal cord protection Aggressive reimplantation of T9-L1intercostals4422
routine sacrifice of segmental aorticbranches can be carried out in a way thatwill allow surgical and endovasculartherapy of extensive distal aortic aneurysmswithout neurologic injury.Ann Thorac Surg 2007;83;S865-945MRA DEMONSTRATESCORD COLLATERALS 85 TAA pts studied with MRA and intraoperativeMEVOK potentials p .0015 correlation between collateral demonstrationof preservation MEVOK with x-clamp Most collaterals originated caudal to the distal clamp pelvic arteriesJ Vasc Surg 2008;48:261-714623
Impact of Collateral Network Concept Refined techniques for spinal cord protection Operative mortality for Extent I-III TAA under 5%J Vasc Surg 2011;53:1195-20147Shift in Spinal Cord Protection Support of the cordcollateral network withdistal aortic perfusion Monitoring of MEVOPduring sequentialclamping4824
Literature ReviewOpen TAAA Repair (? Includes acute)AuthorYear#ptsCoselli et.alSchepens et.alEtz et.alAchweck et.alJacobs et.alSafi et.alLancaster 1,10648530-day mortality6.6 %12.4 %9.7 %12 %8.6 %14.6 %8%TOTALS5, 64410 %Source: Endovascular Aortic Repair ed. Oderich. Springer 201749Current Results30% last 100 cases were TAAA ofchronic dissection etiologyJ Vasc Surgery 2013; 58:283-2905025
Results - OutcomesVariableClamp/Sew(n 385)DAP/MEVOP(n 100)p1.0%0.501Intra-opDeathEarlyPost-opDeathEarly Post-op Death9.9%4.0%4.0%0.072Hospital LOS (d)21.6 23.519.9 12.60.492Permanent SCISCIPermanent11.9%11.9%3.0%3.0%Perm SCI/Death19.1%7.0%0.003ARF with HD11.4%5.1%0.0630.5%9.9%0.0720.0080.00851 MEDICARE DATABASE (2004-07) SIGNIFICANT IMPROVEMENT INEARLY MORTALITY (P .02),COMPLICATIONS (P .01) AND 1YEAR SURVIVAL (P .01)J Vasc Surg 2018; 68; 941-75226
Multi-center French Experience“F/B-EVARcarriessignificant rate ofOpmortality a 21%14.3%Opmortalitymortality and complications the complexitySCISCI 16.6%4.8%of the procedure”Ann of Surgery 2014;00:1-1053 112 TYPE IV and 73 TYPES I-III MORTALITY FOR I-III8.2% REINTERVENTION AT 5 YEARS50%J Thorac Cardiovasc Surg. 2017 Feb;153(2):S32-S41.5427
Durability of Open Surgical Repair of TypeI-III Thoracoabdominal aortic aneurysmJVASC Surg April 2019; 1-1155Summary ResultsEndovascular TAAA Repair 15 clinical series (of pioneers e.g. Chutter,Greenberg, etc) detailing 1,517 patients Many include JRA, SRA, and few non-electivecases Technical success uniform 30-day mortality (edited) range (2-9 %) andSCI (2-16.7 %)Source: Endovascular Aortic Repair5628
JVASC Surg 2018; 68: 1936-194557Role of Hybrid Operation (?)5829
Hybrid Operation:Question Less Invasive Alternative Combination ofdebranching bypassescreates distal seal zonefor TEVAR Aortic Arch Visceral Segment59Preliminary Results of the NorthAmerican Complex Abdominal AorticDebranching (NACAAD) RegistryGustavo S. Oderich, Peter Gloviczki, Mark Farber,William Quinones-Baldrich, Roy Greenberg,Gilbert R. Upchurch Jr., Dan Clair, Sean Lyden, Guillermo A.Escobar, Carlos Timaran, James Black, Sharif Ellozy, EdwardWoo, Michael Singh, Mark Fillinger, Jason Lee, Juan CJimenez, Jonathan L. Eliason, Himanchu J. Patel, PurandathLall. Stephen Cha and Patrick ClagettFor the NACAAD investigators6030
NACAAD registryMortality30 early deaths (14%)––––––Multisystem organ failure, 11Cardiac event, 10Ruptured aneurysm, 4Ischemic stroke, 2Intracranial hemorrhage, 2Intraoperative hemorrhage, 1Mortality in centers with 10cases: 11% (0 – 21%)TAAA, thoracoabdominal aortic aneurysmPRAA, pararenal aortic aneurysmEarly death, 30-day and/or in-hospital61CIRC. 2011; 124: 26706231
Ann Cardiothoracic Surg.2012 Sep; 1(3): 311-31963JVASC Surg 2011 Jul; 54(1): 30-406432
J. Vis Surg 2018; 465Summary The Evolution of total Endovascular repair ofTAA HAS BEEN SLOW!USA Regulatory EnvironmentINTERNATIONAL MARKET Surgeon Experience and Expertise recalls theEvolution of Open Repair Current ResultsPararenalType IV TAAAType I-III TAA6633
At MGH Dr. Linton’s coarc. repairs and the short lived homograft era LINTON BEGINS THORACOABDOMINAL AORTIC SURGERY - 1956 5 6. 4 . Knott et.al 2008 126 0.8% Chiesa et.al 2006 85 3.