Transcription
Using Predictive Models to Move MedicaidProviders Toward Best Practices and Reduce WastePredictive Modeling SummitGary Redding, Vice President and Practice Leader, Thomson ReutersMichelle McAllister, Consulting Manager, Thomson Reuters
AGENDA Thomson Reuters Using Predictive Models to Move MedicaidProviders Toward Best Practices and ReduceWaste 2009 Thomson Reuters Questions and Discussion2HEALTHCARE PAYER SOLUTIONS
Thomson ReutersGary Redding, Vice President and Practice Leader, Thomson Reuters
2009 Thomson ReutersOUR FOOTPRINT4HEALTHCARE PAYER SOLUTIONS
Knowledge To ActThomson Reuters is the world’s leading source ofintelligent information for business and professionals.FINANCIALLEGALHEALTHCARE & SCIENCE Integrated decision support solutions for improvingclinical and business performanceTAX &ACCOUNTINGMEDIA Insights for better healthcare touching 150 millionlives 2009 Thomson Reuters We are known for our: Independence Objectivity Reliability5HEALTHCARE PAYER SOLUTIONS
UNPARALLELED EXPERTISE ACROSSTHE SPECTRUM OF HEALTHCAREGE, FedEx,GM, Ford,200 Boeing,EmployersCorning, DowMany U.S.hospitals100 HealthPlans3,000 HospitalsFederalGovernmentCMS, AHRQ,CDC, SAMHSA,VA, DOD11 state employers28 Medicaidagencies8 HHS agenciesAll major U.S.pharmacompanies 2009 Thomson ReutersCIGNA,Paramount,Emblem,Humana,NumerousBCBS plansStateGovernmentPharma6HEALTHCARE PAYER SOLUTIONS
A Trusted Partner to Government and edpac 2009 Thomson ReutersResearch& Non-ProfitStateGovernment28 Medicaid agencies11 state employersAARPAcademyHealthBridges to ExcellenceCalifornia Cooperative Healthcare Reporting initiativeIHA (Integrated Healthcare Association)Pacific Business Group on HealthMidwest Health Initiative (St. Louis)Robert Wood Johnson FoundationOthers77HEALTHCARE PAYER SOLUTIONS
Medicaid RMSALGALATX 2009 Thomson ReutersFL8HEALTHCARE PAYER SOLUTIONS
OUR VALUEPROVIDING INTELLIGENT INFORMATIONTO MAKE BETTER DECISIONS FASTERDECISION SUPPORT 2009 Thomson ReutersClinical and ManagementReporting, Modeling,AnalysisMANAGING DATACONSULTING ANALYTICS400 Sources,SAS 70 CertifiedSubject Matter Experts,Account TeamMEASURING PERFORMANCEBENCHMARKING & NORMSQuality Measurement, P4P,Physician Measurement3,000 Measures, 69 Million Lives,PULSE SurveyREFERENTIAL DATAENGAGING CONSUMERSConsumer Advantage, InformedEnrollmentClinical, Drug, Disease, Poison,Toxicology9HEALTHCARE PAYER SOLUTIONS
We Help Our Customers . . . Analyze state and national trends Profile provider performance Monitor population health Fight Fraud, Abuse, Waste and Overpayment Improve clinical performance and outcomes Forecast, monitor and manage healthcare costs Oversee vendor contracts Support care management Formulate payment policy Launch cost control strategies 2009 Thomson Reuters Support prevention programs Answer any healthcare programquestionHEALTHCARE PAYER SOLUTIONS
Using Predictive Models to Move MedicaidProviders Toward Best Practices and Reduce WasteMichelle McAllister, Consulting Manager, Thomson Reuters
Overview Context– What is Predictive Modeling?– History of Predictive Modeling How it Works– Predictive Modeling Basics– A Useful Approach to Predictive Modeling and Targeting 2009 Thomson Reuters Case Studies: Applications in Moving ProvidersToward Best Practices and Reduce Waste12HEALTHCARE PAYER SOLUTIONS
Context
What is Predictive Modeling? Use of demographic, diagnostic, and utilizationinformation, with analytic models to predict:– Beneficiaries who will be high-risk/high-cost in the future– Future costs– Future utilization– Influence Best Practices– Help Reduce Waste 2009 Thomson Reuters in order to better intervene, manage risk, ensurequality and set rates14HEALTHCARE PAYER SOLUTIONS
History of Predictive Modeling Research beganon health-basedrisk models Health Insurance Planof California (HIPC)implemented ahomegrown riskadjustment model 2009 Thomson Reuters State of WashingtonEmployees and Stateof Colorado’s Medicaidprogram used riskadjustment forpayments15 1st Society of Balanced Budget Act –Actuaries studymandated risk-adjustedpayments forcomparing severaldifferent risk modelsMedicare Choice foryear 2000 (Principaland risk adjusters.Inpatient Dx Model)HEALTHCARE PAYER SOLUTIONS
History of Predictive Modeling (cont.) 2009 Thomson Reuters 2nd Society ofActuaries studycomparing severaldifferent riskmodels and riskadjusters. DCGschosen best inclass. CMS selects an ‘allencounter model’16 3rd Society ofActuaries studycomparing severaldifferent risk modelsand risk adjusters.DCGs chosen best inclass. 12 modelstested.HEALTHCARE PAYER SOLUTIONS
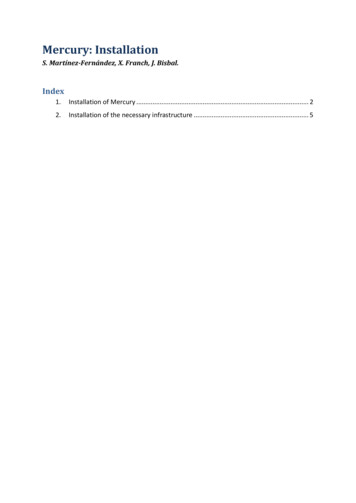
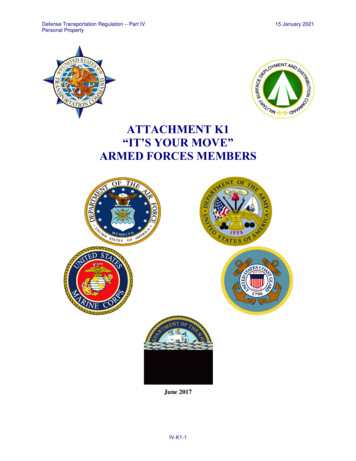
History of Predictive Modeling (cont.)Individual Level R-squared60.00%DCG All-EncounterACGsCDPS50.00%CRGsIngenix ERG* R squaredExplains predictive value.A higher R squaredequates to a better degreeof predictability.DCG RxGroups40.00%Ingenix PRG30.00%20.00% 2009 Thomson Reuters10.00%0.00%ConcurrentProspectiveSociety of Actuaries, “A Comparative Analysis of Claims-based Methods of Health Risk Assessment for Commercial Populations,” 2007HEALTHCARE PAYER SOLUTIONS
How it works
Predictive Modeling Basics Most models are designed to require 1 year’s worthof enrollment and medical and/or pharmacy data. Purpose Varies– Predictive Modeling in Pricing Identify difference in cost between people and groups to priceaccordingly– Predictive Modeling in Care Management 2009 Thomson Reuters Resource use and intensity is the focus19HEALTHCARE PAYER SOLUTIONS
DCGs Thomson Reuters currentlyutilizes Diagnostic Cost Groups(DCGs)– DCGs are a population-basedclassification and riskadjustment methodologyDCG Models in Advantage SuitePopulationGroupMedicareAll - encounterMedicaidAll - encounter– Developed and licensed byVerisk Health Inc.– Selected by CMS for theMedicare Choice ProgramVariantAll – encounterCommercialRx Groups –Rx/InpatientRx Groups – RxOnly 2009 Thomson ReutersEtc.HEALTHCARE PAYER SOLUTIONS
The DCG models work by: Classifying raw administrative (medical and/orpharmacy claims as well as eligibility and aidcategory) data into coherent clinical groupings Applying clinically valid hierarchies and interactionsto create an aggregated, empirically valid patientscore at the individual beneficiary level 2009 Thomson Reuters Correlating the scores with the cost of the healthburden carried by the beneficiary Aggregating individual scores by groups of interestcreates group-level predictive results specific tomany Medicare/Medicaid applications21HEALTHCARE PAYER SOLUTIONS
Medical Episode Grouper (MEG)What is an episode? An episode is all care for a course of treatment of a disease– Primary and secondary diagnosis codes grouped into one of 560disease categories– Stratified by severity of illness– Disease categories and clinical criteria specified by physicians atJefferson Medical College Includes inpatient, outpatient and drug claims– Not every claim is assigned an episode Also includes admissions 2009 Thomson Reuters Patients may have more than one episode at any given time22HEALTHCARE PAYER SOLUTIONS
2009 Thomson ReutersMEG providesclinically relevantgrouping23HEALTHCARE PAYER SOLUTIONS
MEG: Grouping MethodologyAppropriatelygroup claimsinto episodesaccording todiseasecategory andrelative timebetweenservices Classification - Diagnosis codes from healthcare claims and otheradministrative data are grouped into one of the over 550 DiseaseStaging disease categories and severity stages. Beginning and Ending Episodes - Clean periods unique to eachdisease category are used to group each claim into an episode. Inclusion Logic - Less specific episode groups occurring in closeproximity to specific episodes are combined with the specificepisodes, e.g. “other gastrointestinal or abdominal symptoms" and"appendicitis". Drug Data - Mappings of National Drug Codes (NDCs) to episodegroups enables pharmacy claims to be grouped to relevant episodes. Lookback Procedure - Lab and diagnostic imaging claims precedingan episode are examined to determine whether they should becombined with the episode. 2009 Thomson 4RxOfficeVisitThe completeepisode ranges intime between the labtest and the finaloffice visit.HEALTHCARE PAYER SOLUTIONS
MEG—Putting it All TogetherEpisode an e 2009 Thomson ReutersVisitDRUG TRANSACTION RMLOOKUP 1-1595-11-1525HEALTHCARE PAYER SOLUTIONS
Medical Episode Grouper (MEG)What is the analytic value of using episodes? Attributes all costs to diseases– Particularly prescription drugs Finds a physician that is accountable for treatment– Managing Physician Identifies the physician who guided treatment usually providingmultiple E & M visits Use to identify the decision-maker in a patient’s care– Primary Physician Identifies the physician with the highest costs Use to evaluate if specific episode costs 2009 Thomson Reuters Measures and compares the costs of treating disease– Which providers and plans are most efficient– Both price and resource consumption26HEALTHCARE PAYER SOLUTIONS
MEG: Potential Drug Substitutions – ACEI vs. ARBQuintile 1Quintile 512%41%59%88% 2009 Thomson ReutersACEIARBACEIARB ARB has no generic substitute and is more costly than therapeutically similar ACEI. Quintile 5 patients are more likely to receive an ARB.27HEALTHCARE PAYER SOLUTIONS
MEG:Variation and Cost of Antithrombotic Treatment People prescribe/take antithrombotics for hypertension to lower risk ofischemic event – “it makes sense.” Aspirin/antiplatelet is recommended for secondary prevention of ischemicevent. However:– Warfarin not recommended.– Antiplatelet therapy not recommended for primary prevention, as risk ofhemorrhage is greater than risk reduction of ischemic event. 2009 Thomson ReutersCost of Antithrombotic Drugs for Primary PreventionQuintile 1 3,686Quintile 5 213,962Lip GYH, Felmeden DC. Antiplatelet agents and anticoagulants for hypertension. CochraneDatabase of Systematic Reviews 2004, Issue 3. Art. No.: CD003186. DOI:10.1002/14651858.CD003186.pub228HEALTHCARE PAYER SOLUTIONS
Episodes and Patient-Level Adjustment Diagnostic Cost Groups (DCGs)– Risk adjustment methodology used to predictcurrent or future patient costs, e.g. relative riskscore (RRS)– Unit of analysis – the patient– Based on all prior or current year claims to identifypatient-level complexity/comorbidities 2009 Thomson Reuters Together, MEG and DCGs provide a completepicture of a patient29HEALTHCARE PAYER SOLUTIONS
Disease Staging Framework Initially developed under contract to NCHSR withongoing private development by Medstat/Jeffersonteams Software converts a stream of claims into clinicallyhomogeneous groups Takes over 15,000 ICD-9-CM codes to 560 diseasecategories Independent of setting or treatment 2009 Thomson Reuters Etiology assigned to each category Severity stratification based on robust clinicalcriteria30HEALTHCARE PAYER SOLUTIONS
A Useful Approach to Predictive Modeling andTargeting: Risk Adjusted EpisodesWhat is Risk Adjusted Episodes? An improved method of benchmark adjustment in Decision Analystthat combines the disease and severity strength of MEG with thepopulation-based risk adjustment power of the DCG grouper Basing risk adjustment on average episode costs ignores significant riskfactors which physicians take into account when treating a patient.– Age and gender– Comorbidities Basing risk adjustment on a single illness burden score (for the patient)ignores vital information about diseases and severity levels. 2009 Thomson Reuters– Risk adjustment using illness burden accounts for the risk of a population across allconditions, but is not enough to determine expected costs for a specific condition. Combining episodes and illness-burden methodologies addresses theshortcomings of each.31HEALTHCARE PAYER SOLUTIONS
The Problem62 year old, MaleComorbidities Renal failure Deep vein thrombosis Impaired fasting glucose AsthmaMichaelProgressive Angina2005 Costs 15,323Relative Risk Score 56.3858 year old, FemaleDianeComorbidities Hypertension, minimalProgressive Angina2005 Costs 5,974 2009 Thomson ReutersRelative Risk Score 5.54Patients at the same severity levelwithin an episode can havesignificant cost variance .due to different comorbidity profiles.32HEALTHCARE PAYER SOLUTIONS
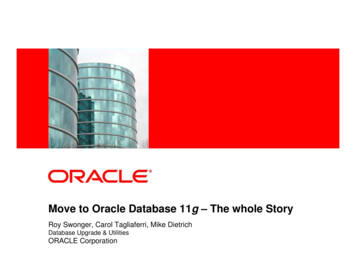
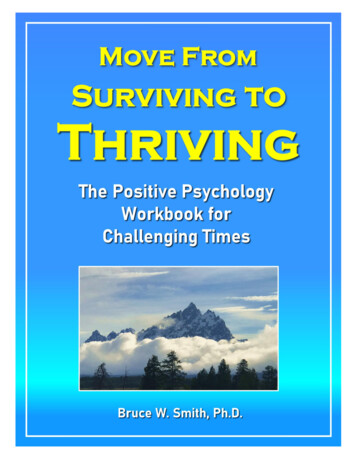
Dimensions of Risk that Drive Episode Cost 20,000Mean AllowedPayments 15,000 10,000 5,000 01234Complexity Levels5 2009 Thomson ReutersEpisode Severity LevelsTo fairly compare physicians on cost ofcare, differences in complexity levels needto be considered1 - Stable Angina2 - Progressive Angina3 - AMISource: Based on 100 Million Claims, 2003-200433HEALTHCARE PAYER SOLUTIONS
Risk Adjusted Episodes– The method is intuitive and easy to explain to physicians /clinicians– It does a better job at an individual physician-level ofaccounting for that physician’s mix of patients / severity 2009 Thomson Reuters– It has potential for improvements in predictive power34HEALTHCARE PAYER SOLUTIONS
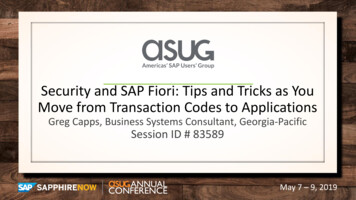
Risk Adjusted Cost Profile for CardiologyEpisodes 2009 Thomson ReutersActualEpisodeCosts PerPhysicians # Episodes Cost Scale(avg 100) EpisodeExpected CostsPer 77159 6,426 5,075 5,1961.271.24Harris75115 2,106 3,018 2,8750.700.73Davis72159 4,983 5,690 5,9170.880.84Brown6280 838 1,537 1,4590.550.57Wilson6283 1,001 1,501 1,4920.670.67Smith61167 5,667 5,746 5,8510.990.97Gold5886 816 1,557 1,5920.520.51Murphy57158 3,710 5,646 5,3290.660.70Evans53110 2,653 2,990 2,8580.890.93Ford5391 2,671 1,818 1,9941.471.34Source: Based on subset of Marketscan Commercial data, 2002-200435HEALTHCARE PAYER SOLUTIONS
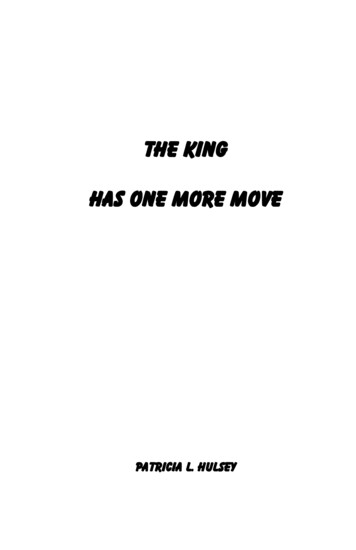
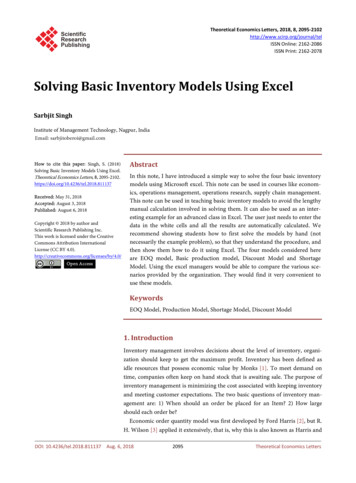
Risk Adjusted Cost Profile for Dr. FordArrhythmias1.011ActualCosts PerEpisode 226CongestiveHeart Failure3.011Angina Pectoris1.01Angina Pectoris 2009 Thomson ReutersEpisode GroupStage EpisodesExpected CostsPer EpisodeBeforeAfterPerformanceRatioBeforeAfter 1,217 1,2950.190.17 391 6,474 8,5250.060.052 18,816 4,632 4,6644.064.031.021 36,638 7,583 7,8974.834.64Angina Pectoris2.041 23,794 22,033 28,4801.080.84EssentialHypertension,Chronic Maint1.0145 870 1,057 1,0570.820.82OtherCardiovascularSymptoms1.012 1,876 1,128 1,2901.661.4653 2,671 1,818 1,9941.471.34TOTALSSource: Based on subset of Marketscan Commercial data, 2002-200436HEALTHCARE PAYER SOLUTIONS
Risk Adjusted Cost Profile for Dr. Ford(patient detail)Episode GroupStagePatientActualExpected CostsCosts PerPer EpisodeEpisode BeforeAfterDCG RelativeRisk ScoreActualAverageCongestive HeartFailure3.01Jim 391 6,474 8,52516.087.04Angina Pectoris2.04Adam 23,794 22,033 28,4804.464.36OtherCardiovascularSymptoms1.01Sarah 3,535 1,128 1,1762.601.55OtherCardiovascularSymptoms1.01Dave 218 1,128 1,4038.221.55Using the 69 providers with at least 10 episodes as a sample, no provider’s performanceratio changed by more than 0.15. 2009 Thomson ReutersUsing all 149 providers as a sample, 71% of performance ratios changed by 0.05 or less.In general, only modest changes are expected when using Risk Adjusted Episodesfor dynamic benchmarks (slightly more variance for Marketscan benchmarks).Source: Based on subset of Marketscan Commercial data, 2002-200437HEALTHCARE PAYER SOLUTIONS
Case StudiesMoving Medicaid Providers Toward Best Practices and Reduce Waste
Provider Profiling with Risk Adjusted Episodes Blue Cross Blue Shield Plan was charged with developingrisk-adjusted provider profiles for both internal and externalprofiling goals. Thomson Reuters combined patient-level risk scores from theDiagnostic Cost Grouper (DCG) with the severity score fromThomson Reuter’s Medical Episode Grouper. 2009 Thomson Reuters Eliminates the potential of rewarding physicians who care forpatients with few co-morbid diseases while penalizingphysicians who care for patients with a significant illnessburden. Results: BCBS used information during contract negotiations,and supplied providers with actionable goals andrecommendations.39HEALTHCARE PAYER SOLUTIONS
Provider Performance and Gaps in Care Thomson Healthcare and APS Health Systems arepartnering to assist a State Medicaid agency inusing data to create meaningful internal andexternal analyses to evaluate provider performanceand create an action plan to address any gaps. Maintain healthcare utilization review systemspecific to disease/risk status – based on updatedguidelines & evidence based medicine– Advantage Suite with MEG, DCGs, Patient Health Record 2009 Thomson Reuters– Physician Performance Assessment Module40HEALTHCARE PAYER SOLUTIONS
PHYSICIAN PERFORMANCE ASSESSMENT:CORE METHODS & CAPABILITIES Efficiency (Affordability) Measures– Medical Episode Grouper (MEG)– Disease Staging Severity Model– DCG Risk-AdjustedThomson ReutersAnalytics 2009 Thomson Reuters Effectiveness (Quality) Measures– Nationally adoptedevidence-based measures– Custom measures as appropriate Analysis and Reporting– Physician Identification– Physician Attribution– Other Methods and Analytics– Measure Reliability and Stability– Reporting and Distribution41Proven, Fair, CredibleMethods forPerformance EvaluationHEALTHCARE PAYER SOLUTIONS
A FRAMEWORK FOR PHYSICIANPERFORMANCE sessment Quality Measures- Numerator- Denominator 2009 Thomson ReutersReporting Denominator- Episode Grouper- Episode Severity- Patient Risk (comorbidities) Numerator- Utilization & Cost Measures Physician Identificationand Attribution Outlier Exclusion Volume Thresholds Composite Scores42HEALTHCARE PAYER SOLUTIONS
Thomson Healthcare’s Intelligence: EBMClaims Administrative RulesDetermination of AppropriatenessSets of procedures and billing activitiesgoverning the administrative rules for trative RulesPeer Group Practice NormsPeer Group NormsComparisons among providers or patients that identifydeviations from peer group normative behaviorEvidenceBasedMedicineEvidence-Based Medicine 2009 Thomson ReutersThe conscientious and judicious use of current best evidence fromclinical and outcome research for the management of individualpatientsGoldStandard43HEALTHCARE PAYER SOLUTIONS
Predictive Modeling in Program Integrity There is no application that can “predict” future fraud and abuse– Providers and Beneficiaries cannot be prosecuted for future possibilities 2009 Thomson Reuters When are Program Integrity and Predictive Modeling linked?– By looking at past experience states can predict which types of providerservices, which regions of the state, or other variables that predict morelikely yields of fraud or abuse cases This type of predictive modeling definition is currently beingpopularized in law enforcement for deployment of police to areas ofthe city that have a history of particular crimes at particular times.– Compiling several red flags or indicators of potential F&A and applying ascore to a provider over the multiple indicators– Prepayment flags that scored providers in various levels of upcoding,unbundling, or improper billings only look at incoming claims and don’tlook at the whole picture of paid claims across all databases– Prepayment Editing predicts inappropriate billings and denies the claimsbefore payment44HEALTHCARE PAYER SOLUTIONS
2009 Thomson ReutersQuestions & Discussion45HEALTHCARE PAYER SOLUTIONS
Contact:David NelsonDirectorThomson Reuters(734) 913-3432 Direct(734) 913-3338 Fax 2009 Thomson ReutersDavid.L.Nelson@ThomsonReute
Michelle McAllister, Consulting Manager, Thomson Reuters 2009 Thomson Reuters. 2. HEALTHCARE PAYER SOLUTIONS. AGENDA Thomson Reuters Using Predictive Models to Move Medicaid Providers Toward Best Practices and Reduce Waste Questions and Discussion. . Formulate payment policy .