Transcription
Point of Service CollectionsTuesday, October 18, 201610:40 a.m. - 11:40 a.m.Jeff Darling, CHAMManager, Patient Access Service CenterOneida HealthcareScott DalgetyVP of Client ServicesAccuReg
SpeakersJeff Darling, CHAMManager, Patient Access Service CenterOneida HealthcareScott DalgetyVP of Client ServicesAccuReg
Liability Shift from Payer to Patient Revenue MixBefore ACA10%PatientAfter 3
What are POS Collections? Point of Service Collections POS, TOS, Pre-service, Up-front, Front-end Various definitions: Prior to ArrivalPoint of ServicePoint of Service up to DC datePoint of Service up to x days after dischargeMay include outstanding balances and bad debt recoveries4
NAHAM Definition NAHAM Definition of POS Collections: Any and all collections posted by Patient Access prior to and includingdischarge date. This includes: Collections from self-paysCollections from insured patients (copay/deductible/co-ins)Initial payments collected for approved payment plansPrior balances and bad debt accounts5
Why are POS Collections Important? 70% chance of collecting at point of service (30% after discharge) Academy for Healthcare Revenue, 2014 The majority of patients are willing to pay when they need the service Reduce the cost of billing Reduce bad debt Correctly identify charity Accelerate cash flow for financial viability6
Why Estimate and Collect at POS? 30% of revenue now comes from patients Patients want price transparency and comparison Patients want to know their cost after insurance Patients don’t like surprise bills Estimates enable financial assistance discussions Estimates reduce patient financial stress Easier to collect up front than after service Likelihood of collecting is greatest at POS Cost to collect is lowest at POS7
NAHAM Pre-Registration Process Tiers8
POS Collections PotentialNAHAM AccessKeys 3.0ID#ID#DOMAINDOMAINAccessKey (KPI)AccessKey ation MiddleMiddleImplementation MatureMatureImplementationImplementationPhaseor ManualProcessor orSemi-AutoPhasePhaseor ManualProcess hmarksrepresent progressivephasesto achievinga to achievinga PatienthighAccessteam andPatientare largelydependentthearelevelof executivesupport,andboardperformingAccessteam onandlargelydependentoncommunitythe level ofexecutiveadoption, available technology, staffing, processes and use of best ctionsPOS-4POS-4CollectionsCollectionsPOS Collections to RevenuePOS Collections to RevenuePOS Collections toPOS CollectionstoTotalPatient CollectionsTotal Patient CollectionsPOS Collection OpportunityPOS CollectionRateOpportunityRateTotal POS Dollars CollectedTotal POS Dollars CollectedPOS-5POS-5CollectionsCollectionsPOS Collected Accounts RatePOS Collected Accounts RatePOS-6POS-6CollectionsCollectionsEstimate to Registration RateEstimate to Registration racyRateEstimationAccuracyRatePOS CollectionsPOS CollectionsNet PatientService RevenueNet PatientServiceRevenuePOS tal Patient CollectionsPOS CollectionsPOS EstimationsCollectionsPOSPOS EstimationsTotal Dollars CollectedTotalDollars Collected( DischargeDate)( Discharge Date)Accounts CollectedAccounts CollectedTotal Registrations*Total RegistrationsEstimates GeneratedEstimates GeneratedTotal Registrations1Total RegistrationsAccurateEstimatesAccurate EstimatesQualifiedEstimatesQualified Estimatessupport, community and board adoption, available technology, staffing, processes anduse of best 0%30%30%45%45%60%60%Total POS Cash Collected compare to prior periodsTotalPOSorCashCollectedforcompareto prior periods(no ratiobenchmarkpeer comparison)(no ratio or benchmark for peer 85%90%90%95%95%9
Financial Impact Revenue Generation: Earlier cash Prior balance resolution Divert bad debt Expense Reduction: Cost to collect Time value of money Early out and collections fees10
NAHAM POSC Best Practices1.Establish a Baseline ‐ What are your average POS collections permonth? By Location?2.Identify Gaps - Assess the current POS collection policies, practices,training needs and technology at each Patient Access location (ED,Surgery, Outpatient, Pre-Reg, etc.)3.Provide staff with - Patient liability estimation and payment toolsand training on insurance terminology and calculation of copay,deductible and coinsurance.11
Estimator System Questions Automated? (from scheduled procedures)Accurate? (POS-7 Estimation Accuracy Rate 85% 10%)Workflow: Alerts & Scripts?Employee and/or patient facing (kiosk/portal/mobile)?Integrated with payment processing?POS collections reporting?Integrated financial assistance scripting? Payment options personalized to each patient Line up with the hospital’s Financial Assistance Policies Charity Care, Payment Plans, Discounts, Loans Integrated Payment Processing?12
Payment System Questions E-cashiering? Auto-post payments via 835? Patient payment portals andmobile apps Reconciliation reporting? Integration to estimation tools Multiple payment methods? Credit/debit/ACH/cashFlexible payment plansPrompt pay discountsPatient loans (bank vs hospital) To save time and errorEstimate to payment KPI reporting Retail and EMV?13
Payment System Questions Monitoring Dashboards Public Display14
SegmentationLittle ability to payStrong ability to payNo available credit,low credit scoreCredit availablePotential charitycare or MedicaidIdentity issuesIncorrect dataPotential fraudCollect payment at time ofserviceBorderline ability to payHigh credit scoreConsider forfinancing solutions15
Ability and WillingnessFPLCredit Score16
The Affordability Tipping 8001900200017
NAHAM POSC Best Practices4.Train Staff - How to collect effectively (soft-skills customer training) with scripting,objection handling, and financial assistance options they can offer patients which arepre-approved by the hospital’s financial assistance policies (FAPs).5.Develop Collection Policies - Empower registrars to offer discounts, payment plans,loans and charity for those who qualify, and provide them with clear parameters toreschedule non-urgent services for patients that decline financial assistance.6.Foster a Collections Culture - With support from the Board, Executives, Managementand Physicians, where every registrar asks at every opportunity, of every patient withan estimated liability, at every location and every time.18
NAHAM POSC Best Practices7.Continually Raise the Bar - After goals are met, but keep goalsattainable.8.Implement Incentives - These can be non-financial (recognition, parties,etc.) or financial (depending on facility).9.Engage Physicians and Office Managers - To set expectations at orderingand scheduling levels.10.Monitor POS Collections Performance - On a monthly, weekly and dailyat four levels; health system, facility, location and employee, using all 7POS Collections AccessKeys.19
Oneida HealthcareJeff DarlingManager, Patient Access Service Center20
BackgroundOneida Healthcare (OHC) is a 101bed acute care hospital and a 160bed extended-care facility (ECF) andshort-term rehab facility licensed bythe State of New York and operatedby Oneida Health Systems, Inc., aNew York not-for-profit corporationand Joint Commission accredited.21
Background 4 Primary Care Health Centers1 Maternal Health Clinic4 Outreach Laboratory Draw StationsPhysical Therapy Center2 Offsite Imaging CentersQuick Care CenterSleep Study and Pulmonary FunctionTesting Neurology Services, OrthopedicSpecialists and ENT Specialists22
Organizational Structure Decentralized – oversight of: Main reg ED Pre-reg Authorization team 28 FTE’s, 1 team leader, 1 certified application counselor and director23
Get Started – Why Wait? Don’t procrastinate – Get started today Track manually or via technology, if available Release results monthly – Department-specific as well as on an individual level Creates healthy competition Don’t need to have monetary incentive – Can provide small tokens of recognition. Dress down day, free lunch, certificate Top collector, most improved, etc. Empower a preceptor or a champion who has experience collecting – I don’t have one? Lead by example – show them how25
Takes Off Like Wildfire Start in your direct areas of responsibility Will spread to outside areas Bring back to rev cycle meeting Bring in departments to assist in collection efforts Educate patient via Pre-Registration process Inform patient of responsibility Attempt to collect over phone at that time Patient must stop at cashier or reg on day of service Work with greeter or security (front desk) to direct patients26
Identified Need for POS CollectionsFour years ago brought forth the concept to collect POS Collections was an opportunity for revenue Needed technology for efficiencies Verifying eligibility New management supported POS collections to collect Lack of education – no scripting Resistance (reg, patients and nursing) Lack of support from previous leadership Needed a system to track results – manual Accelerate patient registration times27
Project Prerequisites and Goals Verify eligibility How to check eligibility How to interpret responses Staff education Clinical and non-clinical Support from departmentmanagers Manual versus automatedprocess Labor intensive and time consuming Scripting Reporting and recognition Needed a champion28
Changes Made Automated Registration QA – 2014 Automated Eligibility Verification – 2015 Automated Estimation – 2016 Integrated Payment Processing – 2016 Began Staff Training on POSC – 201629
Changes Made Implemented Quality Assurance Tool – 2014 Implemented New Eligibility Tool linked directly to QA – 2015 Implemented Estimation Tool – Also linked to same application –4/2016 All while still driving POS collections in an upward trend Staff education must focus on their role and the importance registration playsin the rev cycle30
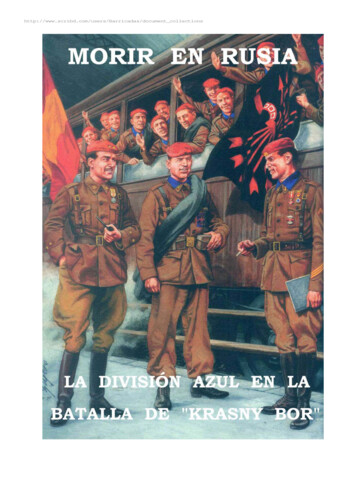
POS Collections March 2016Main Reg & ER1st ShiftLinda ShafferBonnie StarkeyTina Dillman (per Diem)Alexandra NicholsonChristine WoodAlyssa CollinsHeidi Wilson-MinerNoel Coe (DOH 4/4/16)Total 1st ShiftMonthlyRegistrarResults2nd ShiftMaureen CaraherCourtney NetzbandPam StaudtMargaret Reese (PT)Rose Lomonaco (per Diem)Karen StearnsPatricia CrossBrandie Stevenson (PD)Total 2nd ShiftPre- RegistrationCindy Crill (Pre Reg)3rd ShiftSuzanne Robles (PT)Lindsay RosselloElla BowmanTeri SecordWendy NetzbandTotal 3rd ShiftGoalsAmount Collected 3,323.47 1,493.07 1,999.31 1,561.55 2,695.34 1,347.35 2,934.57Number Collected Monthly Goal 1st ShiftAvg Daily Collections(31)38 's over Goal18% over / under Goal2720411926 15,354.66189 1,039.0015 65.00 615.30 290.00 505.00 858.00 2,237.0029281231 5,609.3079 920.0011 210.002 243.00 215.00 100.00 240.00 1,008.00421514 15,000.00 495.31 354.66Monthly Goal 2nd ShiftAvg Daily Collections(31) 's over Goal% over / under Goal 6,000.00Monthly Goal Pre-RegAvg Daily Collections(31) 3,000.00Monthly Goal 3rd ShiftAvg Daily Collections(31) 's over Goal% over / under Goal 1,500.00 180.93- 390.70 26.67 32.51- 492.0031Grand Total Registration 29,509.26386
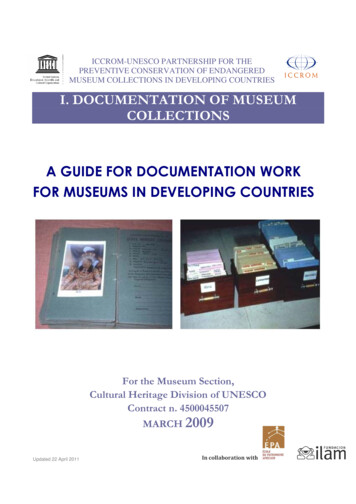
POS Collections to RevenueAccessKey POS-1 Goal 1% 6,000,0000.6% 5,000,0000.5% 4,000,0000.4% 3,000,0000.3% 2,000,0000.2% 1,000,0000.1% Aug-15Sep-15Oct-15Nov-15Dec-15Jan-16Feb-16POS to Rev32
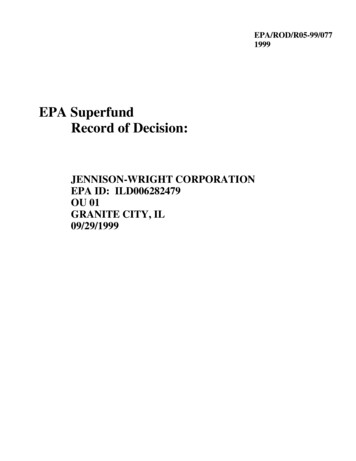
Total POS Dollars CollectedAccessKey POS-4 40,000 35,000 35,025 30,000 27,294 25,000 23,789 20,840 20,000 15,000 14,676 20,784 25,824 19,382 18,096 14,566 12,910 10,000 5,000 Jan-15Feb-15 Mar-15 Apr-15 May-15 Jun-15RegistrationJul-15Aug-15Emergency DeptSep-15Oct-15RadiologyNov-15 Dec-15Jan-16Feb-16 Mar-16 Apr-16Total POSC33
Future Goals Achieve 1% (Good – NAHAM KPI #1) of net patient revenue by12/2016 Achieve 1.5% standard (Better) by 6/2017 Implement POS collection incentive by 6/2016 Track NAHAM KPI #3 – POS Collection Opportunity Rate –Collections/Estimates34
Questions?Jeff Darling, CHAMManager, Patient Access Service CenterOneida Healthcarejdarling@oneidahealthcare.orgScott DalgetyVP of Client ServicesAccuRegsdalgety@accuregsoftware.com
Academy for Healthcare Revenue, 2014 The majority of patients are willing to pay when they need the service Reduce the cost of billing Reduce bad debt Correctly identify charity . in the rev cycle 30. 31 Monthly Registrar Results POS Collections March 2016 Main Reg & ER Goals