Transcription
Central East CommunityCare Access CentreOutstanding careevery personevery day
Who are we?The Central East Community Care Access Centre (CECCAC) is one of 14CCACs that work in communities across Ontario to connect people with qualityin-home and community-based health care. We make sure our patients receivethe care they need when they need it. We provide information, direct access toqualified care providers and many comprehensive services to help people comehome from the hospital sooner or live independently at home longer.Finding and accessing care can sometimes be confusing and complicated.CCACs help people find their way through Ontario’s health care system,understand their options and get the highest quality care possible. We helppeople across their life spans from school children who have special healthneeds to seniors who need health services at home or access to a long-termcare home.Every day in communities across the province nurses, doctors, therapists,personal support workers, care coordinators and many others are workingtogether to provide better quality of care for our patients. The CCACs work asa team along with our health care partners to transform our health care systemin order to deliver the health care that people need.Central East CCAC
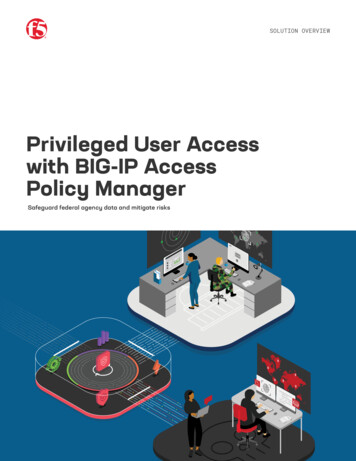
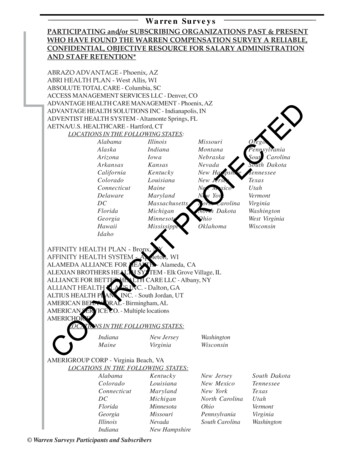
TheHealthSectorsof OntarioCentral East CCAC
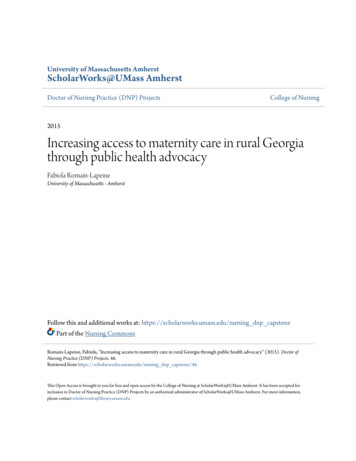
Central East CCAC RegionThe Central East CCAC shares the sameboundaries as the Central East LocalHealth Integration Network (LHIN),stretching from Victoria Park inScarborough, north to Algonquin Park inHaliburton County and to Lake Ontarioalong the southern border. There areseven branch offices:1.2.3.4.5.6.7.Central East CCACCampbellford BranchHaliburton BranchLindsay BranchPeterborough BranchPort Hope BranchScarborough BranchWhitby Branch (Head Office)
Our ServicesCentral East CCAC services are paid for by the Ministry of Health andLong-Term Care and can include: Linking patients to a wide range of community servicesnot directly provided by the Central East CCAC A range of in-home health care and relatedsocial services and supplies and equipment Specialized programsCentral East CCAC
Who can make a referral for service?Referrals to the Central East CCAC can be made by: individuals family members caregivers friends physicians health care professionalsCentral East CCAC
What We DoCentral East CCAC Care Coordinators are dedicated nurses,occupational therapists, social workers and other health careprofessionals who work directly with patients in hospitals, doctors’offices, communities and at home to ensure that people get the carethey need.Central East CCAC
What services are available? Care CoordinationCentral East CCAC Care Coordinators are regulated health careprofessionals with specialized knowledge and skills that helpassess the patient’s needs, assist them in developing a careplan and arrange for the services required. In-Home NursingPhysiotherapyOccupational therapySpeech-language therapySocial workDieteticsMedical supplies and equipmentPersonal support (bathing, dressing etc.)Central East CCACHC
Who is eligible for our service?To be eligible for services, you must have:In-Home Services or Alternate Care Setting (ACS) a valid Ontario Health Card health care needs that cannot be met on an outpatient basis a need for a least one professional or personal support service a medical condition that can be adequately treated in the homeor ACSPlacement a valid Ontario Health Card be 18 years of age or older a need for either nursing care 24 hours a day, assistance withactivities of daily living or on-site supervision or monitoring must have care needs that can be met in a Long-Term CareHomeCentral East CCAC
PlacementWhen living independently is no longer possible, the CentralEast CCAC co-ordinates applications to long-term care homes.The Care Coordinator will: provide information about long-term care determine eligibility for placement provide assistance in theapplication processHCCentral East CCAC
Specialized ProgramsThe Central East CCAC may also offer assessment forand referral to specialized programs geared to specifichealth needs.Programs include:Acquired Brain InjuryConvalescent CareAssisted Living for High Risk SeniorsBehavioural Supports OntarioCentre for Complex Diabetes CareCentralized Diabetes IntakeCentral East LHIN Self-ManagementCommunity Palliative Nurse PractitionerHealth Care ConnectMental Health and Addiction NursesNurse Practitioners Supporting Team AvertingTransfers (NPSTAT) Rapid Response Nurses Central East CCAC
Information and ReferralIf a patient is not eligible for the services provided by theCentral East CCAC, our staff will link them to alternate servicesavailable in the community.These services may include: some adult day programs meal delivery services transportation assistance assistance with shopping and cleaningNote: You may be required to pay a fee for servicesprovided by a community service agency.Central East CCAC
Health Care ConnectThe Health Care Connect program is part of the Ministry of Healthand Long-Term Care, and was created to help people who arewithout a family health care provider to find one.The program identifies doctors or nurse practitioners in yourcommunity who are accepting patients and links them to peoplewho are in need of a family health care provider.www.ontario.ca/healthcareconnect800 445 1822Once you have joined Health Care Connect, a Central East CCACCare Connector will be assigned to help you find a health careprovider in your area.Central East CCAC
Call: 310-2222 or visit: www.centraleasthealthline.caCentral East CCAC
Campbellford Branch:119 Isabella Street, Unit 7Campbellford ON K0L 1L0705-653-1005Port Hope Branch:151A Rose Glen RoadPort Hope ON L1A 3V6905-885-6600Haliburton Branch:PO Box 793, 13321 Hwy 118Haliburton ON K0M 1S0705-457-1600Scarborough Branch:100 Consilium Place, 8th FloorScarborough ON M1H 3E3416-750-2444Chinese Line: 416-701-4806Lindsay Branch:370 Kent Street West, Unit 11Lindsay ON K9V 6G8705-324-9165Peterborough Branch:700 Clonsilla Avenue, Suite 202Peterborough ON K9J 5Y3705-743-2212Whitby Branch:920 Champlain CourtWhitby ON L1N 6K9905-430-3308Toll-free: 1-800-263-3877TTY Line: 1-877-743-7939Website: www.ce.ccac-ont.caCentral East CCAC
Children/School HealthSupport ServicesThe School Health Support Services program providesservices to assist students with medical and/or rehabilitationneeds that are beyond the range and responsibilities of schoolstaff. Through this program studentsare able to attend schoolalong with their peers.The Children’s In-HomeServices provides servicesto children/youth up to18 years of age whilein their home.Central East CCAC
Home First Philosophy A philosophy that promotes safe and timely care to meethealthcare needs of patients and families in the mostappropriate setting. A partnership among Central East LHIN, hospitals, CECCACand Community Support Services. A system of people, processes and services to returnpatients back into the community. Overall tenets of Home First: Every patient admitted to the hospital will bedischarged home Decisions about major changes in lifestyle should bemade from home, not from hospital.Central East CCAC
What are the benefits to patients? Patients are in their own home where they want to be. Patients’ health, independence and well-being are maintainedlonger. The risk of patients getting a hospital acquired infectionis reduced. Patients and caregivers are able to receive the benefit ofservices offered by CECCAC and community support agencies. Patients and families are able to make life-changing decisionsrelated to future living accommodations from the comfort oftheir own home – returning back into the community.Central East CCAC
Alternate Care Setting (ACS) Clinics are available for CCAC clients who require nursing care and areambulatory Clinics are open 8:30 a.m. to 8:30 p.m., 365 days of the year Clients book their own appointmentNursing care provided can include: Wound care/dressing changes, including NWPT Therapy IV Therapy Subcutaneous injections (including any Low Molecular Weight Heparininjections for Deep Vein Thrombosis) Intramuscular injections Central Venous Line flushing, such as PICC, Hickman, Port-a-cath. (Blooddraws if in conjunction with PICC Lines) Blood Pressure Monitoring/Cardiac Assessment – based on changes instatus due to medication adjustments or cardiac assessment Chemo de-accessing (required only after Chemo Clinic is closed) Catheter care; includes catheter changes, nephrostomy care, intermittentcatheterization (excludes teaching of self- catheterization).
Assisted Living Services for High RiskSeniorsThe “Assisted Living Services for High Risk Seniors, 2011” project in the CELHIN addresses the needs of high risk seniors who can reside at home butrequire the availability of personal support, homemaking, security checks andreassurance services on a 24/7 basis. The project will target high risk seniorswhose needs cannot be met in a cost effective manner through home andcommunity care services provided solely on a scheduled visitation basis.Assisted Living clients are eligible for combined maximum of 180 hours ofpersonal support, homemaking, and professional services per month, it is theintent of this program that no person shall exceed 90 hours of personalsupport service per month
Behavioral Supports OntarioBehavioural Supports Ontario (BSO) was first announced by the Ministry ofHealth and Long Term Care in August 2011. BSO is a comprehensive systemredesign that enables the breakdown of barriers, encourages collaborativework, shares knowledge and fosters partnerships to ensure people are treatedwith dignity and respect in an environment that supports safety and highquality care.The goal is to enhance the health care services of seniors, their families andcaregivers who live and cope with responsive behaviours associated withdementia, mental illness, addictions and other neurological conditions, whenthey require it and wherever they live whether that be at home, Long-TermCare or in the community. Phase 1 -Long-Term Care Homes (LTCHs) Spread –starting within 13 Early Adopter LTCHs and moving to all 68 LTCHs.Phase 2 -Community Spread –begin with a few staff within communityagencies and spread to all agencies and staff.
Centre for Complex Diabetes Care The Ministry of Health and Long-Term Care has provided funding for newRegional Centres for Complex Diabetes Care (CCDC) in the Central East andin other parts of the province. The Central East CCDC has been establishedin three sites located at Peterborough Regional Health Centre, LakeridgeHealth Whitby, and The Scarborough Hospital. When fully operational, theCentre will offer care to patients with diabetes who have complex healthissues and support needs beyond what can be provided in a primary caresetting or through a Diabetes Education Program (DEP). A typical patient would be one who, because of social, mental health,and/or extensive co-morbidity factors, is not achieving diabetes goalsdespite his/her caregiver’s best efforts. This person would come under thecare of a dedicated team at each CCDC site, led by a Nurse Practitioner thatdraws expertise from a range of professionals including a social worker,nurse, dietician and pharmacist. Appropriate specialists would be consultedwhen advisable.
Centralized Diabetes Intake A more streamlined and integrated service for the intake and referral ofpatients living with diabetes has been expanded for the Central East region. The Centralized Diabetes Intake, supports the Ontario Diabetes Strategy toimprove care for Ontarians living with diabetes. It is anticipated thatimproved access to diabetes care and services will decrease emergencydepartment visits and hospital admissions for people living with diabetes. The Central East CCAC will support intake and patient referrals to existingDiabetes Education Programs and the Central East CCDC. The CCAC hasboth the mandate and infrastructure to support centralized intake andreferrals and can also offer patients help with health system navigation. The Centralized Diabetes Intake has one number to call and a common referral form.Toll free number 1-888-997-9996Referral fax number 905-444-2544
Community Palliative Nurse PractitionerProgramThe Community Palliative Nurse Practitioner Program (CPNP) is a programsupporting individuals and their families in the community living with aterminal condition. CPNPs have expertise providing palliative care in client'shome.What Community Palliative Nurse Practitioners Do: Visit palliative clients in their home while working in partnership with thevisiting nursing staff and the health care team Provide an opportunity and support the client’s wish to die at home Provide physical, emotional, psychological and spiritual support Serve as a source of education and support for client, family and careproviders Help diagnose health problems, provide treatment for pain and othersymptoms
Nurse Practitioners Supporting TeamAverting Transfers (NPSTAT) Reducing and preventing avoidable emergency department transfers ofLong-Term Care Home residentsProviding acute and episodic care referrals to LTCHs throughout the CentralEast LHINReducing the number of Alternate Level of Care (ALC) daysFacilitating and supporting the return of hospitalized residents back to theirLTCHs.Providing primary health care services to unattached frail seniors 70 Building capacity, knowledge and skills of LTCH staff
Services Available (NPSTAT) Diagnose and communicate a diagnosis Order prescriptions,laboratory tests, authorize various assistive devices and formsBladder scansInitiate and order IV solutions and drugsHypodermoclysis for rehydrationVenipuncturePercutaneous draining tubesCentral venous access devices (e.g., PICC line)Order diagnostic tests (ECGs, Ultrasonography & X-Ray)Certify Death (Certificate of Death - Form 16)Sharp debridement of woundsGastrostomy tube (G-Tube) replacementReferrals: OT, PT, RD, SLP, Pharmacist, Social Work, Chaplin, Palliative andMedical Specialists, High Intensity Funding
Rapid Response Nurses (RRN)The Rapid Response Nurses will: Provide professional settlement services which includes an in-home visit 24hours post-acute discharge, medication reconciliation, contact with theprimary care provider to provide a health care update, review the courseof stay in hospital and discharge summary, and to discuss the plan of care. The RRN would also be responsible for arranging an appointment with theprimary care provider so that the client will be seen within five to sevendays of discharge from hospital. will collaborate closely with the CCAC Care Coordinators both at thehospital and in the community The RRN will not be utilized as a substitute for our contracted NursingProviders.
Mental Health and Addiction NursesThis program was created to support District School Boards to build capacityto recognize and respond to student mental health and addiction issues.These nurses are an integral part of an interdisciplinary District School Boardbased team of mental health leaders, community mental health workers, andexisting District School Board staff that will work together to provide earlyidentification and intervention services and supports to students who havemental health and addiction issues.The focus of the program is to support students transitioning from hospitalback to school and to provide education on mental health promotion,resiliency, skill development for the student population where required asidentified by the school boards.Referrals for this program are accepted from the hospital, school teams or theschool administrators only.
Self-Management - Living a Healthy LifeThe Central East LHIN Self–Management Program, Living aHealthy Life offers Self-Management Workshops whichempowers people to develop new tools and skills to break the cycleof symptoms that can result from chronic conditions, diabetes orpain. Six consecutive weeks 2 ½ hours per week Peer volunteer lead All materials are supplied Free Family members and caregivers are welcome Workshops are available in English, French, Tamil and ChineseFor workshop schedules contact:www.healthylifeworkshop.caCentral East CCAC
Choices and ChangesChoices & Changes is a workshop created by the Institute for Health CareCommunication and accredited by the College of Family Physicians of Canada(CFPC). This workshop is designed to acquaint participants with the literature,theory and techniques for promoting change in health behaviours.By the end of the workshop participants will be able to: Describe the role of the clinician as a facilitator of change Assess patients' conviction and confidence to engage in health behaviourchange Describe two skills to influence change in patients' health behaviours Demonstrate two techniques to use in clinical settings to influence changeand promote adherence to treatment plansWorkshops are offered at no cost to clinicians and are sponsored bythe Central East LHIN Self-Management Program.Clinicians who successfully complete the training will be eligible for acertificate and CFPC Mainpro-1 credits.
CCAC Vision and MissionOur VisionOutstanding care - every person, every dayOur MissionTo deliver a seamless experience through the health system forpeople in our diverse communities, providing equitable access,individualized care coordination and quality health care.Central East CCAC
On a day-to-day basis, we are: an easy to use gateway to information and high quality healthservices; an innovator seeking to optimize people's health, well-being andautonomy; an integrator partnering with others to reduce the barriers toaccess, respect diversity and improve the care experienceof people across the health care continuum; an employer of choice who believes in the remarkable capacityof our people to continuously learn and make a difference; an open communicator who promotes positive relationships;and a steward of public resources who is openly accountable andcontributes to a sustainable health system.Central East CCAC
Our ValuesCaringWe relate to each other, to those we serve and to those with whom we workwith compassion, respect, integrity and fairness and value the contribution ofeveryone.ExcellenceWe base our decisions on ethical principles and best available information andour actions on best practice.Centered on the PatientWe encourage and promote personal responsibility and informed andparticipative decision-making.CollaborationWe co-ordinate our efforts, working in partnership with colleagues, patients,families, caregivers, providers and the community.AccountableWe manage resources responsibly, share performance related information freely,and foster a culture of open communication.Continuous ImprovementAs a learning organization, we foster a spirit of inquiry, committed to improvingunderstanding and encouraging innovation.
Central East CCAC Facts and Stats The Central East CCAC is one of 14 CCACs in Ontario The Central East CCAC, formally established on January 1, 2007,is the result of the alignment of the following predecessor CCACs:Durham Access To Care, Haliburton, Northumberland and VictoriaAccess Centre, Peterborough Community Access Centre, andScarborough Community Care Access Centre The Central East CCAC has seven branches: Campbellford,Haliburton, Lindsay, Port Hope, Peterborough, Scarborough, andWhitby. Staff members are also located in a number of satelliteoffices in hospitals, family health teams, physician offices andlong-term care centresCentral East CCAC
Central East CCAC Facts and StatsThe Central East CCAC is the: Sixth largest CCAC based on geography coveringapproximately 16,673 square kilometres Second largest based on a population of approximately1
Specialized Programs The Central East CCAC may also offer assessment for and referral to specialized programs geared to specific health needs. Programs include: Acquired Brain Injury Convalescent Care Assisted Living for High Risk Seniors Behavioural Supports Ontario Centre for Complex Diabetes Care