Transcription
Using root cause analysistechniques in clinical auditFebruary 2016produced for HQIP byUsing root cause analysis techniques in clinical audit Copyright HQIP 2015
A collaborative document produced by the Healthcare Quality Improvement Partnership (HQIP) and Clinical Audit Support Centre (CASC).Author:Stephen Ashmore and Tracy RuthvenDirectors:Clinical Audit Support CentreProduction:Mandy Smith, Kim Rezel, Simon Marrow,Sally Fereday, Tosin EniadeProject managers: HQIP2Acknowledgements:CASC would like to thank members of the clinical audit teamsat Mid Cheshire Hospitals NHS Foundation Trust and Norfolkand Suffolk NHS Foundation Trust for kindly supplying localcase studies for this guide. We would also like to thank LouiseHazelwood for her support and all those who attended the HQIPFirst published: May 2015ISBN NO 978-1-907561-06-1 2015 Healthcare Quality ImprovementPartnership Ltd (HQIP)Design: Pad Creative www.padcreative.co.ukRCA training workshops in 2014-15 for their ideas and input. Wehave used templates and methodologies from the National PatientSafety Agency, The Health Foundation, Institute for HealthcareImprovement and the NHS Institute for Innovationand Improvement throughout this guide.Using root cause analysis techniques in clinical audit Copyright HQIP 2015
Contents3Section one5Introduction5About HQIP5About Clinical Audit Support Centre5The aim of this guide5Using this guide5What is root cause analysis (RCA)6Understanding the RCA process6RCA tools and techniques featured in this guide6Section two: RCA tools and techniques71. Brainstorming (structured and unstructured)-- Definition/explanation of the technique-- How brainstorming techniques are used in relation to patient safety-- How brainstorming techniques can be used to add value in clinical audit-- Examples of how brainstorming techniques have been used in clinical audit777782. Brainwriting-- Definition/explanation of the technique-- How brainwriting techniques are used in relation to patient safety-- How brainwriting techniques can be used to add value in clinical audit-- Examples of how brainwriting techniques have been used in clinical audit9999103. Cause and effect diagram-- Definition/explanation of the technique-- The four stages in creating a cause and effect diagram-- How cause and effect diagrams are used in relation to patient safety-- How cause and effect diagrams can be used to add value in clinical audit-- How cause and effect diagrams have been used in clinical audit1111121212124. Change analysis-- Definition/explanation of the technique-- The four stages involved in conducting change analysis-- How change analysis is used in relation to patient safety-- How change analysis techniques can be used to add value in clinical audit-- Examples of how change analysis techniques have been used in clinical audit1414141414155. Five whys-- Definition/explanation of the technique-- The two stages involved in conducting the five whys-- How the five whys technique is used in relation to patient safety-- How the five whys technique can be used to add value in clinical audit-- Examples of how the five whys have been used in clinical audit161616161717Using root cause analysis techniques in clinical audit Copyright HQIP 2015
46. Mapping techniques-- Definition/explanation of the technique-- How mapping techniques are used in relation to patient safety-- How mapping techniques can be used to add value in clinical audit-- Examples of how mapping techniques have been used in clinical audit19191919207. Nominal group technique (NGT)-- Definition/explanation of the technique-- The four stages for conducting NGT-- How NGT techniques are used in relation to patient safety-- How NGT techniques can be used to add value in clinical audit-- Examples of how NGT techniques have been used in clinical audit2222222323238. Pareto analysis-- Definition/explanation of the technique-- The three stages of Pareto Analysis-- How Pareto analysis is used in relation to patient safety-- How Pareto analysis can be used to add value in clinical audit-- Example of how the Pareto analysis has been used in clinical audit2525252727279. Process mapping-- Definition/explanation of the technique-- How process mapping is used in relation to patient safety-- How process mapping can be used to add value in clinical audit-- Examples of how process mapping has been used in clinical audit282829292910. Run charts-- Definition/explanation of the technique-- How run charts are used in relation to patient safety-- How run charts can be used to add value in clinical audit-- Examples of how run charts have been used in clinical audit3030313131Further reading list and references34Using root cause analysis techniques in clinical audit Copyright HQIP 2015
Section oneIntroductionAbout the authorsImproving the quality of clinical services requires change.The key to successful clinical audit – or any other qualityimprovement project – is deciding what changes arenecessary, and which will be most effective in bringing aboutimprovement. Firstly, it is necessary to understand whyproblems identified through clinical audit exist and requirechange. Clinical audit data can show what the problemshave been, but understanding why they have occurred is notalways straightforward.The Clinical Audit Support Centre (CASC) is an independentlimited company responsible for providing best practice andsupport in clinical audit. They assist healthcare professionalsand teams to undertake a wide range of quality improvementinitiatives. They also help clinical teams deliver safe andeffective care and provide accredited training in clinical audit,significant event audit and root cause analysis. The CASCwebsite is www.clinicalauditsupport.comRoot cause analysis techniques are used in healthcare toinvestigate adverse incidents but those same techniques canbe used in clinical audit to reveal the underlying failures thatneed to be addressed to bring about improvement.This guide aims to improve patient care and clinical auditdelivery by providing practical advice on how establishedroot cause analysis (RCA) techniques can ‘add value’ toclinical audit. The guide is primarily aimed at clinical auditprofessionals and healthcare staff that participate in clinicalaudit initiatives at both a local and national level.The Healthcare Quality Improvement Partnership hascommissioned the Clinical Audit Support Centre to producethis guide in order to demonstrate how these techniques canbe used in clinical audit.This guide can be read in conjunction with HQIP Guide to usingquality improvement tools to drive clinical audit.1 It should alsobe noted that root cause analysis and some of the techniquesdescribed below can also be used as quality improvementtechniques in their own right, see the Guide to qualityimprovement methods.2About HQIPThe Healthcare Quality Improvement Partnership is anindependent organisation led by the Academy of MedicalRoyal Colleges, The Royal College of Nursing and NationalVoices. We were established in April 2008 to promote quality inhealthcare, and in particular to increase the impact that clinicalaudit has on healthcare quality improvement.The aim of this guideUsing this guideThis guide focuses on how different RCA techniques can beincorporated into the clinical audit process. Each sectiondetails an established RCA technique and provides: A definition/explanation of the RCA technique Details of how the technique is applied to patient safety Details of how the technique could be applied toclinical audit An example of how the technique has been applied toclinical audit Signposting to useful resources A number of templates used throughout this guide are freeto download from hqip.org.uk for local adaptions 3This guide draws on best practice in RCA with a view toexplaining how RCA techniques can be adapted and used in aclinical audit setting.1. it/2. improvement-methods/5Using root cause analysis techniques in clinical audit Copyright HQIP 2015
What is root cause analysis?Understanding the RCA processThe origins of RCA are found in the manufacturing industry,with the five whys technique developed by the Japaneseinventor Sakichi Toyoda in the 1930s. In subsequent yearsRCA techniques have evolved considerably and becomeincreasingly sophisticated.NPSA guidance advocates a seven-step process to conduct afull RCA investigation. The stages are as follows:1. Identifying which incidents should be investigated2. Gathering the information3. Mapping the eventsFollowing the publication of the Chief Medical Officer’sOrganisation with a Memory in 2000, the National PatientSafety Agency (NPSA) (established 2001 and dissolved in 2012)created a range of RCA resources and encouraged healthcareteams to adopt its methods.4. Analysing the informationThere are many definitions of RCA, but essentially it is aproblem-solving technique, however, unlike clinical audit, it isnot a singular systematic process but instead an approach thatcan draw on many different tools, processesand philosophies.The NPSA created a number of excellent resources anddocuments that focus on how to conduct an RCA in a patientsafety context and further details of these can be found viatheir legacy website4 and in this guide.5. Barrier analysis6. Developing solutions and an action plan for implementation7. Completing a reportRCA tools and techniques featured inthis guide Brainstorming (structured and unstructured) Brainwriting Cause and effect (e.g. fishbone) Change analysis Five whys Mapping tools: narrative chronology, timelines and timeperson grids Nominal group technique Pareto analysis Process mapping Run charts4. http://www.npsa.nhs.uk/6Using root cause analysis techniques in clinical audit Copyright HQIP 2015
Section Two: RCA tools and techniques1. Brainstorming(structured and unstructured)In essence, brainstorming aims to generate as many ideasas possible in the shortest period of time and offers manydifferent approaches. Although we focus on unstructuredand structured brainstorming these techniques should beconsidered alongside brainwriting (see pages 6-8) and nominalgroup technique (see pages 19-21).Definition/explanation of the techniqueThe Oxford English Dictionary defines brainstorming as‘the action or process of making a concerted attemptto solve a problem, usually by group discussion ofspontaneously arising ideas’.Brainstorming is typically carried out in small groups, who withthe support of a facilitator focus on generating ideas or solutionsto a single shared question or problem. It is quick and easy to do,requires minimal resources and involves no statistical analysis,it also has the potential to engage numerous stakeholdersand generate many ideas. Participants in brainstorming areencouraged to be as creative as possible in the knowledge thattheir ideas should not be judged or criticised.1. Unstructured brainstorming: Encourages participants toshare their ideas as they come to mind. All participantswork with the facilitator on the same question/problem butthere is no structure and hence participants will typicallyverbalise their ideas in an unstructured manner. The mainadvantage is that it is quick to conduct and invite membersto offer input, but it can result in one or more person(s)dominating the activity and the facilitator needs to ensureall generated ideas are captured.2. Structured brainstorming: Participants follow rules inorder to make the gathering of ideas more orderly andevenly distributed. As with unstructured brainstormingall participants work with the facilitator on the samequestion/problem but participants are asked one-by-one7Using root cause analysis techniques in clinical auditto verbalise ideas. This round-robin approach continuesuntil the generation of new ideas is exhausted. A structuredbrainstorm will typically take longer to conduct andparticipants may feel under pressure when they are askedfor their ideas in front of others. However, the structuredapproach allows for more equal participation andfacilitators will find it easier to capture all ideas.How brainstorming techniques are used inrelation to patient safety»» As an RCA technique it is typically used to help identify careand service delivery problems»» They may help generate workable solutions to preventfuture incidents from occurring againHow brainstorming techniques can be usedto add value in clinical audit»» They provide a suitable technique for helping clinicalteams to make clinical audit-related decisions; for exampleprioritising clinical audit topics, identifying current barriersto conducting clinical audit and so on»» They can help identify why a clinical audit project has notmet its full potential; for example such techniques canuncover why actions were not implemented, why a re-auditwas not conducted and why the re-audit did not improvepatient care»» They help generate ideas for solving ‘traditional’ clinicalaudit problems; for example effectively involving patientsin clinical audit or raising the profile of clinical audit withsenior managers and board members»» They can assist with generating ideas relating to why specificclinical audit criteria and standards are not being met»» They can assist with generating suggestions in terms of thechanges and actions that should be introduced to improvesub-standard care Copyright HQIP 2015
Example of how brainstorming techniqueshave been used in clinical audit:An interface clinical audit group set up a project toassess the management of patients on lithium therapy.The results of the audit identified sub-standard andpotentially unsafe care with just 59% of patients havingtheir lithium levels checked in the previous three months.In addition, the initial audit identified only 42% of lithiumpatients had their renal function checked and just 60%had their thyroid function checked in accordance withbest practice timeframes.Members of the interface audit group (mostly primarycare professionals and mental health practitioners) helda structured brainstorming session to try and identifypossible changes to implement. One of the ideas generatedwas the creation of a centralised register for lithiumpatients. This formed a pilot scheme that reminded patientsof their tests and coordinated their ongoing treatment.The pilot proved such a success that further funding wasmade available to extend the centralized register across thecounty. The subsequent re-audit results showed significantimprovements across all three criteria with 95% of lithiumlevels checked within three months (up from 59%), 95% ofpatients receiving their renal function check (up from 42%)and 99% of patients receiving their thyroid function check(up from 60%).Further information (full reading list on page 34): National Patient Safety Agency, 2004. Seven steps to patient safety guide (page 157)i National Institute for Health and Care Excellence, 2007. How to change practice guide (pages 16-17)ii NHS Institute for Innovation and Improvement, 2006-2013. Handbook of quality and service improvement tools(pages 254-256)iii8Using root cause analysis techniques in clinical audit Copyright HQIP 2015
2. BrainwritingDefinition/explanation of the techniqueBrainwriting is an alternative method to brainstorming thatadopts a more uniform approach. The fundamental differencebetween brainstorming and brainwriting is that brainstormingencourages participants to verbalise their ideas, whereasbrainwriting involves participants writing their ideas down.Once participants have had time to write their ideas down, thefacilitator collects the ideas and transcribes all unique ideasonto a flipchart for further consideration. The fundamentalbenefit of brainwriting therefore is that all participant’s ideasare submitted anonymously and only the facilitator can see thesource. Like brainstorming, it is designed to generate as manyideas as possible in the shortest period of time.A wide range of brainwriting methods exist, these include:1. Simple brainwriting: The most common approach involvesgroup members writing their own ideas on a post-it note orcard in an agreed time period (for example, five minutes).The facilitator will then take in the ideas and transcribethem into a unique list, discarding duplicates. Afterwards,group members review the list to see if further ideas canbe generated.2. Brainwriting pool: Each person in the group writes downtheir ideas on a post-it note or card and places it in thecentre of the table. Other members of the group can thenpull out ideas pooled in the centre of the table to use asinspiration. By looking at suggestions from others, teammembers can create new ideas, variations or piggyback onto existing ideas.3. Brainwriting 6-3-5: In a nutshell this relates to the rules ofhaving 6 people, each writing 3 ideas in 5 minutes, usingthe table provided (see template 1). At the end of fiveminutes (or when all members have generated three ideas)the worksheets are passed to the person on their right.The process continues until all members have their originalworksheet back. Theoretically 108 ideas should have beengenerated in 30 minutes and these can now be reviewed.9Using root cause analysis techniques in clinical auditThe clear advantages of brainwriting are that all membersare given an equal opportunity to generate ideas and theanonymity of individuals can be maintained, allowing themto be more open. However, the disadvantages of brainwritingare that it takes longer than brainstorming and arguably,lacks spontaneity.It should also be noted that it is possible to conduct abrainwrite without getting all stakeholders together. Forexample, a central facilitator could ask participants to emailideas instead of organising a traditional meeting.How brainwriting techniques are used inrelation to patient safety»» As an RCA technique brainwriting is typically used to helpidentify care and service delivery problems»» They may help generate workable solutions to preventfuture incidents from occurring againHow brainwriting techniques can be used toadd value in clinical audit»» They provide a suitable technique for helping clinicalteams to make clinical audit-related decisions, for exampleprioritising clinical audit topics, identifying current barriersto conducting clinical audit and so on»» They can help identify why a clinical audit project has notmet its full potential; for example using brainwriting touncover why actions were not implemented, why a re-auditwas not conducted or why the re-audit did not improvepatient care»» They help generate ideas for solving ‘traditional’ clinicalaudit problems; for example, involving patients effectivelyin clinical audit or raising the profile of clinical audit withsenior managers and board members»» They can assist with generating ideas relating to why specificclinical audit criteria and standards are not being met»» They can assist with generating suggestions in terms of thechanges and actions that should be introduced to improvesub-standard care Copyright HQIP 2015
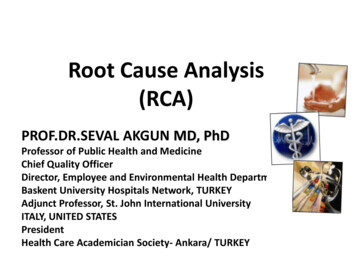
Examples of how brainwriting techniqueshave been used in clinical auditExample 1A large London hospital Trust conducted an annualrecord-keeping audit. The audit team recognised thatalthough considerable time and money were spent onconducting the audit, results changed little from yearto-year and compliance was rarely achieved acrossmany of the key clinical audit standards. In order to helpunderstand why the quality of record keeping in theTrust did not meet best practice, the audit team invitedclinicians to participate in a remote brainwriting activity.Stakeholders were asked to identify why they did notcomplete their records in accordance with the auditstandards by anonymously completing an online survey.The remote brainwriting activity provided key informationthat allowed the Trust to better understand why recordkeeping is sub-standard and subsequently identifiedchanges and actions that could be implemented toaddress the issue.Example 2A GP practice adopted brainwriting methods to enabletheir patient participation group (PPG), to generate a listof possible clinical audit topics for the forthcoming year.The PPG was made up of 10 members from a diverserange of backgrounds with a number of outspokencharacters. It was agreed that the brainwriting approachwould work more effectively than a brainstormingsession, as it would enable participants to share theirideas confidentially. The brainwriting exercise identifiedeight possible clinical audit topics (see also nominalgroup technique within this guide, to understand how thiswas subsequently applied to the brainwriting techniquesto allow democratic section of three topics to audit).Further information (full reading list on page 34): National Patient Safety Agency, 2004. Seven stepsto patient safety guide (page 157)i Chauncey Wilson , Smashing Magazine, 2013.Using brainwriting for rapid idea generationiiTemplate 1: Brainwriting 6-3-5Question/problem:Participant 1Participant 2Participant 3IdeaInstructions: Participants have five minutes to think of threepossible ideas for each question/problem. Ideas are writtendown on the grid in the designated box and after five minutesthe grids are passed on until all group members have submittedtheir ideas.10Using root cause analysis techniques in clinical audit Copyright HQIP 2015
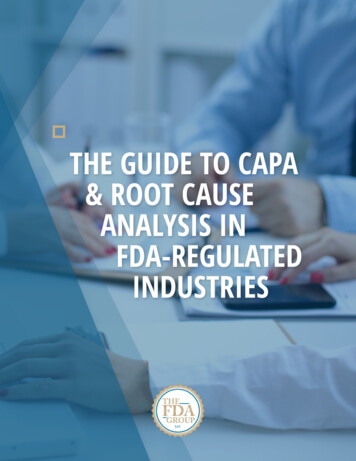
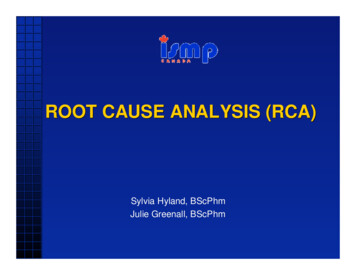
3. Cause and effect diagramDefinition/explanation of the techniqueA cause and effect diagram (also sometimes called a fishboneor Ishikawa diagram) enables teams to visualise the potentialcauses of a particular problem (effect).5The technique was devised by Dr. Karou Ishikawa, a Japanesequality control statistician and was originally used in anindustrial context. Essentially, the cause and effect diagrambreaks the ‘whole’ into ‘parts’, and is particularly helpful inbreaking down the relationship between a problem (effect) andall of the possible factors that are related to it.A cause and effect diagram is often also called a fishbone diagramas the technique creates an illustration that resembles theskeleton of a fish. This is illustrated in the diagram below createdby the National Patient Safety Agency’s diagram below:Diagram 1: Fishbone cause and effect diagramOrganisational andstrategic factorsTask factorsEquipment &resource factorsWorking conditionfactorsIndividual factorsProblem or issue to beexplored: care deliveryproblems/servicedelivery problemsCommunicationfactorsEducation andtraining factorsTeam and socialfactorsPatient factors5. http://www.mindtools.com/pages/article/newTMC 03.htm6. http://www.nrls.npsa.nhs.uk/resources/?entryid45 7560511Using root cause analysis techniques in clinical audit Copyright HQIP 2015
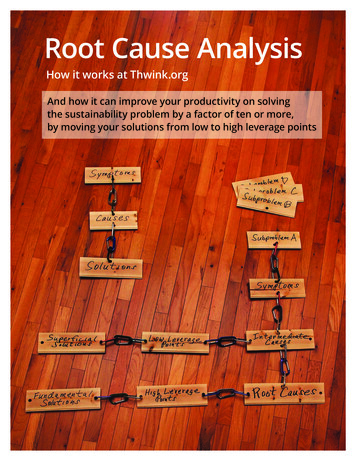
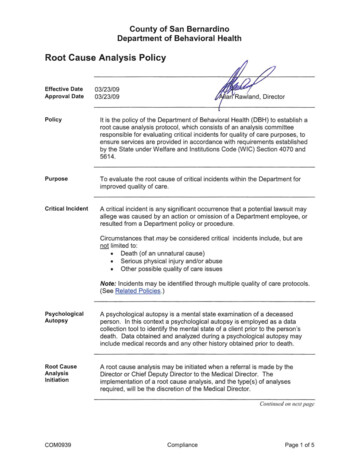
The four stages in creating a causeand effect diagram1. Determine the problem (effect): as the head of the fishshould be the problem you are analysing, which may bereferred to as the effect.2. Determine categories (causes): categories are broadfactors/causes related to the problem/effect. The NPSAdeveloped their cause and effect template specificallyfor healthcare organisations. However, teams canreview this and agree a different set of categories to aidtheir discussions.3. Review each of the categories: each category should bereviewed in turn and considered in relation to the problem(effect). This can be via simple brainstorming techniquesas it is preferable to try and review each category (cause)exhaustively before moving to the next.4. Analyse the diagram: the team using the cause and effectdiagram needs to determine how they will analyse theirdiscussions. Two possible approaches to this are:a. Where an agreed template for the cause and effectdiagram has been used, for example NPSA template the diagram can be analysed by reviewing groupingsof potential causes around each category. Wheremore causes are noted under a particular categorythis may indicate more impact and hence a key rootcause to the problem/effect. In turn this categoryand its associated causes can be considered forappropriate action planning.b. When using a cause and effect diagram withoutpre-determined categories the weight of the impactof the causes can be measured in the size of the‘bones’. For instance the larger bones closer to thehead of the fish may represent a bigger impact,while small bones further away from the head havea smaller impact. Or as above, the causes with themost grouping may indicate most impact and can beidentified as the foundation for action planning.12Using root cause analysis techniques in clinical auditHow cause and effect diagrams are used inrelation to patient safetyThe cause and effect diagram is typically used to separate andcategorise possible causes of a problem or incident. The focusrelates to the content of the problem/incident rather thanthe history of the problem (the history of the incident is dealtwith during the mapping phase). Analysis of the diagram mayenable teams to understand the root cause/s of the problem orincident with the overall aim to ensure that appropriate actionsare implemented.How cause and effect diagrams can be usedto add value to clinical audit»» In the context of clinical audit results, the diagrams canassist in understanding why a non-compliant result wasreported. By utilising the cause and effect diagram theteam review the clinical audit criteria (the effect) in relationto possible reasons (causes) why the level of performancewas below compliance levels»» To review areas that are problematic within the clinicalaudit; for example engagement of junior doctors, patientand service user involvement or utilising national auditresults to enable local improvementsHow cause and effect techniques have beenused in clinical audit»» The cause and effect fishbone diagram (Diagram 2) wasused by a team of clinical audit professionals to reviewthe engagement of junior doctors in the clinical auditprocess. The exercise demonstrated a wide variety ofcauses leading to a lack of engagement of junior doctors,and highlighted the need for appropriate action planning inrelation to clinical audit training and associated support forjunior doctors Copyright HQIP 2015
Diagram 2: Cause and effect diagram reviewing the engagement of Junior Doctors in clinicalaudit processEquipmentIndividual FactorsTime Only allowed a set number of casenotes in some organisations Lack of interest in available topics(resistance to tackle some areas) Competing priorities No space to undertake the work Don’t get to see outcome of changesimplemented so don’t see qualityimprovements. This undermines thevalue of understanding Junior Doctors may leave theirclinical audit until later in theirrotation – placing pressure onthemselves and the CA team Poor experience leads to poorquality audits No allocated time for task Limited or no access to previousclinical audits undertaken Busy shift patternsJunior Doctor engagement Different organisational structuresfor clinical audit e.g. auditregistration requirements Lack of direction Is training at the right time of day? Engagement of senior staff/clinicians Is the content of training right? Access to case notes Given as a task to some JuniorDoctors rather than the individualchoosing to participate Maybe little or no clinical auditteam support for Junior Doctors asorganisation focuses on nationalaudit programme Not trained in how to write agood report Analysis skills trainingmay be required Advertise the clinical audit teamto determine what help can andcannot be providedOrganisations Problem caused by junior doctorsbeing able to set criteria andstandardsTeam FactorsTrainingFurther information (full reading list on page 34): NHS Institute for Innovation and Improvement, 2006-13. Handbook of quality and service improvement tools(pages 44-47)i National Patient Safety Agency, 2010. RCA tools: analysing to identify contributory factors and root causesii Institute for Healthcare Improvement, 2015. Cause and effect diagramiii13Using root cause analysis techniques in clinical audit Copyright HQIP 2015
4. Change analysisDefinition/explanation of the techniqueChange analysis is a very simple approach that essentiallycompares what did happen with what should have happened. Itis typically used to identify divergences from an agreed processto help identify why a problem/failure occurred.The four stages involved in conductingchange analysis1. Map the perfect process: Use the process mappingtechnique to effectively create a fault-free, step-by-stepexemplar model of what should happen. The processshould be as detailed as possible.2. Compare: Make a comparison of what actually happenedagainst the perfect process. This will help to identifyareas of divergence, i.e. indicating where appropriate/best practice was not followed. All the divergences shouldbe listed.3. Prioritise: If more than one divergence occurred then theseshould be prioritised, i.e. consideration given to whichdivergence had the greatest impact.4. Resolve: Each divergence needs to be assessed tounderstand why the perfect process was not adopted.Changes may be required and or new barriers andprocedures put in place to ensure that similar divergencesdo not occur again.14Using root cause analysis techniques in clinical auditHow change analysis is used in relation topatient safety»» Within RCA, change analysis is often used to help identifycare and service delivery problems»» They often help uncover the causes of an incident»» They may help generate workable solutions to preventincidents from occurring again, particularly in relation toidentifying barriers that need to be implemented or newsystems of workingHow change analysis techniques can be usedto add value in clinical auditClinical audit compares actual care and service delivery to bestpractice and therefore is similar to change analysis in manyrespects. Clinic
What is root cause analysis (RCA) 6 Understanding the RCA process 6 RCA tools and techniques featured in this guide 6 Section two: RCA tools and techniques 7 1. Brainstorming (structured and unstructured) 7 - Definition/explanation of the technique 7 - How brainstorming techniques are used in relation to patient safety 7